
Abstract
Background
Negative margins are associated with decreased local recurrence after lumpectomy for breast cancer. A 2nd operation for re-excision of positive margins is required with rates varying from 15 to 50%. At our institution we routinely use frozen-section analysis of all margins to minimize rates of 2nd operations. The aim of this study was to evaluate the cost/benefit of routine frozen-section analysis.
Methods
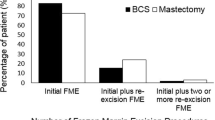
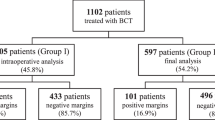
A decision tree was built to compare 2 strategies: (A) lumpectomy without frozen section and a 2nd operation for positive margin(s) versus (B) lumpectomy with intraoperative frozen-section analysis and a 2nd operation for positive margin(s). For strategy A the rate of positive margins and reoperation were varied from 15 to 50%. For strategy B, a 2nd operation rate of 3% was used. Review of our institutional experience demonstrates an intraoperative re-excision of at least 1 margin in 57% of cases performed with frozen-section support.
Results
The cost to provider (i.e., institution) per patient resected to negative margins for strategy A ranged from $4835 to $6306. Average weighted cost of strategy B was $5708. Strategy B was less expensive when the reoperation rate was above 36%. The cost to payor (i.e., Medicare) for strategy A ranged from $3577 to $4665. Average weighted cost for strategy B was $3913. Strategy B was less expensive when the re-excision rate was above 26%.
Conclusion
Routine use of frozen-section analysis of lumpectomy margins decreases reoperation rates for margin control; therefore, the cost to provider and payor can be cost effective.



Similar content being viewed by others

References
Kurtz JM, Jacquemier J, Amalric R, Brandone H, Ayme Y, Hans D, et al. Breast-conserving therapy for macroscopically multiple cancers. Ann Surg. 1990;212:38–44.
Jobsen JJ, van der Palen J, Ong F, Meerwaldt JH. The value of a positive margin for invasive carcinoma in breast-conservative treatment in relation to local recurrence is limited to young women only. Int J Radiat Oncol Biol Phys. 2003;57:724–31.
Arriagada R, Le MG, Rochard F, Contesso G. Conservative treatment versus mastectomy in early breast cancer: patterns of failure with 15 years of follow-up data. Institut Gustave-Roussy Breast Cancer Group. J Clin Oncol. 1996;14:1558–64.
Fisher B, Anderson S, Bryant J, Margolese RG, Deutsch M, Fisher ER, et al. Twenty-year follow-up of a randomized trial comparing total mastectomy, lumpectomy, and lumpectomy plus irradiation for the treatment of invasive breast cancer. N Engl J Med. 2002;347:1233–41.
Singletary SE. Surgical margins in patients with early-stage breast cancer treated with breast conservation therapy. Am J Surg. 2002;184:383–93.
Bedwinek JM, Brady L, Perez CA, Goodman R, Kramer S, Grundy G. Irradiation as the primary management of stage I and II adenocarcinoma of the breast: analysis of the RTOG breast registry. Cancer Clin Trials. 1980;3:11–8.
Park CC, Mitsumori M, Nixon A, Recht A, Connolly J, Gelman R, et al. Outcome at 8 years after breast-conserving surgery and radiation therapy for invasive breast cancer: influence of margin status and systemic therapy on local recurrence. J Clin Oncol. 2000;18:1668–75.
Freedman G, Fowble B, Hanlon A. Patients with early stage invasive cancer with close or positive margins treated with conservative surgery and radiation have an increased risk of breast recurrence that is delayed by adjuvant systemic therapy. Int J Radiat Oncol Biol Phys. 1999;44:1005–15.
Singh M, Singh G, Hogan KT, Atkins KA, Schroen AT. The effect of intraoperative specimen inking on lumpectomy re-excision rates. World J Surg Oncol. 2010;8:4.
Margenthaler JA, Gao F, Klimberg VS: Margin index: a new method for prediction of residual disease after breast-conserving surgery. Ann Surg Oncol. 2010;17:2696–701.
Balch GC, Mithani SK, Simpson JF, Kelley MC. Accuracy of intraoperative gross examination of surgical margin status in women undergoing partial mastectomy for breast malignancy. Am Surg. 2005;71:22–7.
Thompson M, Henry-Tillman R, Margulies A, Thostenson J, Bryant-Smith G, Fincher R, et al. Hematoma-directed ultrasound-guided (HUG) breast lumpectomy. Ann Surg Oncol. 2007;14:148–56.
Fukamachi K, Ishida T, Usami S, Takeda M, Watanabe M, Sasano H, et al. Total-circumference intraoperative frozen section analysis reduces margin-positive rate in breast-conservation surgery. Jpn J Clin Oncol. 2010;40:513–20.
Malik HZ, George WD, Mallon EA, Harnett AN, Macmillan RD, Purushotham AD. Margin assessment by cavity shaving after breast-conserving surgery: analysis and follow-up of 543 patients. Eur J Surg Oncol. 1999;25:464–9.
Janes SE, Stankhe M, Singh S, Isgar B. Systematic cavity shaves reduces close margins and re-excision rates in breast conserving surgery. Breast. 2006;15:326–30.
Jakub JW, Gray RJ, Degnim AC, Boughey JC, Gardner M, Cox CE. Current status of radioactive seed for localization of non palpable breast lesions. Am J Surg. 2010;199:522–8.
Gray RJ, Pockaj BA, Karstaedt PJ, Roarke MC. Radioactive seed localization of nonpalpable breast lesions is better than wire localization. Am J Surg. 2004;188:377–80.
Lovrics PJ, Hodgson N, Gohla G, Boylan C, Goldsmith CH, McCready D, et al. Radioguided seed localization of nonpalpable invasive and in situ breast cancers: a prospective, randomized trial. Ann Surg Oncol. 2011;18:S33; doi:10.1245/s10434-011-1552-3.
Turnbull L, Brown S, Harvey I, Olivier C, Drew P, Napp V, et al. Comparative effectiveness of MRI in breast cancer (COMICE) trial: a randomised controlled trial. Lancet. 2010;375:563–71.
Klimberg VS, Westbrook KC, Korourian S. Use of touch preps for diagnosis and evaluation of surgical margins in breast cancer. Ann Surg Oncol. 1998;5:220–6.
Bakhshandeh M, Tutuncuoglu SO, Fischer G, Masood S. Use of imprint cytology for assessment of surgical margins in lumpectomy specimens of breast cancer patients. Diagn Cytopathol. 2007;35:656–9.
Wilson LB. A method for the rapid preparation of fresh tissues for the microscope. JAMA. 1905;45:1737.
Ferreiro JA, Myers JL, Bostwick DG. Accuracy of frozen section diagnosis in surgical pathology: review of a 1-year experience with 24,880 cases at Mayo Clinic Rochester. Mayo Clin Proc. 1995;70:1137–41.
Ferreiro JA, Gisvold JJ, Bostwick DG. Accuracy of frozen-section diagnosis of mammographically directed breast biopsies. Results of 1,490 consecutive cases. Am J Surg Pathol. 1995;19:1267–71.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Osborn, J.B., Keeney, G.L., Jakub, J.W. et al. Cost-Effectiveness Analysis of Routine Frozen-Section Analysis of Breast Margins Compared with Reoperation for Positive Margins. Ann Surg Oncol 18, 3204–3209 (2011). https://doi.org/10.1245/s10434-011-1956-0
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-011-1956-0