
Abstract
Glucagon Like Peptide 2 (GLP-2) has been proposed as an important regulatory hormone in nutrient absorption. The present study was conducted in human infants with intestinal dysfunction undergoing surgery, correlating postprandial GLP-2 levels with intestinal length, nutrient absorption, and patient outcome. We hypothesized that GLP-2 levels would be inversely related to nutrient absorption; we further hypothesized that post prandial GLP-2 levels would be predictive of the ability to wean patients from total parenteral nutrition (TPN), and tolerance of enteral feeding. Infants prospectively identified with nutrient malabsorption following intestinal surgery were monitored and after initiation of feeds GLP-2 levels were measured in the fed state. Intestinal length was recorded intraoperatively and nutrient absorption was quantified using both a balance study, and carbohydrate probe method. 12 infants had GLP-2 levels successfully measured; two patients had repeated studies. Average gestational age was 32.7 ± 3.4 wk, age at testing was 1.7 ± 1.4 mo and average weight was 3.5 ± 1.1 kg. Causes of intestinal loss were necrotizing enterocolitis, atresia and volvulus. Five patients had severe short bowel syndrome (<50% of normal small intestinal length), 3 died. GLP-2 levels were best correlated with residual small intestinal length (r2 = 0.75). Correlations with total intestinal length including colon were less significant; residual colon appeared to not contribute to measurable GLP-2 production. GLP-2 levels were well correlated with tolerance of enteral feeds. Contradicting the initial hypothesis, GLP-2 levels were directly correlated with nutrient absorptive capacity (correlation with fat absorption: r2 = 0.72, carbohydrate = 0.50 and protein = 0.54 respectively). There were no apparent changes in GLP-2 levels with gestational or postnatal age. As a corollary to the correlation with bowel length, a postprandial level of 15 pmol/L appeared to be discriminatory; infants with postprandial GLP-2 levels of > 15 pmol/L were able to be weaned from total parenteral nutrition, while 3 of 4 infants who had GLP-2 levels less than 15 could not be weaned by one year. These results show that in infants with intestinal dysfunction, GLP-2 levels are correlated with residual small bowel length and nutrient absorption, and may be predictive of outcome. In contrast to adults with intact colon and SBS, infants with SBS and intact colon do not appear able to produce GLP-2 in response to feeding stimulation. Further studies are suggested to examine the ontogeny of the GLP-2 axis and the possible therapeutic role of GLP-2 supplementation.
Similar content being viewed by others


Main
Nutrient malabsorption due to inadequate intestinal surface area, or short bowel syndrome (SBS) is a difficult clinical problem. This is especially challenging in the pediatric population, where it is relatively common, and supportive therapy is frequently complicated by the development of total parenteral nutrition (TPN) induced cholestasis (1–3). At present, treatment in human infants is primarily supportive while the process of intestinal adaptation, or up-regulation of nutrient absorption capacity, occurs (2,3). The description of the intestinal trophic effects of Glucagon Like Peptide 2 (GLP-2) has renewed optimism that we may be able to modify or accelerate this process of adaptation (4–6). However, the physiology of GLP-2 release in humans is poorly understood (7). The limited animal studies and human data available support the concept that GLP-2 acts as a marker of nutrient ingestion and malabsorption. The primary signal for GLP-2 release appears to be the ingestion of a meal, which within minutes triggers the release of GLP-2 (with GLP-1), from the L-cells of the distal ileum and colon (7–12). This is likely a neuronal – hormonal reflex, triggered by the presence of fat in the proximal bowel (13). These hormones then feed back proximally, altering intestinal motility patterns, up-regulating acute and chronic nutrient absorptive capacity (4,14) and potentially acting centrally as a satiety signal (15). In conditions of inadequate nutrient absorptive capacity, the presence of nonabsorbed nutrients within the intestinal lumen may trigger GLP-2 release directly (16). The data from adult humans with SBS would fit with this theoretical framework, with evidence of increased GLP-2 release in adults with remnant colon, and reduced GLP-2 release if no colon is present (17,18). There is evidence of changing GLP-2 signaling patterns during intestinal development, as well as previous studies relating to the release of enteroglucagon (GLP-2) (19–22). However, at present, there are no studies examining GLP-2 release patterns in human infants.
Accordingly, the present study was undertaken to describe the relationship between postprandial levels of GLP-2 in human infants with bowel dysfunction or SBS. We hypothesized that GLP-2 release would be stimulated by the presence of unabsorbed nutrients within the distal small bowel and colon, and so GLP-2 levels in the early postoperative adaptive phase would be correlated with residual total bowel length, and would be inversely correlated with nutrient absorption, as we have demonstrated in postresection animal models (9,10). We also examined the relationship between gestational age and GLP-2 production. Finally, we hypothesized that below a certain level of GLP-2 production, intestinal adaptation would not occur. Therefore, we compared postprandial GLP-2 levels in the patients who died of TPN complications, or remained TPN dependent for more than a year, to the patients who were able to be converted to enteral feeds by one year of follow-up.
METHODS
Patients.
Infants requiring bowel resection with an anticipated TPN requirement of greater than two weeks, or infants with SBS (residual small intestinal length less than 50% of predicted for gestational age) (1) were eligible for this study. At surgery intestinal length was recorded in a standardized fashion by the operating surgeon. Postoperatively the patients' parents were approached for consent. Exclusion criteria were the presence of renal failure, or the presence of other major chromosomal or metabolic syndromes.
Study protocol.
This was a prospective open descriptive study. Patients were studied early in the adaptive process, as part of an assessment of nutrient absorptive capacity done soon after the initiation of feeds. Studies were typically initiated two to three weeks following recovery from the initial disease process (typically necrotizing enterocolitis), and subsequent surgery, although in some cases the surgery was a secondary procedure such as stoma revision or closure. After patients were stable and tolerating feeds of formula (at a rate > 2 mL/h > 48 h, as directed by their primary care physician or surgeon) they underwent assessment of baseline intestinal permeability, and nutrient absorptive study as previously described (23,24). In brief, patients were maintained on their enteral feeds, typically expressed breast milk or Pregestimil (Mead Johnson, Ottawa, ON). A 48-h stool collection was done, collecting all stoma output, or in patients with intestinal continuity nonabsorptive diapers were used, with a urinary catheter in place. Stool volume was measured, output frozen and subsequently analyzed for protein, fat and total energy. Carbohydrate derived energy was calculated from total energy less the protein and fat contribution using our previously described methods (18,23). Total energy content of feces was determined using freeze-dried material assayed for energy release with an oxygen bomb calorimeter (PARR 1261 Bomb Calorimeter, Moline, ILL).
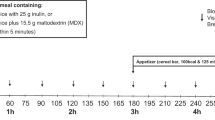
After the stool collection was complete, the patients were continued on their feeding regimen, and on the following day underwent assessment of the urinary recovery of orally administered 3–0 methylglucose (3–0 MG), lactulose and mannitol probes (Baxter Labs, Toronto, ON), quantifying active nutrient transport capacity and intestinal permeability characteristics as previously described (23,24). In brief, feeds were held for 30 min, and patients were gavaged with 1 mL/kg of a solution containing 30 mg/mL 3–0 MG, 20 mg/mL mannitol, and 30 mg/mL lactulose with an osmolality of 352 mosmol/L. Feed were then restarted immediately. Urine was collected for the subsequent eight hours, and the total volume recorded, and samples frozen. All patients had an indwelling urinary catheter placed. Urine specimens were batch analyzed for the content of 3–0 MG, mannitol and lactulose (23,24). Briefly, urine was filtered through a 0.4-μ filter, and diluted as necessary. Samples were deionized and injected on to a Dionnex MA-1 ion exchange column (Dionnex Corp, Sunnyvale, CA). Sugars were eluted with NaOH at a flow rate of 0.4 mL/min with concentrations ranging from 400–600 μm/L. The peaks were detected using pulse amperometric detection on a Dionex HPLC and quantitated as peak areas. Calibration was performed daily with authenticated samples. Data are reported as a percentage of the gavaged probe detected in the urine.
Subsequently, with feeds ongoing, blood samples were obtained via the patient's indwelling central venous line. Sample volumes were minimized because of the small size of the patients, and thus one sample per 8 wk period was deemed ethically appropriate After an appropriate volume discard 3 to 4 mL of blood was collected into iced, heparinized tubes. It was immediately transferred to an iced centrifuged tube containing the protease inhibitor PMSF (phenyl methyl sulfonyl fluoride, SIGMA St. Louis, Missouri), 4 μL/mL of 200-mmol solution. Samples were then centrifuged at 3000 g for 30 min at 4°C. Plasma was collected and stored at −80°C. Peptide was extracted using a Seppack C18 carrier (Waters Associate, Melford, MA, U.S.A.). GLP-2 activity was measured using a radioimmunoassay specific for the N-terminus of human GLP-2 (antibody code 92160) (25). Previously frozen samples were thawed, and extracted in a final concentration of 75% ethanol. Samples were then assayed with the N- terminus specific radio labeled antibody. Experimental detection limit was 1 pmol/L and the inter assay coefficient variation was 5% at a GLP-2 concentration of 40 pmol/L. Each sample was analyzed in duplicate.
Statistics.
Data are presented as mean ± SD of the mean. GLP-2 levels were correlated with nutrient absorption and bowel length using Pearson Correlation Coefficient (Instat Corporation, San Francisco, CA). GLP-2 levels of the patient group achieving TPN independence by one year of age was compared with the average GLP-2 levels of the non TPN independent patients using student's t test with Welch's correction (Instat). Two patients were sampled twice but each had undergone an intestinal reoperation (stricturoplasty and stoma revision with additional ileum placed in continuity with the enteric stream) and so their individual values were treated independently. Patients showing negative values for nutrient absorptive studies were treated as having zero absorption for statistical purposes.
Ethics.
The study protocol was reviewed and approved by the Regional Ethics Board. Informed written consent was obtained from the patients' parents before initiation of the study.
RESULTS
Patient characteristics.
The majority of these patients were small premature infants as outlined in Table 1. Average gestational age was 32.7 ± 3.4 wk, age at testing was 1.7 ± 1.4 mo, and average weight at testing was 3.5 ± 1.1 kg. The common causes of intestinal dysfunction were necrotizing enterocolitis (6), intestinal atresia (3), and volvulus with gastroschisis (2). GLP-2 levels were successfully measured in 12 patients, with 2 patients having repeated studies as described. (Table 2) Included in this table is bowel length in the enteric stream as measured at surgery for each patient. Table 3 shows feeding tolerance at the time of GLP-2 levels measurement, and the results of carbohydrate probe and nutrient absorption studies. In a number of patients without a stoma, stool collections were incomplete and therefore not valid.
Intestinal length and GLP-2.
GLP-2 levels were significantly correlated with residual small intestinal length (Table 2, Fig. 1), with r2 = 0.75, p < 0.005. Although still significant, the correlation with total intestinal length (small intestine + colon), was not as strong, r2 = 0.51; there was no correlation with ileal length, r2 = 0.31. Notably, in several patients with severe short small bowel but intact colon in the enteric stream, (patients 1 and 3), GLP-2 levels were very low (1 pmol/L). In three other measurements in patients with intact colon, but out of the enteric stream, (patients 2, 10a and 10b) GLP-2 levels were also very low (6 pmol/L or less in each, Table 1 and 2).

Small bowel length (cm) vs fed GLP-2 levels (pmol/L) (linear regression analysis).
Nutrient absorption and GLP-2.
To examine the relationship between GLP-2 release and nutrient absorption, we correlated GLP-2 levels with tolerance of enteral feeds (enteral calories as a % of total calories, Table 3, Fig. 2). GLP-2 levels were significantly correlated with enteral feeds, r2 = 0.64, p < 0.03. However, when we examined the relationship between nutrient absorption and GLP-2 levels, we found that rather than an inverse relationship, as initially hypothesized, there was a direct relationship between defined macronutrient (fat, protein, and carbohydrate) absorption and GLP-2 levels (Fig. 3). In each case GLP-2 levels were directly correlated with nutrient absorption, fat r2 = 0.72, protein r2 = 0.54, and carbohydrate r2 = 0.50, (p < 0.03 for all correlations). GLP-2 levels did not correlate with 3–0 MG absorption or permeability as assessed by lactulose/mannitol ratio (Table 3, correlations not shown).

Enteral feeds (%) total calories vs fed GLP-2 levels (pmol/L) (linear regression analysis).

Absorption dietary fat (%) vs GLP-2 levels (pmol/L) (linear regression analysis).
Gestational age and GLP-2.
To examine the effects of intestinal development on the potential for GLP-2 release, we attempted to correlate the gestational and corrected age of the infants against GLP-2 levels; there were no significant relationships detected (Table 1, correlations not shown). As a more simple measure of this we compared GLP-2 levels of patients studied at a corrected age of < 1 mo versus those studied at > 1 mo: (n 7 in each group) GLP-2 levels: 24.1 ± 29.1 studied at < 1 mo versus 41.9 ± 45.1 pmol/L studied at >1 mo, p = 0.20. Finally, two patients had GLP-2 levels drawn on 2 occasions (following intestinal reoperation) after 3 mo (patient 1, stricturoplasty at colonic anastomosis) and 2 mo (patient 10, addition of 30 cm of ileum into enteric stream): there were no apparent changes in the postprandial GLP-2 levels (Table 2).
During the study follow-up three of the patients died, all from complications of TPN related cirrhosis and liver disease. No patients remained on TPN at one year. The average GLP-2 level for the patients that were able to achieve TPN independence was 45.3 ± 38.1 pmol/L versus the patients who were not able to achieve TPN independence, GLP-2 levels 2.25 ± 2.5 (p < 0.006). A fed GLP-2 level of 15 pmol/L appeared to be discriminatory; no patient who had a level > 14 pmol/L died, while 3 of 4 patients who had levels below 14 died. The one patient who survived with levels below 15 pmol/L had an unusual motility disturbance as the cause of bowel dysfunction and in fact had a normal length bowel and colon, which could be subsequently reanastomosed.
DISCUSSION
This is the first study to examine GLP-2 levels in human infants. Although limited by the constraints of working with premature infants, the findings are consistent with postprandial GLP-2 production being important in the intestinal adaptive process in this patient population. The results of this study suggest that in human infants the small intestine is the most important site for the production of GLP-2. In those patients with very short small intestinal remnants, GLP-2 levels were consistently low (Table 2). Further, in these infants residual colon did not appear capable of producing significant amounts of GLP-2. In three of four cases, the patients with severe SBS had near normal lengths of residual colon in the enteric stream, but postprandial GLP-2 levels were very low (Table 2). In previous studies done by coworkers with our group it has been shown that in stable adult patients who are several years out from surgery the presence of residual colon is associated with increased levels of postprandial GLP-2 (17,18). The reasons for these differences are not clear. It is possible that they may relate to timing: in the present study infants were studied at most within a month of re-establishment of intestinal continuity with delivery of nutrients into the colon. The time course of the increased GLP-2 production noted in adult patients is not known, and may require an extended period, up to several years to occur; we know of no studies which have examined this point in humans. However, in animal studies we have shown elevated GLP-2 levels immediately after re-establishment of enteral feeds using a model in which very short segments of proximal jejunum were anastomosed to the ascending colon (10). In the present study we saw no changes in GLP-2 production in the two patients tested several months apart, one of whom had residual colon within the enteric stream (Table 2). These patients were clearly not absorbing enteral nutrients, and so any L-cells present in the distal small intestine and colon should have been stimulated directly (16). In the patients with colon or ileum out of the enteric stream there was no response to proximal feeding, suggesting that the L-cells must be in the enteric stream to be functional (Table 2, patients 2, 10a, 10b). Together these results are consistent with animal studies which suggest that under normal conditions GLP-2 is produced mainly by the enteroendocrine L-cells of the distal small bowel in response to proximal nutrients (9,26).
It has been assumed that the population of L-cells, which have been shown to exist in the distal colon and rectum in adult humans (11,12), produce GLP-2 in normal and pathophysiological states (17,18). However, this has not been specifically studied, nor has the localization or functionality of L-cells been examined in human infants. Finally, the primary cause of intestinal dysfunction in the majority of the infants in the present study (NEC, atresia, and volvulus) all have a significant ischemic component, which may alter the production or response to GLP-2 in the residual intestine. Accordingly, in the present study, the lack of production of GLP-2 in patients with severe SBS is probably caused by the resection of the L-cell bearing ileum, but it may be compounded by a disease induced or age-related inability to produce an appropriately responsive L-cell population in remnant small bowel and colon.
These findings suggest that the GLP-2 “axis” is functional in human infants, even those who were very premature. All patients with residual ileum produced elevated levels of GLP-2, even if they were premature, and when feeds were just introduced. In animal studies, the GLP-2 axis of L-cell production and GLP-2 receptor expression has been shown to be present in late neonatal development, with high levels of tissue and plasma GLP-2 during weaning, and a rapid decline to adult levels thereafter (20). These findings suggest that GLP-2 signaling may be involved in the normal maturation and growth of the intestine during early infancy. Further studies to examine both the ontogeny, and the effect of disease on the development of the GLP-2 axis in the human infant are required. These factors may be especially important in light of the well-described differences in the behavior of SBS between infants and adults (1,27–29).
We do not feel that the variations in GLP-2 levels observed were due to adaptation that had already occurred. In all patients in the present study GLP-2 levels were measured soon after the introduction of feeds, during times when nutrient malabsorption was clearly evident. Several patients had levels taken after several weeks of feeding, and their GLP-2 levels were maintained (patients 4–8, Tables 1 and 2), while as noted in other patients who had levels repeated some months apart the levels did not increase (patients 1 and 10). Thus, we do not feel that GLP-2 levels were significantly reduced because adaptation had already occurred. In support of this, the time course of the GLP-2 response in animals is instructive. Over time (7–28 d following massive resection), GLP-2 levels following meals remain elevated, despite a near normalization of nutrient absorption (9). This suggests that GLP-2 is not simply associated with the adaptive response, but is important in the maintenance phase. To more completely define the interrelationships between the underlying disease process and the ontogeny of this system, much larger patient numbers will be required so that more sophisticated multi-variant analysis can be done.
Overall, these findings show that in human infants with severe intestinal dysfunction and SBS, GLP-2 levels are markedly diminished, and do not increase following feeding. Although correlative, the findings do suggest that GLP-2 stimulation could be of potential therapeutic benefit in this patient population (20,27). Further studies are indicated both to examine this possibility, and to further explore the mechanisms underlying GLP-2 production and effects in this patient population.
Abbreviations
- TPN:
-
total parenteral nutrition
- GLP-2:
-
glucagon like peptide 2
- GLP-1:
-
glucagon like peptide 1
- SBS:
-
short bowel syndrome
- PMSF:
-
phenyl methyl sulfonyl fluoride
References
Sigalet DL 2001 Short bowel syndrome in infants and children: an overview. Semin Pediatr Surg 10: 49–55.
Vanderhoof JA 1996 Short bowel syndrome in children and small intestinal trans plantation. Pediatr Clin North Am 43: 533–550.
Meehan JJ, Georgeson KE 1997 Prevention of liver failure in parenteral nutrition dependent children with short bowel syndrome. J Pediatr Surg 32: 473–475.
Drucker DJ, Ehrlich P, Asai SL, Brubaker PL 1996 Induction of intestinal epithelial proliferation by glucagon-like peptide 2. Proc Natl Acad Sci U.S.A. 93: 7911–7916.
Sigalet DL 2001 ALX-0600 (NPS Allelix Corp) Curr Opin Investig Drugs. 2: 505–509.
Jeppesen PB, Hartmann B, Thulesen J, Graff J, Lohmann J, Hansen BS, Tofteng Poulsen SS, Madsen JL, Holst JJ, Mortensen PB 2001 Glucagon-like peptide improves nutrient absorption and nutritional status in short-bowel patients with no colon. J Gastroenterol 120: 1041–3043.
Drucker DJ 2002 Biological actions and therapeutic potential of the glucagon like peptides. J Gastroenterol 122: 531–544.
Xiao Q, Boushey RP, Drucker DJ, Brubaker PL 1999 Secretion of the intestinotrophic hormone glucagon-like peptide 2 is differentially regulated by nutrients in humans J G. astroenterol 117: 99–105.
Martin GR, Wallace LE, Sigalet DL 2003 Nutrient stimulated GLP-2 release and crypt cell production in experimental short bowel syndrome. Can J Gastroenterol 17: A74A
Topstad D, Martin G, Sigalet D 2001 Systemic GLP-2 levels do not limit adaptation after distal intestinal resection. J Pediatr Surg 36: 750–754.
Vandell IM, Bishop AE, Sikri KL, Uttenthal LO, Bloom SR, Polak JM 1985 Localization of glucagon-like peptide (GLP) immunoreactants in human gut and pancreas using light and electron microscopic immunocytochemistry. J Histochem Cytochem 33: 1080–1086.
Eissele R, Goke R, Willemer S, Harthus HP, Vermeer H, Arnold R, Goke B 1992 Glucagon-like peptide-1 cells in the gastrointestinal tract and pancreas in rat, pig and man. Eur J Clin Invest 22: 283–291.
Rocca AS, Brubaker PL 1999 Role of the vagus nerve in mediating proximal nutrient-induced glucagon-like peptide 1 secretion. J Endocrinol 140: 1687–1694.
Cheeseman CI 1997 Upregulation of SGLT-1 transport activity in rat jejunum induced by GLP-2 infusion in vivo. Am J Physiol 273:R1965–R1971.
Tang-Christensen M, Larsen PJ, Thulesen J, Romer J, Vrang N 2000 The proglucagon-derived peptide, glucagon-like peptide-2, is a neurotransmitter involved in the regulation of food intake. Nat Med 6: 802–807.
Brubaker PL, Schloos J, Drucker DJ 1998 Regulation of glucagon-like peptide-1 synthesis and secretion in the GLUTag enteroendocrine cell line. J Endocrinol 139: 4108–4114.
Jeppesen PB, Hartmann B, Hansen BS, Thulesen J, Holst JJ, Mortensen PB 1999 Impaired meal stimulated glucagon-like peptide 2 response in ileal resected short bowel patients with intestinal failure. Gut 5: 559–563.
Jeppesen PB, Hartmann B, Thulesen J, Hansen BS, Holst JJ, Poulsen SS, Mortensen PB 2000 Elevated plasma glucagon-like peptide 1 and 2 concentrations in ileum resected short bowel patients with a preserved colon. Gut 47: 370–376.
Petersen YM, Burrin DG, Sangild PT 2001 GLP-2 has differential effects on small intestine growth and function in fetal and neonatal pigs. Am J Physiol Regul Integr Comp Physiol 281:R1986–R1993.
Lovshin J, Yusta B, Iliopoulos I, Migirdicyan A, Dableh L, Brubaker PL, Drucker DJ 2000 Ontogeny of the glucagon-like peptide-2 receptor axis in the developing rat intestine. J Endocrinol 141: 4194–4201.
Kreymann B, Ghatei MA, Domin J, Kanse S, Bloom SR 1991 Developmental patterns of glucagon-like peptide 1 (7-36) amide and peptide-YY in rat pancreas and gut. J Endocrinol 129: 1001–1005.
Calvert SA, Soltesz G, Jenkins PA, Harris D, Newman C, Adrian TE, Bloom SR, Aynsley-Green A 1985 Feeding premature infants with human milk or preterm milk formula. Biol Neonate 47: 189–198.
Sigalet DL, Martin GR, Meddings J 2004 3-0 Methylglucose uptake as a marker of nutrient absorption and bowel length in pediatric patients. J Parenteral and Enteral Nutr 28: 158–162.
Meddings J, Gibbons I 1998 Discrimination of site-specific alterations in gastrointestinal permeability in the rat. J Gastroenterol 114: 83–92.
Hartmann B, Johnsen AH, Orskov C, Adelhorst K, Thim L, Holst JJ 2000 Structure, measurement, and secretion of human glucagon-like peptide-2. Peptides 21: 73–80.
Orskov C, Holst JJ, Knuhtsen S, Baldissera FG, Poulsen SS, Nielsen OV 1986 Glucagon-like peptides GLP-1 and GLP-2, predicted products of the glucagon gene, are secreted separately from pig small intestine but not pancreas. J Endocrinol 119: 1467–1475.
Buchman AL, Scolapio J, Fryer J 2003 AGA technical review on short bowel syndrome and intestinal transplantation. J Gastroenterol 124: 1111–1134.
Vanderhoof JA 1996 Short bowel syndrome in children and small intestinal transplantation. Pediatr Clin North Am 43: 533–550.
Thulesen J, Hartmann B, Kissow H, Jeppesen PB, Orskov C, Holst JJ, Poulsen SS 2001 Intestinal growth adaptation and glucagon-like peptide 2 in rats with ilealjejunal transposition or small bowel resection. Dig Dis Sci 46: 379–388.
Acknowledgements
The authors thank Kim Tran for performing the HPLC measurements. We thank Drs. Butzner, Eccles, and Wong for help in completing these studies in their patients, and for their ongoing support and discussion. The authors thank the organizational and financial support of Lidia Demchyshyn and NPS Corporation in developing this collab oration and transporting specimens. The secretarial support of Gail Wright-Wilson is sincerely appreciated. Financial support of the Alberta Children's Hospital Foundation, and the Danish Medical Council is gratefully acknowledged. Finally, the sup port of the families, patients and the nurses on N cluster and the Foothill's Neonatal ICU, both in caring for these infants, and their unfailing support in completing these studies is very much appreciated.
Author information
Authors and Affiliations
Corresponding author
Additional information
Supported by a grant from the Alberta Children's Hospital Research Foundation and the Danish Medical Council.
Rights and permissions
About this article
Cite this article
Sigalet, D., Martin, G., Meddings, J. et al. GLP-2 Levels in Infants With Intestinal Dysfunction. Pediatr Res 56, 371–376 (2004). https://doi.org/10.1203/01.PDR.0000134250.80492.EC
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1203/01.PDR.0000134250.80492.EC
This article is cited by
-
Management and Complications of Short Bowel Syndrome: an Updated Review
Current Gastroenterology Reports (2016)
-
Role of glucagon-like peptide–2 deficiency in neonatal short-bowel syndrome using neonatal piglets
Pediatric Research (2013)
-
Intestinal Permeability and Glucagon-like peptide-2 in Children with Autism: A Controlled Pilot Study
Journal of Autism and Developmental Disorders (2008)
-
Glucagon-like Peptide-2 Induces a Specific Pattern of Adaptation in Remnant Jejunum
Digestive Diseases and Sciences (2006)
-
Management of intestinal failure
The Indian Journal of Pediatrics (2006)
