Article Text

Statistics from Altmetric.com
One of the major research areas for tuberculosis (TB) focuses not only on diagnostics but also on biomarkers that can provide prognostic data about the disease course and response to treatment. Although progress has been made, improved tests for paediatric TB are especially needed. Young children are at increased risk of progressing to TB after exposure, and may suffer from disseminated forms of the disease. Due to the paucibacillary nature of paediatric disease, the current armamentarium and future pipeline of TB diagnostics that largely rely on microbial growth and/or molecular detection are unlikely to demonstrate performance equivalent to that in adults. Thus, an accurate surrogate marker of disease may be crucial to improving the diagnosis of paediatric TB. We have tested and evaluated a novel B-cell assay called the antibodies in lymphocyte supernatant, or ALS, which has performed very well in diagnosing TB disease both in Asia1 2 and Africa (manuscript in preparation). Here, we report the performance of ALS as a biomarker in children with culture-confirmed TB.
The ALS assay is based on a principle similar to that of the enzyme-linked immunosorbent spot assay, measuring antibody-secreting cells in cultures of peripheral blood mononuclear cells (PBMCs). The ALS assay detects antibody secretion from in vivo activated plasma B cells that migrate throughout the peripheral circulation in response to TB antigens that are present during active disease but not latent TB infection.3 The ALS methodology for children includes phlebotomy of 3.5 ml of blood in order to isolate 5 million PBMCs; these cells are incubated in tissue culture plates without stimulation for 48–72 h. The supernatant is collected, placed into BCG-coated microtitre plates and IgG responses to BCG are measured by ELISA.1 3 A positive titre is defined as ≥0.350 optical density units, calculated from data on healthy children.3 In its present format, the method requires skilled personnel and equipment for PBMC separation from blood samples, sterile cell cultures and ELISA.
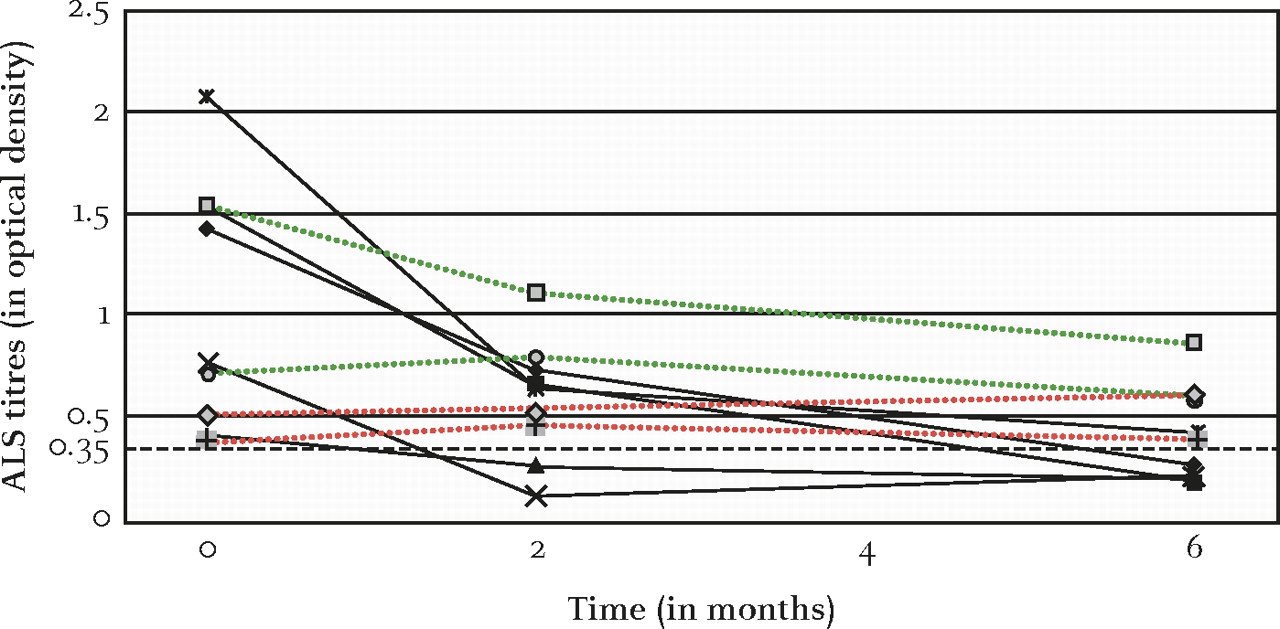
A prospective study of children from a low-HIV prevalence area of Bangladesh assessed ALS responses among 58 hospitalised children with clinically diagnosed TB (ages 1–14 years, 15% confirmed by culture), 16 hospitalised children ruled out for TB and 58 age-matched controls. The ALS assay was 91% sensitive and 87% specific when compared with the clinical diagnostic algorithm for diagnosing TB disease and performed equally well in TB cases <5 years old compared with those ≥5 years.3 Notably, the BCG-specific IgG titres declined after starting appropriate anti-TB treatment. Figure 1 illustrates the trends in ALS titres for nine paediatric patients with culture-confirmed TB. Five of these patients had drug-susceptible TB and four patients had drug-resistant TB, including one patient with TB resistant to isoniazid and streptomycin, another with TB resistant to rifampin, streptomycin and ethambutol, and two patients with TB resistant to isoniazid and rifampin (multidrug-resistant (MDR) TB). First-line anti-TB therapy (isoniazid, rifampin, pyrazinamide) in patients with drug-susceptible TB resulted in a significant reduction in ALS titres after 2 months (p=0.016), whereas the four patients with drug-resistant TB demonstrated only a marginal decline in ALS titres after 2 months of first-line anti-TB therapy (p=0.62), reflecting their clinical status (table 1). However, modification of the antibiotic regimen led to clinical improvement and gradual reduction of the ALS titres in three of these four patients. The fourth patient—with MDR TB—took longer time to recover clinically, despite appropriate second-line anti-TB therapy, which paralleled the delayed reduction in ALS titres. Previously, we have illustrated a similar profile of the ALS response in adults with MDR TB.2
{kind=link}
Antibodies in lymphocyte supernatant (ALS) titres during the course of anti-tuberculosis (TB) therapy. The black dashed line represents the threshold value for a positive test, 0.35 optical density. Solid data lines depict changes in ALS titres for children found to have culture-confirmed drug-susceptible TB. Dotted data lines depict changes in ALS titres for children found to have drug-resistant TB; red dotted lines represent children with multidrug-resistant TB (isoniazid and rifampin resistant) and green dotted lines represent children with drug-resistance to isoniazid or rifampin (but not both). ALS titres from the five children with drug-susceptible TB significantly declined after 2 months of first-line anti-TB treatment (p=0.016). However, ALS titres failed to decline significantly after 2 months of first-line anti-TB treatment among the four children who were later found to have drug-resistant TB (p=0.62). After these four children initiated second-line anti-TB treatment, the ALS titres gradually declined, mirroring their clinical improvement.
Demographic and clinical characteristics of patients (N=9)
The ALS assay is different from traditional serological tests that quantify TB-specific IgM, IgG or IgA levels in serum. Since the serum containing pre-existing antibodies in vivo is removed on isolation of PBMCs, the ALS assay focuses on assessing active antibody secretion from TB-specific plasma cells circulating during TB disease. Traditional serological tests have greatly varied sensitivity and poor specificity for TB disease, and the results cannot discriminate active or subclinical disease from latent TB infection.4 The sensitivity is greatly reduced in sputum-smear negative and/or HIV-infected individuals and may also be affected by prior BCG vaccination, or exposure to non-tuberculous mycobacteria.5 By contrast, the performance of the ALS assay is not adversely affected by these clinical conditions.
The ALS assay is a novel method that is feasible and has high accuracy in detecting TB disease in children3 and adults1 2; however, it warrants further assessment as a biomarker for response to therapy. Interestingly, evaluation of the ALS method for TB diagnosis in Ethiopian adults demonstrated significant positive results for both TB-infected and TB–HIV co-infected patients suggesting that this test, in contrast to presently available immunological assays, can perform well in HIV-infected populations (manuscript in preparation).
Footnotes
Funding The funders of the study—Swedish International Development Cooperation Agency and the International Centre for Diarrhoeal Disease Research, Bangladesh (ICDDR,B)—had no role in the study design, data interpretation or writing of this manuscript.
Competing interests RR and DS are the inventors of the antibodies in lymphocyte supernatant assay which is patented; however, the ICDDR,B is the patent holder. Any potential financial gain will be for the Centre if/when this assay is commercialised. There are no other potential conflicts of interest related to the work presented.
Ethics approval This study was conducted with the approval of the Ethics Review Committee of the ICDDR,B.
Provenance and peer review Not commissioned; externally peer reviewed.