
Abstract
Background
Routine axillary lymph node dissection (ALND) after selective sentinel lymphadenectomy (SSL) in the treatment of breast cancer remains controversial. We sought to determine the need for routine ALND by exploring the relationship between sentinel lymph node (SLN) and non-SLN (NSLN) status. We also report our experience with disease relapse in the era of SSL and attempt to correlate this with SLN tumor burden.
Methods
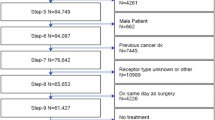
This was a retrospective study of 390 patients with invasive breast cancer treated at a single institution who underwent successful SSL from November 1997 to November 2002.
Results
Of the 390 patients, 115 received both SSL and ALND. The percentage of additional positive NSLNs in the SLN-positive group (34.2%) was significantly higher than in the SLN-negative group (5.1%; P = .0004). The SLN macrometastasis group had a significantly higher rate of positive NSLNs (39.7%) compared with the SLN-negative group (5.1%; P = .0001). Sixteen patients developed recurrences during follow-up, including 6.1% of SLN-positive and 3.3% of SLN-negative patients. Among the SLN macrometastasis group, 8.7% had recurrence, compared with 2.2% of SLN micrometastases over a median follow-up period of 31.1 months. One regional failure developed out of 38 SLN-positive patients who did not undergo ALND.
Conclusions
ALND is recommended for patients with SLN macrometastasis because of a significantly higher incidence of positive NSLNs. Higher recurrence rates are also seen in these patients. However, the role of routine ALND in patients with a low SLN tumor burden remains to be further determined by prospective randomized trials.

Similar content being viewed by others

References
Ivens D, Hoe A, Podd TJ, Hamilton CR, Taylor I, Royle GT. Assessment of morbidity from complete axillary dissection. Br J Cancer 1992;66:136–8
Hladiuk M, Huchcroft S, Temple W, Schnurr BE. Arm function after axillary dissection for breast cancer: a pilot study to provide parameter estimates. J Surg Oncol 1992;50:47–52
Greco M, Agresti R, Cascinelli N, et al. Breast cancer patients treated without axillary surgery: clinical implications and biologic analysis. Ann Surg 2000;232:1–7
Cody HS III. Clinical aspects of sentinel node biopsy. Breast Cancer Res 2001;3:104–8
Leong SP, Morita ET, Treseler PA, Wong JH. Multidisciplinary approach to selective sentinel lymph node mapping in breast cancer. Breast Cancer 2000;7:105–13
Treseler PA, Tauchi PS. Pathologic analysis of the sentinel lymph node. Surg Clin North Am 2000;80:1695–719
Nemoto T, Vana J, Bedwani RN, Baker HW, McGregor FH, Murphy GP. Management and survival of female breast cancer: results of a national survey by the American College of Surgeons. Cancer 1980;45:2917–24
Carter C, Allen C, Henson DE. Relation of tumor size, lymph node status, and survival in 24,740 breast cancer cases. Cancer 1989;63:181–7
Fisher B, Wolmark N, Bauer M, Redmond C, Gebhardt M. The accuracy of clinical nodal staging and of limited axillary dissection as a determinant of histologic nodal status in carcinoma of the breast. Surg Gynecol Obstet 1981;152:765–72
Ross MI. Sentinel node dissection in early-stage breast cancer: ongoing prospective randomized trials in the USA. Ann Surg Oncol 2001;8(9 Suppl):77S–81S
Wong SL, Edwards MJ, Chao C, et al. University of Louisville Breast Cancer Sentinel Lymph Node Study Group. Predicting the status of the nonsentinel axillary nodes. A multicenter study. Arch Surg 2001;136:563–8
Chu KU, Turner RR, Hansen NM, Brennan MB, Bilchik A, Giuliano AE. Do all patients with sentinel node metastasis from breast carcinoma need complete axillary node dissection? Ann Surg 1999;229:536–41
Turner RR, Chu KU, Qi K, et al. Pathologic features associated with nonsentinel lymph node metastases in patients with metastatic breast carcinoma in a sentinel lymph node. Cancer 2000;89:574–81
Viale G, Maiorano E, Mazzarol G, et al. Histologic detection and clinical implications of micrometastases in axillary sentinel lymph nodes for patients with breast carcinoma. Cancer 2001;92:1378–84
Giuliano AE, Haigh PI, Brennan MB, et al. Prospective observational study of sentinel lymphadenectomy without further axillary dissection in patients with sentinel node-negative breast cancer. J Clin Oncol 2000;18:2553–9
Veronesi U, Galimberti V, Zurrida S, et al. Sentinel lymph node biopsy as an indicator for axillary dissection in early breast cancer. Eur J Cancer 2001;37:454–8
Schrenk P, Hatzl-Griesenhofer M, Shamiyeh A, Waynad W. Follow-up of sentinel node negative breast cancer patients without axillary lymph node dissection. J Surg Oncol 2001;77:165–70
Roumen RM, Kuijt GP, Liem IH, van Beek MW. Treatment of 100 patients with sentinel node-negative breast cancer without further axillary dissection. Br J Surg 2001;88:1639–43
Chung MA, Steinhoff MM, Cady B. Clinical axillary recurrence in breast cancer patients after a negative sentinel node biopsy. Am J Surg 2002;184:310–4
Blanchard DK, Donohue JH, Reynolds C, Grant CS. Relapse and morbidity in patients undergoing sentinel lymph node biopsy alone or with axillary dissection in breast cancer. Arch Surg 2003;138:482–8
Reitsamer R, Peintinger F, Prokop E, Rettenbacher L, Menzel C. 200 sentinel lymph node biopsies without axillary lymph node dissection—no axillary recurrences after a 3-year follow-up. Br J Cancer 2004;90:1551–4
Badgwell BD, Povoski SP, Abdessalam SF, et al. Patterns of recurrence after sentinel lymph node biopsy for breast cancer. Ann Surg Oncol 2003;10:376–80
Guenther JM, Hansen NM, DiFronzo LA, et al. Axillary dissection is not required for all patients with breast cancer and positive sentinel nodes. Arch Surg 2003;138:52–6
Author information
Authors and Affiliations
Corresponding author
Additional information
Published by Springer Science+Business Media, Inc. © 2005 The Society of Surgical Oncology, Inc.
An erratum to this article is available at http://dx.doi.org/10.1245/ASO.2005.08.513.
Rights and permissions
About this article
Cite this article
Fan, YG., Tan, YY., Wu, CT. et al. The Effect of Sentinel Node Tumor Burden on Non–Sentinel Node Status and Recurrence Rates in Breast Cancer. Ann Surg Oncol 12, 705–711 (2005). https://doi.org/10.1245/ASO.2005.08.020
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1245/ASO.2005.08.020