Article Text

Abstract
Severity of hypoxaemia can be assessed using the partial pressure of arterial oxygen to fraction of inspired oxygen ratio (FiO2). However, in patients breathing through non-rebreather reservoir bag oxygen mask, accuracy of bedside FiO2 estimation methods remains to be tested. In a post-hoc analysis of a multicentre clinical trial, three FiO2 estimation methods were compared with FiO2 measured with a portable oxygen analyser introduced in the oxygen mask. Among 262 patients analysed, mean (SD) measured FiO2 was 65% (13). The 3%-formula (21% + oxygen flow rate in L/min × 3) was the most accurate method to estimate FiO2. Other methods overestimated FiO2 and hypoxaemia severity, so they should be avoided.
- critical care
Statistics from Altmetric.com
Introduction
Ratio of partial pressure of arterial oxygen to fraction of inspired oxygen (PaO2/FiO2) is a widely used index of oxygenation, easy-to-assess at bedside, enabling assessment of severity of hypoxaemia,1 considered in the calculation of prognosis scores2 and a common inclusion criterion in clinical trials on patients breathing spontaneously.3 Unlike during mechanically ventilation, FiO2 cannot be easily measured at the bedside in patients breathing spontaneously through non-rebreather reservoir bag oxygen mask. Therefore, various formulas or tables have been proposed to estimate FiO2 according to oxygen flow rate.4–6 However, the reliability of these estimation methods has yet to be investigated. The aim of our study was (1) to compare the reliability of three different methods in the estimation of FiO2 in patients with acute hypoxaemic respiratory failure breathing spontaneously under non-rebreather reservoir bag oxygen mask: the 3%-formula (21% + oxygen flow rate in L/min × 3),4 the 4%-formula (21% + oxygen flow rate in L/min × 4)5 and a commonly used conversion table (online supplementary table 1)6 and (2) to test the physiological variables influencing FiO2.
Supplemental material
Methods
Patients
This study is a post-hoc analysis of a randomised clinical trial including patients with acute hypoxaemic respiratory failure defined as a respiratory rate >25/min and a PaO2/FiO2 ratio ≤300 mm Hg with FiO2 measured in a non-rebreather reservoir bag oxygen mask with an oxygen analyser (MX300, Teledyne Analytical Instruments).4 For the purposes of this study, we excluded patients in whom FiO2 was not measured, those in whom oxygen flow was not reported and those not breathing through non-rebreather reservoir bag oxygen mask. Vital signs, oxygen flow and arterial blood gas analysis at the time of FiO2 measurement were analysed.
Statistical analysis
Mean differences (95% CI) in FiO2 and PaO2/FiO2 were compared using t-test. Agreement between the different FiO2 estimation methods and measured FiO2 was considered using an arbitrary limit of agreement of ±10% and was assessed using Bland-Altman plot. Correlations between physiological variables and measured FiO2 were computed using Pearson correlation coefficient. A backward stepwise logistic regression model was computed to identify physiological variables associated with low FiO2 defined according to the median measured FiO2. Two-tailed p<0.05 was considered significant. According to French law, informed consent was waived for the current analysis.
Results
Among the 310 patients included in the original study, 27 were excluded for missing data and 21 for not breathing through non-rebreather reservoir bag oxygen mask. Baseline characteristics of the 262 patients retained in the analysis are displayed in table 1. With a median oxygen flow rate of 15 L/min (IQR 12–15), the mean (SD) measured FiO2 and PaO2/FiO2 were 65% (13) and 140 mm Hg (63), respectively.
Baseline characteristics of the patients
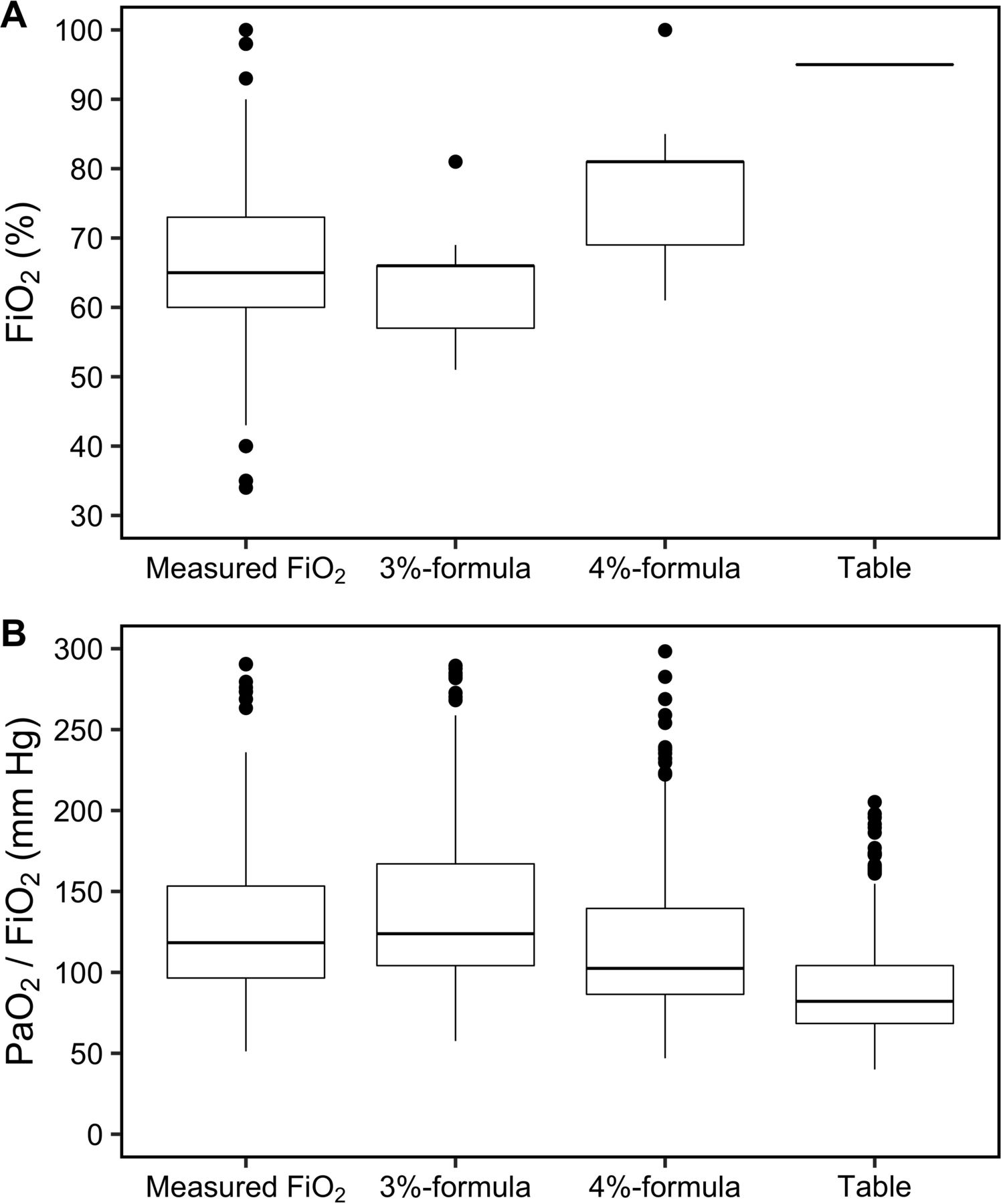
Mean (SD) estimated FiO2 and mean differences with measured FiO2 were 62% (6) with the 3%-formula (−3% (95% CI −5% to −2%), p<0.001), 75% (8) with the 4%-formula (+10% (95% CI 9% to 12%), p<0.001) and 95% (0) with the table (+30% (95% CI 28% to 31%), p<0.001; figure 1A). Mean (SD) estimated PaO2/FiO2 and mean differences with measured PaO2/FiO2 were 143 (56) with the 3%-formula (+3 mm Hg (95% CI −1 to +8), p=0.15), 118 (47) with the 4%-formula (−22 mm Hg (95% CI −27 to −18), p<0.001) and 92 (34) with the table (−48 mm Hg (95% CI −53 to −43), p<0.001; figure 1B).

(A) Comparison of fraction of inspired oxygen (FiO2) according to the different methods of FiO2 and the different methods used to estimate FiO2 (p<0.001 between each group). (B) Comparison of partial pressure of arterial oxygen (PaO2)/FiO2 according to the different methods of FiO2 and the different methods used to estimate FiO2 (p=0.15 between measured FiO2 and 3%-formula, p<0.001 otherwise).
Bland-Altman plot assessing agreement between measured FiO2 and the FiO2 estimation methods is displayed in figure 2. The proportion of patients within the ±10% arbitrary limit of agreement of measured FiO2 was 63% (n=164) with the 3%-formula, 44% (n=114) with the 4%-formula and 7% (n=19) with the table (p<0.001). Among patients in whom FiO2 was misestimated, the overestimation rate was 35% (34 out of 98 patients) with the 3%-formula, 89% with the 4%-formula (131 out of 148) and 100% of the 243 patients with the table.

{kind=link}
{kind=link}
Agreement between measured fraction of inspired oxygen (FiO2) and the different methods used to estimate FiO2 using the Bland and Altman method. The 3%-formula is represented with orange dots and lines, the 4%-formula with blue triangles and lines, and the conversion table with red lozenges and lines. Dashed lines represent mean of differences and continuous lines 1.96 SD. The grey box represents the predetermined arbitrary ±10% limit of agreement.
Measured FiO2 was positively correlated with oxygen flow rate (r=0.28), PaCO2 (r=0.20) and age (r=0.13), and negatively correlated with height (r=−0.22, online supplementary figure). Using multivariable analysis, tallness, increased respiratory rate and decreased PaCO2 were variables independently associated with low measured FiO2 (<65%) after adjustment on oxygen flow rate (online supplementary table 2).
Supplemental material
Supplemental material
Discussion
The 3%-formula had the best agreement and enabled accurate estimation of measured FiO2 in 63% of cases, with similar PaO2/FiO2 estimated with the 3%-formula and with measured FiO2. By contrast, the 4%-formula and the table were associated with almost consistent overestimation of measured FiO2, resulting in a dramatic underestimation of PaO2/FiO2, and therefore, a potentially marked overestimation of respiratory disease severity. Furthermore, measured FiO2 at a given oxygen flow rate varied according to patients’ physiological characteristics.
Interindividual variability of FiO2 in healthy volunteers breathing oxygen through a mask was reported more than 50 years ago.7 The respective influence of tidal volume and respiratory rate on measured FiO2 was described in a bench model.8 Here, we confirm that oxygen delivery by non-rebreather reservoir bag mask is altered by breathing pattern in patients with acute hypoxaemic respiratory failure. During oxygen therapy through a mask, oxygen accumulates in the mask, leading to increased oxygen concentration and FiO2. Hence, determinants of minute ventilation, tidal volume and respiratory rate, and its consequence, PaCO2, influence oxygen accumulation in the mask and FiO2. Although tidal volumes were not measured, height could influence minute ventilation and resultantly FiO2 through its major impact on lung volumes.9
Some limitations have to be acknowledged. First, measured FiO2 could not be an accurate surrogate of actual FiO2 as reported in healthy volunteers.10 However, measurement of FiO2 in the oropharynx or the trachea of acutely ill patients is nearly impossible. Second, the ±10% limit of agreement seems reasonable but is debatable. Although a narrower limit of agreement would have decreased accuracy of the 3%-formula, it would also have increased the proportion of FiO2 overestimation with the 4%-formula and the table. Third, our patients were treated with high oxygen flow rates under non-rebreather reservoir bag masks. Whether the accuracy of FiO2 estimation methods would be similar with lower oxygen flow rates and other oxygen masks remains to be tested.
These results call into question the actual respiratory severity of the patients breathing spontaneously through a non-rebreather reservoir bag oxygen mask included in most studies. Our results suggest that the 3%-formula should be used to compute PaO2/FiO2 in patients breathing spontaneously under non-rebreather reservoir bag oxygen mask to more accurately compare treatment effects according to depth of hypoxaemia. All in all, the 3%-formula may be useful as a means of assessing respiratory severity of patients with acute hypoxaemic respiratory failure in clinical studies, as well as in real life. Whether the choice of the FiO2 estimation method used to calculate PaO2/FiO2 would modify clinical decisions remains unknown.
Conclusion
Despite limited accuracy, in patients with acute hypoxaemic respiratory failure breathing spontaneously high oxygen flow rates under non-rebreather reservoir bag masks, the 3%-formula better estimated measured FiO2 compared with the 4%-formula and the conversion table. The latter two methods markedly underestimated PaO2/FiO2 ratio compared with the 3%-formula. Measured FiO2 varied according to height, respiratory rate and PaCO2.
Acknowledgments
The authors gratefully thank Jeffrey Arsham for editing the original manuscript.
Footnotes
Contributors All authors designed the study, wrote the manuscript together and approved the final version of the manuscript. All authors give their agreement to be accountable for all aspects of the work, and ensure the accuracy and integrity of any part of the work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests RC reported receiving grants from the French Ministry of Health, Le Nouveau Souffle, AADAIRC, French Intensive Care Society and European Respiratory Society, and non-financial support from Fisher & Paykel Healthcare and MSD outside the submitted work. J-PF reported receiving grants from the French Ministry of Health and personal fees and non-financial support from Fisher & Paykel Healthcare outside the submitted work. CG reported non-financial support, personal fees and logistic support from Fisher & Paykel, Resmed and Lowenstein Medical. AWT reported receiving grants from the French Ministry of Health, personal fees and non-financial support from Fisher & Paykel Healthcare, and personal fees from Maquet-Getinge, GE Healthcare and Covidien outside the submitted work.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.