
Abstract
Background
The survival benefit of sentinel node biopsy is still controversial. The aim of our study was to assess the overall survival (OS; calculated both from the date of primary tumor excision and lymph node dissection) data from two large groups of AJCC 2002 stage-III cutaneous melanoma patients—after completion lymph node dissection (CLND after positive sentinel node biopsy) and after therapeutic LND (TLND for clinically/cytologically detected regional lymph node metastases).
Materials and Methods
We analyzed the outcomes for 544 consecutive patients, who underwent CLND (47.4%; 258 patients) or TLND (52.6%; 286 patients) at one institution between December 1994 and January 2005. There were no significant differences between the two groups in terms of age and gender distribution and in the parameters of the primary tumor. Median follow-up time was 36 months (range 6–110 months).
Results
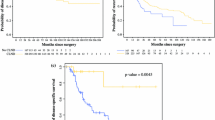
We found no significant differences in OS (from the date of primary tumor excision) between CLND and TLND patients in the groups with primary tumor thicknesses of 1.0 mm or less or greater than 4.0 mm (pT1 and pT4); however, in patients with thicknesses greater than 1.0 mm and 4.0 mm or less (in subgroups pT2 and pT3), we found significantly better OS for CLND than for TLND patients—CLND: median OS not reached, 5-year OS was 57.2% (95%CI: 44.4–70.1%); TLND: median OS 42.1 months, 5-year OS was 37.9% (95%CI: 26.5–49.2%) (P = 0.0006). In the entire CLND and TLND groups, the median OS and 5-year OS rates were 60.5 months and 52.5% (95%CI: 45.6–61.5%) and 38.2 months and 39.5% (95%CI: 32.7–46.5%), respectively. Based on multivariate analysis, we have found that in the CLND group the important factors negatively influencing OS (from the date of lymphadenectomy) are: male gender, features of primary tumor (higher Breslow thickness and presence of ulceration) and features of nodal metastases (extracapsular invasion and number of involved nodes). In the TLND group, however, the negative prognostic factors are: male gender and features of nodal metastases (extracapsular invasion and number of involved nodes) without the impact of primary tumor characteristics.
Conclusion
The results of the study demonstrate that the survival benefit after positive sentinel node biopsy with subsequent CLND is probably limited only to the subgroup of patients with primary tumor thicknesses not larger than 4 mm and not less than 1 mm when compared with lymph node dissection of palpable nodes. The primary tumor features have no impact on survival after lymphadenectomy performed for clinically involved nodes.






Similar content being viewed by others

References
Veronesi U, Adamus J, Bandiera DC, et al. Inefficacy of immediate node dissection in stage 1 melanoma of the limbs. N Engl J Med 1977; 297:627–30.
Balch CM, Soong S, Ross MI, et al. Long-term results of a multi-institutional randomized trial comparing prognostic factors and surgical results for intermediate thickness melanomas (1.0 to 4.0 mm). Intergroup Melanoma Surgical Trial. Ann Surg Oncol 2000; 7:87–97.
Cascinelli N, Morabito A, Santinami M, et al. Immediate or delayed dissection of regional nodes in patients with melanoma of the trunk: a randomised trial. WHO Melanoma Programme. Lancet 1998; 351:793–6.
Veronesi U, Adamus J, Bandiera DC, et al. Delayed regional lymph node dissection in stage I melanoma of the skin of the lower extremities. Cancer 1982; 49:2420–30.
Morton DL, Wen DR, Wong JH, et al. Technical details of intraoperative lymphatic mapping for early stage melanoma. Arch Surg 1992; 127:392–9.
Cascinelli N, Belli F, Santinami M, et al. Sentinel lymph node biopsy in cutaneous melanoma: the WHO Melanoma Program experience. Ann Surg Oncol 2000; 7:469–74.
Cascinelli N. WHO declares lymphatic mapping to be standard of care for melanoma. Oncology 1999; 13:288.
Balch CM, Buzaid AC, Soong SJ, et al. Final version of the American Joint Committee on Cancer staging system for cutaneous melanoma. J Clin Oncol 2001; 19:3635–48.
Balch CM, Soong SJ, Gershenwald JE, et al. Prognostic factors analysis of 17,600 melanoma patients: validation of the American Joint Committee on Cancer melanoma staging system. J Clin Oncol 2001; 19:3622–34.
Nowecki ZI, Rutkowski P, Nasierowska-Guttmejer A, et al. Sentinel lymph node biopsy in melanoma patients with clinically negative regional lymph nodes–one institution’s experience. Melanoma Res 2003; 13:35–43.
Vuylsteke RJ, van Leeuwen PA, Statius Muller MG, et al. Clinical outcome of stage I/II melanoma patients after selective sentinel lymph node dissection: long-term follow-up results. J Clin Oncol 2003; 21:1057–65.
Gershenwald JE, Thompson W, Mansfield PF, et al. Multi-institutional melanoma lymphatic mapping experience: the prognostic value of sentinel lymph node status in 612 stage I or II melanoma patients. J Clin Oncol 1999; 17:976–83.
Thompson JF, Shaw HW. Sentinel node mapping for melanoma: results of trials and current applications. Surg Oncol Clin N Am 2007; 16:35–54.
McMasters KM, Reintgen DS, Ross MI, et al. Sentinel lymph node biopsy for melanoma: controversy despite widespread agreement. J Clin Oncol 2001; 19:2851–5.
Morton DL, Thompson JF, Cochran AJ, et al. Sentinel-node biopsy or nodal observation in melanoma. N Engl J Med 2006; 355:1307–17.
Rutkowski P, Nowecki ZI, Zurawski Z, et al. In-transit/local recurrences in melanoma patients after sentinel node biopsy and therapeutic lymph node dissection. Eur J Cancer 2006; 42:159–64.
van Akkooi AC, de Wilt JH, Verhoef C, et al. High positive sentinel node identification rate by EORTC melanoma group protocol. Prognostic indicators of metastatic patterns after sentinel node biopsy in melanoma. Eur J Cancer 2006; 42:372–80.
Statius Muller MG, van Leeuwen PA, de Lange-De Klerk ES, et al. The sentinel lymph node status is an important factor for predicting clinical outcome in patients with Stage I or II cutaneous melanoma. Cancer 2001; 91:2401–8.
Karakousis CP. Therapeutic node dissections in malignant melanoma. Semin Surg Oncol 1998; 14:291–301.
Eggermont AMM, Suciu S, MacKie R, et al. Post-surgery adjuvant therapy with intermediate doses of interferon alfa 2b versus observation in patients with stage IIb/III melanoma (EORTC 18952): randomized controlled trial. Lancet 2005; 366:1189–96.
Eggermont AMM, Gore M. Randomized adjuvant therapy trials in melanoma: surgical and systemic. Semin Oncol 2007; 34:509–15.
Balch CM, Soong S-J, Desmond R. In reply. J Clin Oncol 2005; 23:9428.
Berd D, Mastrangelo MJ, Sato T. Calculation of survival of patients with stage III melanoma. J Clin Oncol 2005; 23:9427.
Petro A, Schwartz J, Johnson T. Current melanoma staging. Clin Dermatol 2004; 22:223–7.
Leiter U, Meier F, Schittek B, et al.. The natural course of cutaneous melanoma. J Surg Oncol 2004; 86:172–8.
Kretschmer L, Preusser KP, Marsch WC, et al. Prognostic factors of overall survival in patients with delayed lymph node dissection for cutaneous malignant melanoma. Melanoma Res 2000; 10:483–9.
Meier F, Will S, Ellwanger U, et al. Metastatic pathways and time courses in the orderly progression of cutaneous melanoma. Br J Dermatol 2002; 147:62–70.
Aloia TA, Gershenwald JE, Andtbacka RH, et al. Utility of computed tomography and magnetic resonance imaging staging before completion lymphadenectomy in patients with sentinel lymph node-positive melanoma. J Clin Oncol 2006; 24:2858–65.
Gold JS, Jaques DP, Busam KJ, et al. Yield and predictors of radiologic studies for identifying distant metastases in melanoma patients with a positive sentinel lymph node biopsy. Ann Surg Oncol 2007; 14:2133–40.
Kretschmer L, et al. Patients with lymphatic metastasis of cutaneous melanoma benefit from lymphonodectomy and early excision of their nodal disease. Eur J Cancer 2004; 40:212–8.
Retsasa S, Mastrangelo MJ. Reflecting on the 2001 American Joint Committee on Cancer Staging System for Melanoma. Semin Oncol 2007; 34:491–7.
Cascinelli N, Bombardieri E, Bufalino R, et al. Sentinel and nonsentinel node status in stage IB and II melanoma patients: two-step prognostic indicators of survival. J Clin Oncol 2006; 24:4464–71.
van Akkooi AC, Bouwhuis MG, van Geel AN, et al. Morbidity and prognosis after therapeutic lymph node dissections for malignant melanoma. Eur J Surg Oncol 2007; 33:102–8.
Meyer T, Merkel S, Göhl J, et al. Lymph node dissection for clinically evident lymph node metastases of malignant melanoma. Eur J Surg Oncol 2002; 28:424–30.
Messaris GE, Konstadoulakis MM, Ricaniadis N, et al. Prognostic variables for patients with stage III malignant melanoma. Eur J Surg 2000; 166:233–9.
Hughes TMD, A’Hern RP, Thomas JM. Prognosis and surgical management of patients with palpable inguinal lymph node metastases from melanoma. Br J Surg 2000; 87:892–901.
van Akkooi AC, Bouwhuis MG, de Wilt JH, et al. Multivariable analysis comparing outcome after sentinel node biopsy or therapeutic lymph node dissection in patients with melanoma. Br J Surg 2007; 94:1293–9.
Badgwell B, Xing Y, Gershenwald JE, et al. Pelvic lymph node dissection is beneficial in subsets of patients with node-positive melanoma. Ann Surg Oncol 2007; 14:2867–75.
Karakousis CP, Driscoll DL. Positive deep nodes in the groin and survival in malignant melanoma. Am J Surg 1996; 171:421–2.
Doubrovsky A, de Wilt JHW, Scolyer RA, et al. Sentinel node biopsy provides more accurate staging than elective lymph node dissection In patients with cutaneous melanoma. Ann Surg Oncol 2004; 11:829–36.
Balch CM, Cascinelli N. Editorials: sentinel-node in melanoma. N Engl J Med 2006; 355:1370–2
Morton DL, Hoon DS, Cochran AJ, et al. Lymphatic mapping and sentinel lymphadenectomy for early-stage melanoma: therapeutic utility and implications of nodal microanatomy and molecular staging for improving the accuracy of detection of nodal micrometastases. Ann Surg 2003; 238:538–50.
Essner R, Conforti A, Kelley MC, et al. Efficacy of lymphatic mapping, sentinel lymphadenectomy, and selective complete lymph node dissection as a therapeutic procedure for early-stage melanoma. Ann Surg Oncol 1999; 6:442–9.
Roka F, Kittler H, Cauzig P, et al. Sentinel node status in melanoma patients is not predictive for overall survival upon multivariate analysis. Br J Cancer 2005; 92:662–7.
Gutzmer R, Al Ghazal M, Geerlings H, et al. Sentinel node biopsy in melanoma delays recurrence but does not change melanoma-related survival: a retrospective analysis of 673 patients. Br J Dermatol 2005;153:1137–41.
Rutkowski P, Nowecki ZI, Nasierowska-Guttmejer A, et al. Lymph node status and survival in cutaneous malignant melanoma–sentinel lymph node biopsy impact. Eur J Surg Oncol 2003, 29:611–8.
Carlson GW, Murray DR, Lyles RH, et al. The amount of metastatic melanoma in a sentinel lymph node: does it have prognostic significance? Ann Surg Oncol 2003; 10:575–81.
Scheri RP, Essner R, Turner RR, et al. Isolated tumor cells in the sentinel node affect long-term prognosis of patients with melanoma. Ann Surg Oncol 2007; 14:2861–6.
van Akkooi AC, de Wilt JH, Verhoef C, et al. Clinical relevance of melanoma micrometastases (<0.1 mm) in sentinel nodes: are these nodes to be considered negative? Ann Oncol 2006; 17:1578–85.
van Akkooi AC, Nowecki ZI, Voit C, et al. Prognosis depends on micro-anatomic patterns of melanoma micrometastases within the sentinel node (SN). A multicenter study in 388 SN positive patients. Eur J Cancer - Supplements 2007; 5:397:abstract 7006
Gershenwald JE, Mansfield PF, Lee JF, et al. Role for lymphatic mapping an sentinel lymph node biopsy in patients with thick (≥4 mm) primary melanoma. Ann Surg Oncol 2000; 7:160–5.
Thomas JM. Prognostic false-positivity of the sentinel node in melanoma. Nat Clin Pract Oncol 2008; 5:18–23.
Acknowledgements
We thank M. Rosinska, M.D., for statistical advice and M. Symonides, M.D., PhD, for linguistic assistance.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Nowecki, Z.I., Rutkowski, P. & Michej, W. The Survival Benefit to Patients with Positive Sentinel Node Melanoma After Completion Lymph Node Dissection May Be Limited to the Subgroup with a Primary Lesion Breslow Thickness Greater Than 1.0 and Less Than or Equal to 4 mm (pT2–pT3). Ann Surg Oncol 15, 2223–2234 (2008). https://doi.org/10.1245/s10434-008-9965-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-008-9965-3