Article Text

Abstract
Background The European Alliance of Associations for Rheumatology recommended that lipid-lowering therapy (LLT) in systemic lupus erythematosus (SLE) should follow general population guidelines. We examined the eligibility for LLT in SLE according to Systematic Coronary Risk Evaluation (SCORE), with and without the addition of vascular ultrasound (VUS) and disease-related features.
Methods 210 patients with SLE without prior cardiovascular events, diabetes or antiphospholipid syndrome underwent cardiovascular risk assessment with SCORE. LLT eligibility was evaluated in low-risk and moderate-risk patients following European Society of Cardiology (ESC) guidelines. Atherosclerotic plaques on carotid ultrasound (cUS)) and carotid and femoral ultrasound (cfUS), prolonged disease duration (PDD, ≥10 years), failure to achieve lupus low disease activity state (LLDASno), cumulative glucocorticoid ‘cardiovascular harm’ dose (GCCVH, optimal cut-off to predict ultrasound-detected plaques) and antiphospholipid antibody positivity (aPLpos) were tested as SCORE risk enhancers for classification ability (phi coefficient) and agreement (Cohen’s kappa) using SCORE plus cfUS as a reference modality for LLT eligibility.
Results Plaques were detected in 9.9% of low-risk cases and 54.6% of moderate-risk cases. SCORE alone would indicate 0% of low-risk patients and 3% of moderate-risk patients for LLT eligibility. According to SCORE+cfUS, 9.9% of low-risk patients and 57.6% of moderate-risk patients, respectively, would be eligible for LLT based on ESC guidelines. Ιn low-risk/moderate-risk patients, phi values for SCORE+PDD, GCCVH (cut-off ≥11 g), LLDASno and aPLpos in antiplatelet-naïve antiphospholipid antibody-positive (aPLpos/APT−) cases were 0.06/0.13, 0.23/0.20, 0.07/0.16 and 0.06/0.33, respectively. Agreement for LLT eligibility to SCORE+cfUS was better for SCORE+PDD in moderate-risk patients and for SCORE+cUS in both groups of patients. SCORE+GCCVH and SCORE+aPLpos showed at least fair agreement (kappa ≥0.20) to SCORE+cfUS in low-risk or moderate-risk and in aPLpos/APT− moderate-risk patients, respectively.
Conclusion Disease-related and VUS features, in addition to SCORE, may help to improve LLT decision making in SLE. GCCVH and aPLpos improve LLT eligibility similarly and to a greater degree than PDD or LLDASno.
- Systemic Lupus Erythematosus
- Cardiovascular Disease
- Ultrasonography
- Atherosclerosis
- Lipids
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Current European Alliance of Associations for Rheumatology recommendations state that, following risk assessment that considers both traditional and disease-related cardiovascular risk factors, lipid management in systemic lupus erythematosus (SLE) should follow guidelines for the general population.
The European Society of Cardiology recommends the use of the Systematic Coronary Risk Evaluation (SCORE) risk prediction model to guide lipid-lowering therapy (LLT) eligibility, with additional use of risk modifiers such as vascular ultrasound (VUS) for low-risk or moderate-risk patients.
WHAT THIS STUDY ADDS
Use of VUS enhances risk classification for lipid management in patients with SLE at low risk or moderate risk according to SCORE.
Disease features such as glucocorticoid use and antiphospholipid antibody positivity showed at least fair agreement to SCORE plus VUS for for LLT eligibility mainly in moderate-risk patients with SLE according to SCORE alone.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Use of VUS and disease-related variables can inform SCORE-guided lipid management in SLE.
Introduction
Cardiovascular disease is a leading cause of morbidity and mortality in systemic lupus erythematosus (SLE).1–3 The European Alliance of Associations for Rheumatology (EULAR) issued recommendations4 5 emphasising the need for strict control of modifiable traditional and disease-related cardiovascular risk factors (CVRFs) in SLE, including blood pressure (BP), hyperlipidaemia, disease activity and chronic glucocorticoid exposure.
Hyperlipidaemia is associated with adverse cardiovascular outcomes in SLE4 6 7; however, it is often unrecognised and undermanaged.8–11 The recent EULAR recommendations for cardiovascular risk management in rheumatic and musculoskeletal diseases (RMDs)4 state that lipid management in SLE should follow general population guidelines. The European Society of Cardiology (ESC) guidelines recommend identifying patients eligible for lipid-lowering treatment (LLT) according to low-density lipoprotein (LDL) cholesterol targets tailored to Systematic Coronary Risk Evaluation (SCORE) classification.12–14 However, SCORE has been considered to potentially underestimate actual risk in SLE.4 5
Evidence in SLE suggests a discordance between risk predicted by SCORE and actual risk identified by the presence of asymptomatic atherosclerotic plaques on carotid and/or femoral vascular ultrasound (VUS),15 16 a non-invasive imaging tool recommended by ESC to improve risk classification to guide LLT in the general population.12 14 In SLE, a higher prevalence of carotid and femoral plaques compared with controls17 argues for the use of multivessel VUS for cardiovascular risk stratification in these patients.15 18 Interestingly, ESC guidelines state that chronic immune-inflammatory disorders, including RMDs, are risk modifiers for lipid management,12 but the magnitude of this risk modification was not clarified for SLE. Additional risk assessment by considering disease-specific variables, as discussed in EULAR recommendations,4 5 not traditionally included in SCORE may help to improve CVRF management.
Herein, following EULAR recommendations to consider both traditional and disease-specific SLE features for cardiovascular risk (CVR) assessment to guide risk factor modification, as well as to manage lipid levels according to guidelines issued for the general population, we aimed to investigate the impact of VUS and disease-related variables such as disease duration, cumulative glucocorticoid dose, disease activity and antiphospholipid antibody positivity (aPLpos) on LLT eligibility in SLE.
Methods
Study population
We examined 210 consecutive adult patients (all Caucasian) fulfilling the 2012 classification criteria for SLE,19 without prior atherosclerotic cardiovascular events, or cardiovascular comorbidities including antiphospholipid syndrome (APS) according to the updated Sapporo criteria,20 diabetes mellitus (DM) or advanced chronic kidney disease. The patient selection process is reported in online supplemental figure S1.
Supplemental material

Flowchart of risk classification process to examine eligibility for LLT in patients with SLE. aPL, antiphospholipid antibodies; LDL, low-density lipoprotein; LLT, lipid-lowering therapy; SCORE, Systematic Coronary Risk Evaluation; SLE, systemic lupus erythematosus.
Clinical, biochemical and imaging data
Investigators, blinded to each other, independently assessed patients’ rheumatological status (PPS and MGT), carotid and femoral arteries by VUS (GK) and cardiovascular health (GCD), including SCORE classification and attainment of LDL cholesterol targets according to ESC recommendations.12 14
The following data were collected during participants’ first visit at our department: age, gender, weight, height, total cholesterol (TC), LDL cholesterol, high-density lipoprotein cholesterol, triglycerides and disease features including disease duration, use of medications (statins, antihypertensives, antiplatelets, hydroxychloroquine, immunosuppressants and glucocorticoids) and antiphospholipid antibodies (aPL) [lupus anticoagulant (LA); IgG and IgM anticardiolipin antibodies (aCL); and IgG and IgM antibeta 2 glycoprotein I antibodies (β2GPI)] measured according to the Sydney classification criteria for APS.21 Calculated measures included body mass index, cumulative glucocorticoid dose, Systemic Lupus Erythematosus Disease Activity Index 2000 (SLEDAI-2K) score and lupus low disease activity state (LLDAS). LLDAS was defined as SLEDAI-2K score of ≤4 with no activity in major organ systems and no haemolytic anaemia or gastrointestinal activity, no new lupus disease activity compared with the previous assessment, a Safety of Estrogens in Lupus Erythematosus National Assessment physician global assessment (scale 0–3) score of ≤1, a current prednisolone (or equivalent) dose of ≤7.5 mg.day, and a standard maintenance dose of immunosuppressive drugs and approved biological agents.22 BP was measured according to the ESC guidelines.23
VUS examination was performed by the same experienced operator at eight different anatomical sites of the walls of the carotid and common femoral arteries according to a well-established imaging protocol followed by our Cardiovascular Risk Research Laboratory15 17 based on the Mannheim consensus.24 Ultrasonography was performed with a high-resolution B-mode ultrasound device (Vivid 7 Pro; GE Healthcare, California, USA).
Baseline CVR classification according to SCORE
Risk estimates were calculated with the SCORE equation,13 14 which considers age, gender, systolic BP and TC levels to calculate numerical estimates for 10-year risk of cardiovascular events, to guide LLT according to LDL levels.14 Following ESC guidelines,12 14 risk classes were applied as follows: low risk, <1%; moderate risk, 1.0%–4.9%; high risk, 5.0%–9.9% or extreme BP and/or TC levels; and very high risk, ≥10%.
Composite CVR classification according to SCORE plus disease-related or VUS features
Composite CVR classification was applied following current EULAR recommendations for CVRF management emphasising the need to consider both traditional and disease-related CVRFs for risk assessment in SLE.4 To refine patients’ CVR profile, VUS and disease-related CVRFs were used as risk enhancers (‘positive’ reclassifiers) in addition to baseline classification provided by SCORE. According to ESC recommendations,12 14 the presence of atherosclerotic plaques on carotid and/or femoral VUS is considered as a risk modifier which classifies patients as very-high risk (ie, equivalent to symptomatic atherosclerotic cardiovascular disease) independently of the risk classes assigned by SCORE. VUS-documented plaques were defined as a focal intraluminal thickening at the near and far arterial wall with intima–media thickness (IMT) of ≥1.5 mm or increased by at least 0.5 mm or 50% compared with the IMT value of the adjacent vascular wall.24
The SLE-specific CVRFs under examination as potential risk enhancers included the following variables reported by EULAR: disease duration,5 disease activity,4 5 glucocorticoid use4 5 and aPLpos4 5 (box 1). To maintain consistency between the application of VUS and disease-related CVRFs, binary risk categorisation was also applied for the latter, as follows:
Prolonged disease duration (PDD) was defined as disease duration of ≥10 years based on corresponding evidence from other high-CVR disorders such as rheumatoid arthritis25 and DM,12 14 and meta-analyses in SLE,26 which were included in the systematic literature review for the development of the EULAR recommendations for CVR management in RMDs including SLE and APS.4
Active disease was defined as failure to achieve lupus low disease activity state (LLDASno), a measure of disease activity currently endorsed by the EULAR recommendations for SLE management.5
Cumulative glucocorticoid ‘cardiovascular harm’ dose (GCCVH) was defined by calculation of a cut-off cumulative glucocorticoid dose predictive of VUS-detected atherosclerotic plaques as a very-high risk classifier (as discussed in the Statistical analysis section).
aPLpos. According to laboratory criteria for classification of APS21 and the EULAR recommendations,4 5 20 aPLpos was defined as the presence of LA and/or medium-titre–high-titre aCL and/or medium-titre–high-titre anti-β2GPI on two or more occasions, at least 12 weeks apart.
Potential disease-related and vascular imaging risk enhancers
Disease-related features:
Disease duration of ≥10 years
Cumulative glucocorticoid dose
Failure to achieve low lupus disease activity state
Antiphospholipid antibody positivity
Vascular imaging features:
Presence of asymptomatic atherosclerotic plaques on carotid and/or femoral artery ultrasound
Hyperlipidaemia management
At the time of VUS examination, patients not undergoing LLT were classified as in ‘no need for intervention’ or ‘need for intervention’ for LDL cholesterol levels, respectively, with ‘intervention’ referring to lifestyle measures and/or indication for LLT according to ESC guidelines.12 Patients on treatment with lipid-lowering agents were further examined for ‘adequate treatment’ or ‘inadequate treatment’ following lipid targets established for the general population.
Assessment of eligibility for LLT
According to ESC guidelines,12 14 CVR refinement by use of risk enhancers applied to SCORE classification may prove clinically useful in low-risk and moderate-risk patients. Thus, LLT eligibility according to LDL cholesterol levels was evaluated by a stepwise approach including SCORE alone and subsequently by using SCORE plus carotid ultrasound (cUS),12 PDD,5 26 LLDASno,4 5 27 aPLpos4 5 20 26 and GCCVH (a surrogate measure of chronic glucocorticoid exposure4 5) for risk classification compared with SCORE plus carotid and femoral ultrasound (cfUS)12 as a reference risk enhancer. Risk classification and assessment of LLT eligibility are summarised in figure 1.
Statistical analysis
Data distribution was assessed with the Kolmogorov-Smirnov goodness-of-fit test. Comparison of continuous variables was assessed with Student t-test and Mann-Whitney U test in normally distributed and non-normally distributed data, respectively. Quantitative data are presented as mean±SD if normally distributed and as median (IQR) when non-normally distributed. Pearson χ2 and Fisher exact tests were used to compare categorical variables. Qualitative data are presented as relative frequencies.
Because of the inconclusive evidence on glucocorticoid use measures to predict cardiovascular events in SLE,4 28 in low-risk and moderate-risk patients not undergoing LLT, Youden’s J statistic was used to calculate (1) optimal thresholds for GCCVH reflecting points of maximum accuracy to predict very high CVR (ie, presence of atherosclerotic plaques)12 14 and (2) performance measures (area under the curve, sensitivity, specificity, positive predictive value and negative predictive value) corresponding to the identified GCCVH cut-off. Logistic regression analysis was applied to explore disease-related predictors of plaque presence, after adjusting for traditional CVRFs included in the SCORE equation.
To test the classification ability of the different ‘SCORE plus risk enhancer’ assessment strategies, phi coefficient was used as an established measure of binary risk categorisation for imbalanced data,29 using SCORE plus cfUS as a reference classifier, given the higher CVR associated with the presence of both carotid and femoral plaques.15 18 Agreement between LLT eligibility according to SCORE plus PDD, GCCVH, LLDASno or aPLpos, and eligibility guided by SCORE plus cfUS (as a reference rater) was assessed with Cohen’s kappa.
Given that antiplatelet use is associated with a lower CVR even in patients without symptomatic cardiovascular disease,14 30 a sensitivity analysis that examined aPLpos as a potential risk enhancer excluding aPL-positive cases on antiplatelet treatment (ie, ‘aPLpos/APT−’ subgroup) was incorporated in the analyses for risk classification and eligibility for LLT.
Results
Baseline characteristics
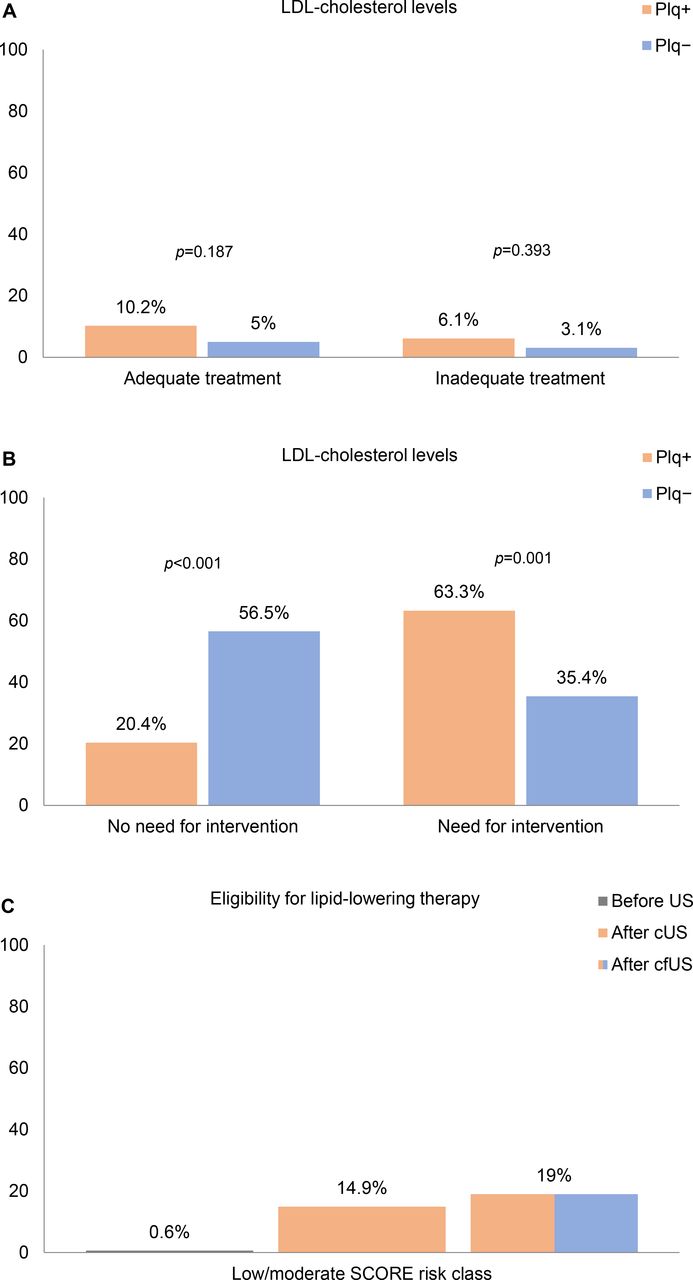
Patients with atherosclerotic plaques [49 cases; carotid (isolated): 38.8%; femoral (isolated): 16.3%; carotid and femoral: 44.9%] had longer disease duration and higher total and LDL cholesterol levels than those without (online supplemental table S1). Patients with plaques not undergoing LLT were more likely to be in need of intervention for LDL cholesterol levels compared with patients without plaques (63.3% vs 35.4%, p=0.001; figure 2B).

Hyperlipidaemia management in patients with SLE. (A) Treatment adequacy according to LDL cholesterol levels in patients undergoing LLT. (B) Proportions of patients requiring intervention (lifestyle measures and/or pharmacological therapy) for LDL cholesterol levels. (C) Proportions of patients at low/moderate score risk in need of LLT according to LDL cholesterol levels before and after the use of VUS. cUS, carotid ultrasound; cfUS, carotid and femoral ultrasound; LDL, low-density lipoprotein; LLT, lipid-lowering treatment; Plq, presence (+) or absence (−) of atherosclerotic plaques on vascular ultrasound; SCORE, Systematic Coronary Risk Evaluation; SLE, systemic lupus erythematosus; VUS, US, ultrasound; VUS, vascular ultrasound.
In the LLT-naïve low-risk or moderate-risk group, all modifiable SCORE variables, disease duration, and cumulative glucocorticoid dose were significantly higher in patients with plaques compared with patients without plaques (table 1). A higher prevalence of plaques at all anatomical sites was observed within the moderate-risk group compared with the low-risk group (figure 3B).

{kind=link}
{kind=link}
{kind=link}
Distribution of VUS-detected plaques among the examined anatomical sites and risk classes in patients with SLE at low or moderate SCORE risk class not undergoing lipid-lowering treatment. (A) Prevalence of risk classes within each anatomical site group; percentages refer to frequency of plaques per risk class per total number of patients with plaques. (B) Prevalence of anatomical sites within each risk group; percentages refer to frequency of plaques per anatomical site per number of patients at low or moderate risk. SLE, systemic lupus erythematosus; SCORE, Systematic Coronary Risk Evaluation; VUS, vascular ultrasound.
Traditional and disease-related CVRFs of patients with SLE at low or moderate score risk not undergoing lipid-lowering therapy (N=174)
Predictors of plaques in patients at low or moderate SCORE risk class not undergoing LLT
In LLT-naïve patients at low or moderate risk according to SCORE, carotid plaques were detected in 37.5% of cases, and plaques at both carotid and femoral arteries in 40.6% of cases (table 1). J statistic defined the GCCVH optimal high-risk cut-off at ≥11 g with a positive predictive value of 73.9% (online supplemental table S2). Multivariate analysis for disease-related CVRFs showed that, after adjustment for SCORE variables, GCCVH was an independent determinant of plaque presence (online supplemental table S3).
CVR classification
Baseline classification by SCORE alone is shown in online supplemental table S1. As displayed, SCORE misidentified 33% and 47% of patients with plaques as low risk and moderate risk, respectively.
Risk classification and eligibility for LLT according to SCORE alone and SLE-related CVRFs and VUS in addition to SCORE in low-risk or moderate-risk patients are presented in table 2. In low-risk patients, high-risk classification based on SCORE plus PDD, GCCVH and LLDASno was 34.0%, 27.0% and 35.9%, respectively, while SCORE plus aPLpos would classify at high risk 17.7% and 9.4% of all and aPLpos/APT− patients, respectively. SCORE plus cUS or cfUS upgraded the risk to a lesser degree compared with SCORE plus disease-related CVRFs, except in aPLpos/APT− patients. Phi coefficient showed that classification ability among SLE-specific risk enhancers was higher for SCORE plus GCCVH.
Risk classification and eligibility for lipid-lowering therapy according to disease-related and vascular imaging risk enhancers in treatment-naïve patients with SLE at low or moderate score class (N=174)
In the moderate-risk group, 66.7%, 57.6% and 33.3% of patients were classified at high risk using SCORE plus PDD, GCCVH and LLDASno, respectively, with comparable rates for SCORE plus cUS or cfUS. Within this group, SCORE plus aPLpos assigned 21.2% of patients vs 11.5% of aPLpos/APT− patients at high risk. Among disease-related risk enhancers, phi coefficient was higher for SCORE plus GCCVH, while SCORE plus aPLpos demonstrated the highest classification ability in aPLpos/APT− patients. SCORE plus cUS had the highest phi coefficient among all risk classification strategies in both low-risk and moderate-risk groups.
Eligibility for LLT in patients at low or moderate SCORE risk class not undergoing LLT
LLT eligibility according to LDL cholesterol targets corresponding to SCORE classification would be indicated in 0.6% of cases using SCORE alone compared with 14.9% and 19% of cases after assessment with cUS and cfUS, respectively (figure 2C). LLT eligibility in low-risk and moderate-risk groups is displayed in table 2. In both groups, a greater proportion of low-risk patients would be eligible with SCORE plus cUS or cfUS versus SCORE alone, while SCORE plus PDD, GCCVH or LLDASno would consider as eligible 31.2%, 25.5% and 32% of low-risk cases and 66.7%, 57.6% and 33% of moderate-risk cases, respectively. LLT eligibility based on SCORE plus aPLpos would be lower for both groups, with rates comparable to those indicated by SCORE plus cUS or cfUS in low-risk aPLpos/APT− patients.
Eligibility agreement between SCORE alone, SCORE plus disease features and cUS, and SCORE plus cfUS as the reference rater is shown in table 2. In the low-risk group, kappa values were low for all risk assessment strategies except for SCORE plus cUS and SCORE plus GCCVH. Results were similar in moderate-risk patients, although agreement was better for SCORE plus PDD and, mainly in aPLpos/APT− patients, SCORE plus aPLpos; in the same subgroup of aPL-positive patients, SCORE plus aPLpos also showed agreement to SCORE plus cfUS at a comparable degree to SCORE plus GCCVH.
Discussion
Our study showed for the first time that both VUS and disease-related CVRFs may improve CVR assessment for LLT eligibility in patients with SLE classified as non-high-risk by SCORE.
Recent EULAR recommendations4 5 proposed that CVR assessment in SLE should consider both traditional and disease-related risk factors to guide CVRF management, as well as to follow general population guidelines for LLT. LLT eligibility in the general population12 is based on CVR assessment according to prediction models such as the SCORE, which incorporates only traditional CVRFs, and risk enhancers such as VUS.12 14 Several disease-related CVRFs such as disease duration and disease activity, aPL and glucocorticoids are involved in cardiovascular disease pathophysiology in SLE.4 5 26 Therefore, we aimed to evaluate the agreement between SCORE plus disease-related traits tested as risk enhancers and SCORE plus cfUS used as a reference modality since risk assessment by VUS has been endorsed by the ESC guidelines for hyperlipidaemia management.12
Indeed, as stated by EULAR and also demonstrated by our results on the impact of using SCORE alone on LLT eligibility, risk assessment by SCORE may hinder CVRF management in SLE. In our study, VUS screening improved SCORE risk classification for LLT eligibility by 18.4% in patients at low risk or moderate risk. Previous SLE studies15 17 18 suggested that patients with both carotid and femoral plaques may be at a higher cumulative CVR,18 advocating for more aggressive CVRF management.
Despite mounting evidence about the role of disease-specific CVRFs,4 6 26 27 their inclusion into generic risk assessment models, as has been recommended for rheumatoid arthritis14 25 and systemic vasculitis,4 has yet to be endorsed for SLE. Difficulties to incorporate SLE-related variables into clinical practice may arise out of inconclusive evidence owing to differences in their definitions.4 6 26–28 This may be also reflected in the difference observed between the glucocorticoid dose predictive of atherosclerotic plaques identified in our study and doses reported to be associated with cardiovascular events in SLE,4 28 as well as in the impact of disease duration, disease activity and aPLpos on LLT eligibility. The 2022 EULAR recommendations for CVR management in RMDs highlighted that better identification of measures of exposure and outcomes may help to optimise patient management.4 Further research on how to effectively differentiate the role of disease-related features as subclinical risk markers, risk factors for clinical events or risk classifiers to guide CVRF management is warranted.
Among the examined disease-related classifiers, SCORE plus GCCVH had the highest agreement to SCORE plus cfUS-guided eligibility in both low-risk and moderate-risk groups. Additionally, GCCVH was found to be the only disease-related CVRF strongly associated with the presence of plaques on VUS, indicating that chronic glucocorticoid use may contribute to tailoring risk classification in SLE to CVRF management on par with traditional modifiable CVRFs. Nevertheless, the best measure of glucocorticoid use for CVR assessment in SLE has yet to be established.4 28 In a recent meta-regression analysis,28 average daily glucocorticoid dose was found to be more strongly associated with cardiovascular damage compared with cumulative dose, though cut-offs to discriminate non-high-risk from high-risk cases were not reported. Better identification of both average daily and cumulative GCCVH doses, as have been examined in RA,31 could help to optimise CVRF management in SLE.
A meta-analysis in SLE found that disease duration is an independent predictor of adverse cardiovascular outcomes in this RMD.26 In our study, compared with SCORE plus cfUS, SCORE plus PDD would include an additional 9.1%, while SCORE plus cUS would miss 15.2% of moderate-risk cases requiring LLT, respectively. Given the absolute difference between the latter two classification modalities, as well as the feasibility to assess clinical CVRFs prior to ordering an imaging test, it would be reasonable to consider the use of SCORE plus PDD for LLT eligibility in moderate-risk patients. However, in the same group of patients, agreement between eligibility based on SCORE plus PDD and eligibility according to SCORE plus cfUS was the lowest among all SLE-related classifiers. This finding suggests that further studies are needed to better elucidate its role in CVRF management in SLE.
aPLpos, in addition to SCORE, did not prove a useful risk modifier to guide LLT compared with the use of other disease-related features such as GCCVH. Nevertheless, given the role of antiplatelets in CVR prevention in the general population14 30 and the fact that low-dose aspirin is used for primary thrombosis prevention in aPL-positive patients with SLE,4 20 we decided to include in the analysis aPL-positive patients not receiving antiplatelets. Interestingly, SCORE plus aPLpos in aPLpos/APT− moderate-risk patients was found to significantly impact LLT eligibility, at a comparable degree to SCORE plus GCCVH. Current evidence20 26 32 supports the role of aPL to predict cardiovascular events in SLE; however, specific associations with atherosclerotic CVR remain unclear.
Although previous evidence27 suggested that categorical disease activity classification may be a stronger indicator of CVR compared with per-point numerical increments in SLE, the presence of LLDAS in two-thirds of patients with plaques in our study may explain the low impact of disease activity as a potential risk classifier. LLDAS, as well as PDD and aPLpos, was not found to be associated with the presence of plaques in our study. However, because of variations in prevalence of risk factors,14 33 CVRFs may not linearly correspond to risk classifiers, especially for patients at lower CVR14 such as the majority of those examined in our study.
The lower prevalence of plaques in low-risk patients most probably accounts for the lesser impact of SCORE plus VUS assessment on LLT eligibility compared with the moderate-risk group. Our findings showing that more patients would be eligible for LLT according to SCORE plus disease features compared with SCORE alone seem to corroborate previous limited evidence on the better performance of SLE-specific tools to capture actual risk compared with generic risk prediction models.4 34 35 Nevertheless, pending further investigation, due to the substantial difference between LLT eligibility guided by SCORE plus disease-related CVRFs and SCORE plus VUS, routine use of these risk enhancers would require further investigation and decisions on an individual basis (eg, presence of multiple CVRFs in patients at the low-to-moderate risk threshold).
In our study, refinement of risk classification by VUS seemingly had a greater impact on LLT eligibility compared with the use of potential disease-related risk classifiers. However, given that cfUS as a reference rater included cUS, results about the difference in the magnitude of effect between use of SCORE plus cUS and SCORE plus SLE features in comparison to SCORE plus cfUS should be interpreted with caution.
Notwithstanding the relative impact of disease-related features on CVR classification in our study, their use to guide LLT would be justified only after the identification of specific thresholds qualifying them as risk classifiers, similarly to the use of VUS according to ESC guidelines.12 14 Incorporation of disease-specific CVRFs as risk classifiers has also been introduced in other high-CVR diseases such as the level of proteinuria in DM12 14 or the type of extra-articular manifestations in RA.25 The sole presence of SLE4 5 12 or of an SLE-related feature not satisfying the definition of a risk enhancer to modify SCORE classification, as those demonstrated in the present study, would not be sufficient to initiate LLT in these patients.
Strengths of our study include the VUS assessment in a well-characterised cohort of patients with SLE, the previous validation of SCORE in the Greek population,14 the evaluation of major disease-related features (as reported by EULAR recommendations4 5) as potential risk enhancers, and the assessment of the impact of risk classifiers in both low-risk and moderate-risk patients as recommended by the ESC.12 14 The predominance of Caucasians followed up at a tertiary academic centre limits the generalisability of the results to other ethnic groups and healthcare settings.
In conclusion, our findings support the use of VUS and disease-specific characteristics in addition to SCORE for risk classification to guide LLT eligibility in SLE. Glucocorticoid exposure and aPLpos improve risk classification for LLT eligibility at comparable levels in moderate-risk patients, while disease duration seems to have a lesser impact. Future research in cardiovascular health in SLE is needed to define the role of VUS and disease features as risk qualifiers for lipid management in patients classified at low risk according to SCORE.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Scientific Board, Laiko General Hospital, Athens, Greece (study number SB: 1790). The participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors are grateful to all patients for their participation in the study and thank the reviewers for their helpful comments.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors GCD: conceptualisation, methodology, investigation, resources, data curation, writing (original draft, review and editing) and visualisation. GK: investigation, data curation and formal analysis. PPS: investigation and resources. MGT: conceptualisation, methodology, investigation, resources and writing (review and editing), supervision and project administration, guarantor. All authors contributed to data interpretation and gave the final approval of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.