
Abstract
Background
Acquired tracheoesophageal fistula (TEF) is a rare presentation in pediatric lymphoma patients. Most heal spontaneously following chemotherapy/radiotherapy without requiring surgery.
Case presentation
A 10-year-old child is presented with persistent tracheoesophageal fistula after completion of chemotherapy for Hodgkin’s lymphoma. The mid-tracheal location of the fistula had significant implications in terms of airway management. Securing the airway with a microcuff tube helped meet the goals of achieving adequate ventilation while preventing airway contamination and permitting the repair without any complication.
Conclusions
The index case posed surgical and anesthetic challenges due to the size and location of the fistula. However, timely surgical intervention improved the quality of life of the child as well as that of the parents.
Similar content being viewed by others


Background
Acquired tracheoesophageal fistula (TEF) is rare in children. In adults, it is usually secondary to bronchial or esophageal carcinoma, whereas in children, it may occur following foreign body ingestion or inhalation, prolonged intubation, and irradiation for solid malignancies and lymphoma (Birman and Beckenham 1998; Lal et al. 2006).
We present the surgical and anesthetic challenges in a child with Hodgkin’s lymphoma and persistent TEF after completion of chemotherapy course.
Case presentation
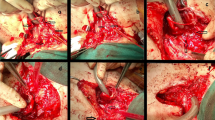
A 10-year-old female child, weighing 20 kg, was referred for closure of acquired tracheoesophageal fistula (TEF) at C7 (Figs. 1 and 2) and D2 level (Fig. 3), persistent even 4 months after completion of chemotherapy course (6 cycles, EURONET protocol) for nodular sclerosis type of Hodgkin’s lymphoma (stage 3 B + E). This case was previously reported, after 4 cycles of chemotherapy while being conservatively managed associated with improvement in systemic symptoms and subjective improvement in overall health with 2 kg weight gain (Munikoty et al. 2017). However, she continued spitting saliva with episodes of respiratory distress. There was poor right vocal cord movement. The child had been on nasogastric tube feed for 11 months as the family had refused a gastrostomy. There was constant fear of aspiration and poor quality of life.

Tracheoesophageal fistula after chemotherapy at C7 vertebra level with dimensions of 2.2 cm × 2.5 cm × 2.4 cm

Fistula at C7 vertebra level

Tracheoesophageal fistula at D2 vertebral level
The pre-anesthetic evaluation revealed no history suggestive of any systemic illness other than the lymphoma. The general physical, systemic, and airway examination revealed no abnormality. The baseline hemogram, serum electrolytes, renal function tests, and coagulogram were within normal limit. The child was fasted overnight and started on 60 ml/kg of Ringer lactate maintenance fluid during the fasting period. Aspiration prophylaxis in the form of injection pantoprazole 20 mg and injection metoclopramide 3 mg was administered on the morning of surgery. Before taking the child inside the operation theater, she was premedicated with 80 μg glycopyrrolate. No sedative premedication was administered.
Intraoperative monitoring consisted of ECG, NIBP, SpO2, end-tidal CO2, nasopharyngeal temperature, and urine output. Intravenous induction was carried out using 2 mg of morphine, 40 mg of propofol, and atracurium 20 mg followed by maintenance on propofol infusion. Under general anaesthesia, rigid bronchoscopy was performed initially and a Fogarty catheter passed across the fistula. Thereafter, trachea was intubated with a Kimberly Clark 5.5 mm microcuff pediatric endotracheal tube (ETT) (Fig. 4) which has a high-volume, low-pressure cuff which is less traumatic with better sealing of anesthetic gases, using CMAC® video laryngoscope. ETT position was also confirmed using fiber-optic bronchoscope besides bilateral chest auscultation and fixed at 18.5 cm. The child was ventilated with inspiratory pressure of 14 cmH2O and PEEP of 5 cmH2O, and respiratory rate was adjusted to maintain ETCO2 between 35 and 40 mmHg. An 18G intravenous cannula and a 22G left radial arterial cannula were secured. Anesthesia was maintained with isoflurane in a mixture of air and oxygen. Surgery was performed in left lateral position. In spite of extensive fibrosis, making separation of trachea from esophagus difficult, the two were adequately mobilized and closed, with a sternocleidomastoid muscle interposition graft. A gastrostomy, feeding jejunostomy, and tracheostomy were placed. Serial intraoperative ABGs were within normal limits. Perioperative analgesia consisted intravenous morphine (2 mg), fentanyl (40 mcg), paracetamol (300 mg), and intercostal nerve block with 0.1% ropivacaine before closure of wound. Ondansetron (2 mg) was also given for prevention of postoperative nausea and vomiting. Patient was shifted and intubated to surgical intensive care unit for elective mechanical ventilation for better graft healing and uptake.

5.5 mm microcuffed endotracheal tube
She was sedated and electively mechanically ventilated to allow for the graft to heal and allow its proper uptake, following which she was gradually weaned off the ventilator by the eleventh postoperative day. The postoperative period was uneventful. Oral feeds were gradually started following a contrast esophagogram on day 14. She was discharged home with tracheostomy in situ and decannulation done a month later. At more than 1-year follow-up, she is on solid diet with no dysphagia. She has mild stridor, the hoarseness of voice has improved, and she is now able to speak a few words and attends school.
Discussion
Acquired TEF is a life-threatening event. It is very rare as an initial manifestation of Hodgkin’s disease in children (Lal et al. 2006; Alba et al. 1994). In one study, over a 23-year study period, only 13 pediatric oncology patients developed esophageal complications in the form of strictures or fistula. These were noted at a mean 3.5 years (range 0.4–11.8 years) after cancer diagnosis with 14 patients (93%) having received mediastinal radiation. Fistulas were seen only in 4 patients aged 3–16 years in mid or distal esophagus, of whom only one had Hodgkin’s disease (Lal et al. 2006).
Compression by tumor mass, direct tumor invasion, and most commonly tumor necrosis following irradiation or chemotherapy are the likely causes of TEF (Lal et al. 2006; Alba et al. 1994). Our patient had initially manifested with a neck abscess, and bursting of necrotic tracheobronchial lymph nodes may have been causative.
The TEF in lymphoma is said to have a better prognosis than other malignancies (Westin et al. 2012). While many cases are expected to heal following chemotherapy and radiotherapy, the respiratory tract has to be protected in the interim. The recommended initial treatment is to place a stent in the trachea or esophagus. However, this was not considered feasible in our patient due to the fistula location and the cost involved. Surgical intervention was therefore considered as the fistula was persisting 5 months after completion of chemotherapy.
The main anesthetic challenges were that the ETT, especially its cuff, had to be placed accurately beyond the fistula; adequate care had to be taken to avoid tube dislodgement, and measures were taken to prevent leak of anesthetic gas and aspiration of fluid during the surgery. The surgical anastomosis was close to the ETT especially due to the large size of the fistula, and its sterility had to be maintained during insertion.
The index case posed surgical and anesthetic challenges due to the size and location of the fistula. However, results were gratifying and improved the quality of life of the parents as well as that of the child who is now able to attend school.
Conclusions
To conclude, in our case, securing the airway with an appropriate-sized microcuff ETT helped provide a clear surgical field while maintaining adequate ventilation and simultaneously protecting the soiling of airway. Use of interposition muscle graft, adequate mobilization before fistula closure, and early nutritional rehabilitation is important to prevent recurrence, lumen stenosis, and improvement in surgical results.
Availability of data and materials
Not applicable.
Abbreviations
- TEF:
-
Tracheoesophageal fistula
- ETT:
-
Endotracheal tube
References
Alba D, Lobato SD, Alvarez-Sala R, Villasante C, Echevarria C (1994) Tracheoesophageal fistula as the presenting manifestation of Hodgkin’s lymphoma. Postgrad Med J 70:49–50
Birman C, Beckenham E (1998) Acquired tracheo-esophageal fistula in the pediatric population. Int J Pediatr Otorhinolaryngol 44:109–113
Lal D, Foroutan H, Su W, Wolden S, Bouland F, La Quaglia M (2006) The management of treatment related esophageal complications in children and adolescents with cancer. J Pediatr Surg 41:495–499
Munikoty V, Bhatia A, Bansal D, Das A, Khandelwal N (2017) Acquired TEF in Hodgkin lymphoma in a child: a rare clinical association. J Pediatr Hematol Oncol 39:309–310
Westin JR, Gibbs A, Mills KR, Neelapu SS (2012, 2012) Hodgkin lymphoma untreated for six years presenting with tracheoesophageal fistula. Case Rep Med:457908. https://doi.org/10.1155/2012/457908
Acknowledgements
None.
Funding
None.
Author information
Authors and Affiliations
Contributions
IS was involved in anesthetic management and review of manuscript. PM was involved in surgical management and review of manuscript. SP was involved in drafting the manuscript. RK was involved in patient management and drafting the manuscript. DB was involved in patient management and review of manuscript. The authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Written informed consent was obtained from patient’s legal guardian.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Sen, I.M., Menon, P., Puri, S. et al. Perioperative management of acquired TEF repair in a child with Hodgkin’s lymphoma: a case report. Ain-Shams J Anesthesiol 14, 62 (2022). https://doi.org/10.1186/s42077-022-00261-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s42077-022-00261-y