Article Text

Abstract
Objective Spondyloarthritis (SpA) can encompass axial, peripheral and extra-articular disease manifestations. Patients are classified as axial or peripheral SpA depending on the presence or absence of current back pain, independently of the other disease manifestations. Therefore, we aimed to assess the percentage of patients with axial SpA with peripheral disease and how this peripheral disease contributes to the overall disease activity.
Methods Prevalence and disease activity of peripheral disease manifestations were assessed in a real-life observational cohort of 314 patients with the clinical diagnosis of SpA and fulfilling the Assessment of SpondyloArthritis international Society (ASAS) criteria.
Results Of the 314 patients fulfilling the ASAS criteria, 230 fulfilled the axial and 84 the peripheral SpA criteria. Of the 230 patients with axial SpA, 49% had purely axial disease without peripheral disease manifestations whereas 51% had combined axial (back pain) and peripheral (arthritis, enthesitis and/or dactylitis) disease. The latter group had the highest disease activity in comparison with pure axial SpA as well as with peripheral SpA.
Conclusion Half of the patients classified as axial SpA according to the ASAS criteria also have peripheral disease manifestations such as arthritis, enthesitis and/or dactylitis. These peripheral disease manifestations contribute significantly to overall disease activity.
- spondyloarthritis
- ankylosing spondylitis
- disease activity
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Patients with spondyloarthritis (SpA) can present with axial disease, peripheral disease, or a combination of both. However, they are classified as axial or peripheral. The combination of both axial and peripheral manifestations is therefore not well.
What does this study add?
This study demonstrates that half of the patients with 'axial' disease have in fact a combination of axial and peripheral disease. Moreover, these patients have higher disease activity than those with 'pure' axial disease.
How might this impact clinical practice?
The data suggest that it remains crucial to assess the overal disease activity and the different domains of the disease, even when classified as axial disease. Treating accordingly may improve outcome.
Introduction
Spondyloarthritis (SpA) is a chronic inflammatory disease with a heterogeneous clinical presentation, which can include axial, peripheral and extra-articular (skin, gut and eye) disease manifestations. Traditionally, SpA was divided in subtypes based on phenotypic presentation. However, recent insights in the taxonomy of the disease do not justify this phenotypic classification as data from family and genetic studies,1–5 response to treatment6–9 and immunopathology10–13 rather suggest a single disease with overlapping but distinct pathophysiology for axial versus peripheral disease.14 This taxonomy parallels the Assessment of SpondyloArthritis international Society (ASAS) classification criteria distinguishing axial and peripheral SpA.15 16
One potential issue with the classification into axial versus peripheral SpA is that approximately 30% of patients with SpA have both axial and peripheral involvement.15 17 The ASAS criteria prespecify that patients with current back pain and peripheral disease manifestations (arthritis, enthesitis and/or dactylitis) are classified as axial SpA, independently of which disease manifestations predominate in terms of disease activity and burden. When inappropriately applied by different stakeholders (including rheumatologists and also other healthcare professionals, regulators and payers), this classification may thus potentially lead to an underestimation of the prevalence and disease activity of peripheral disease in SpA. Therefore, this study aimed to systematically assess the prevalence and activity of peripheral disease in axial and peripheral SpA as defined by the ASAS criteria in a large, real-life observational cohort.
Methods
Patient cohort
We included patients via the specialised SpA outpatient clinic at the Academic Medical Center/University of Amsterdam between June 2007 and August 2012 (n=272) and at the University Medical Center Utrecht between January 2011 and August 2012 (n=42) in this cross-sectional observational study. Patients were at least 18 years old, were clinically diagnosed with SpA by the rheumatologist and fulfilled the ASAS criteria.15 16 We collected demographic and disease characteristics, HLA-B27 status and X-rays of the sacroiliac joints at the first visit. Locally trained readers scored the X-rays according to the modified New York (mNY) criteria.18 The rheumatologist recorded and measured the patient’s and physician’s global assessment of disease activity, Bath Ankylosing Spondylitis Disease Activity (BASDAI),19 Ankylosing Spondylitis Disease Activity Score (ASDAS) based on the C reactive protein (CRP),20 66/68 swollen joint count and tender joint count, 10 cm Schober test, chest expansion, CRP, erythrocyte sedimentation rate (ESR) and use of medication every 3 months. The treating rheumatologist documented and evaluated the presence (past or present) of psoriasis, uveitis and inflammatory bowel disease (IBD) according to the definition of the ASAS criteria.16 A family history of SpA was defined as at least one first-degree or second-degree family member with ankylosing spondylitis (AS), psoriasis, IBD, reactive arthritis or uveitis. Enthesitis and dactylitis were defined as a clinically apparent enthesitis/dactylitis score >0 by the treating rheumatologist. Peripheral disease manifestations were defined as clinical apparent arthritis, enthesitis or dactylitis diagnosed by the rheumatologist at the current visit or a documented diagnosis by a rheumatologist at an earlier time point. The treating rheumatologist recorded the presence of active back pain and a history thereof. Patients were treated according to standard clinical patient care, hence all therapies were allowed. For the current study, we used data of the patients’ first visit to the SpA outpatient clinic.
Statistical analysis
Categorical data are presented as numbers (%), continuous data as mean (SD) or as median (IQR) as appropriate. We used χ2 test for categorical data and Mann-Whitney U test or unpaired t-test for continuous data. Statistical tests were two-sided, and p values less than 0.05 were considered significant.
Results
Patient characteristics and disease activity in axial SpA versus peripheral SpA
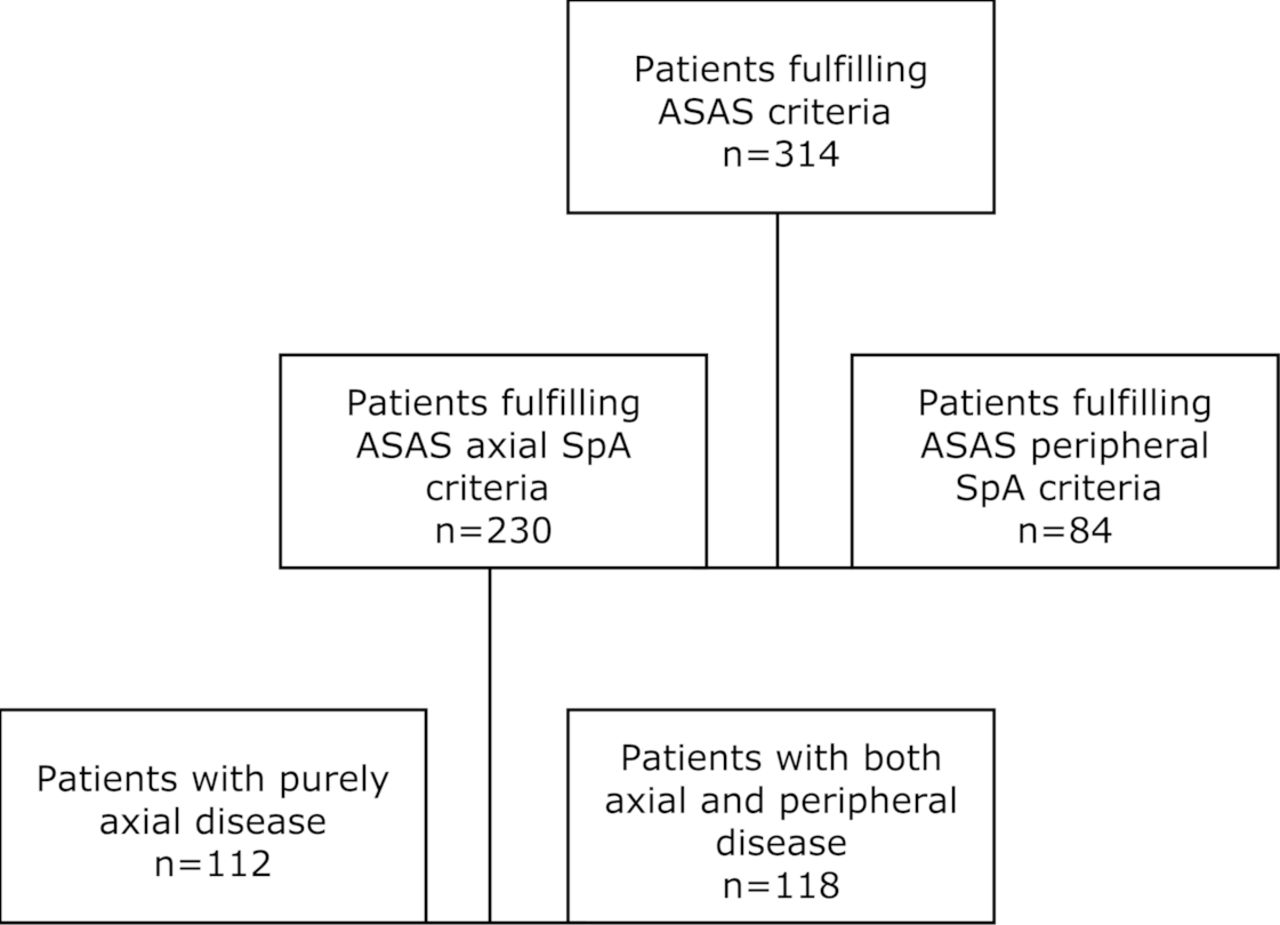
Of the 314 patients with SpA fulfilling the ASAS criteria, 230 patients fulfilled the ASAS axial SpA criteria and 84 patients fulfilled the peripheral SpA criteria (73.2% vs 26.8%) (figure 1). The demographic and clinical characteristics of both patient groups are summarised in table 1. The mean age of the patients with ASAS axial SpA was 41 (33–52) compared with 48 (37–56) for the patients with ASAS peripheral SpA (p=0.005). Of the 230 patients with ASAS axial SpA, 145 were men, compared with 49 of the 84 patients with ASAS peripheral SpA (63% vs 58%, p=0.447). Patients with ASAS axial SpA had an earlier disease onset (32 (24–41) years) than patients with ASAS peripheral SpA (38 (31–48) years, p=0.001). Of the 230 patients with ASAS axial SpA, 170 were HLA-B27 positive, compared with 18 of the patients with ASAS peripheral SpA (76% vs 27%, p<0.001). All of the 230 patients with ASAS axial SpA had current back pain, compared with 18 of the 84 patients with ASAS peripheral SpA (only past back pain) (100% vs 21%, p<0.001), and 161 of the 230 patients with ASAS axSpA fulfilled the mNY criteria versus 0 of the 84 patients with ASAS peripheral SpA (70% vs 0%, p<0.0001). Arthritis (p<0.001), enthesitis (p<0.001) and dactylitis (p=0.009) were more frequent in patients with ASAS peripheral SpA (table 1), as were psoriasis (p<0.001) and IBD (p=0.004). In contrast, but in line with the frequency of HLA-B27, uveitis was more prevalent in axial SpA (p<0.001). A positive family history was observed in 86 of the patients with ASAS axial SpA and in 23 of the patients with ASAS peripheral SpA (37% vs 27%, p=0.099).
{kind=link}
Flow chart of patients included in the cohort according to the fulfilment of the Assessment of SpondyloArthritis international Society (ASAS) criteria. SpA, spondyloarthritis.
Clinical characteristics, disease activity and treatment of ASAS axial spa versus ASAS peripheral SpA
Disease activity measurements specifically developed for axial SpA activity were higher in axial than in patients with peripheral SpA. On the contrary, CRP and ESR levels as markers of systemic inflammation were comparable between both groups (table 1). Remarkably, besides composite parameters originally developed for axial disease (although also taking into account peripheral disease manifestations)—such as ASDAS-CRP and BASDAI—also global disease activity parameters (patient’s and physician’s global assessment) were significantly higher in axial than in peripheral SpA (p<0.001 for all four comparisons). Analysis of patients naive to tumour necrosis factor-alpha (TNF-α) blocking therapy did not alter these results (data not shown).
Non-steroidal anti-inflammatory drug (NSAID) use was higher and corticosteroid and conventional synthetic disease-modifying antirheumatic drug (csDMARD) use was lower in the ASAS axial SpA group (all p<0.05, table 1) as a reflection of standard clinical care. TNF-α inhibitor usage was similar between patients fulfilling the ASAS axial versus ASAS peripheral SpA criteria.
Patients with purely axial and combined axial and peripheral SpA
The ASAS criteria exclude patients with active axial symptoms from the peripheral SpA group but do not exclude patients with active peripheral symptoms from the axial SpA group. Our results show that peripheral arthritis as well as enthesitis occurred each in more than 30% of the patients with axial SpA (table 1). Therefore, we additionally differentiated the 230 patients fulfilling the ASAS axial SpA criteria into purely axial disease (without concomitant arthritis, enthesitis and/or dactylitis) (n=112, 48.7%) and combined disease (axial SpA with concomitant arthritis, enthesitis or dactylitis) (n=118, 51.3%) (figure 1). Table 2 shows the characteristics of patients with purely axial SpA and combined axial and peripheral SpA.
Clinical characteristics, disease activity and treatment of patients with purely axial SpA and combined axial and peripheral SpA
The mean age of the patients with purely axial SpA was 39 (32–48) compared with 44 (34–54) for the patients with combined SpA (p=0.064). Seventy of the 112 patients with purely axial SpA were men, compared with 75 of the patients with combined SpA (63% vs 64%, p=0.868). The patients with purely axial SpA had a mean disease onset at 32 (23–38) years, patients with combined SpA at 34 (24–44) years. Of the 112 patients with purely axial disease, 86 were HLA-B27 positive, compared with 84 of the patients with combined SpA (80% vs 72%, p=0.163).
By definition, none of the 112 patients with purely axial SpA had peripheral arthritis, enthesitis or dactylitis, of the patients with combined SpA, 75, 73 and 9 patients had peripheral arthritis, enthesitis or dactylitis, respectively (p≤0.001, p≤0.001 and p=0.003). Of the 112 patients with purely axial SpA, seven had psoriasis, and of the patients with combined SpA, 16 had psoriasis (6% vs 14%, p=0.065). Seven of the 112 patients with purely axial SpA had IBD, compared with 7 of the 118 patients with combined SpA (p=0.920). Of the patients with purely axial SpA, 41 had a positive family history for SpA, compared with 45 of the patients with combined SpA (37% vs 45%, p=0.811).
The median patient’s global assessment was 52 (23–68) in patients with purely axial SpA and 61 (45–75) in patients with combined SpA (p=0.0010). The median physician’s global assessment in patients with purely axial SpA was 44 (16–60) compared with 53 (33–62) in combined SpA (p=0.009). The median BASDAI was 4.4 (2.9–6.0) in patients with purely axial SpA and 5.4 (4.0–6.6) in patients with combined SpA (p=0.001). The median ASDAS-CRP level was 2.6 (1.8–3.5) in patients with purely axial SpA and 3.0 (2.2–3.7) in patients with combined axial and peripheral SpA (p=0.014). There was no significant difference in CRP and ESR levels. The group with combined axial and peripheral disease retained the highest disease activity after exclusion of patients treated with anti-TNF therapy (data not shown). Of the 112 patients with purely axial SpA, five used any csDMARD, compared with 27 of the patients with combined disease (5% vs 23%, p≤0.001).
Peripheral disease in combined axial versus peripheral SpA
To further assess the potential relevance of peripheral disease in the group of ASAS axial SpA, we compared peripheral disease features and treatments between combined SpA and peripheral SpA. Patients with combined SpA had a higher prevalence of enthesitis than patients with peripheral SpA (62% vs 48%, p=0.044) but a lower prevalence of peripheral arthritis (63% vs 98%, p<0.001). Dactylitis prevalence was not different between both groups. Prevalence of psoriasis and IBD was higher in patients with peripheral SpA (54% vs 14%, p<0.001% and 17% vs 6%, p=0.014, respectively) while uveitis prevalence was higher in patients with combined SpA than in peripheral SpA (26% vs 6.0%, p<0.001). Patients with combined SpA used NSAIDs more frequently than patients with peripheral SpA (74% vs 56%, p=0.008), and patients with combined SpA used csDMARDs less frequently than patients with peripheral SpA (23% vs 67%, p<0.001).
Discussion
In this real-life observational cohort of 314 patients with SpA, we investigated the clinical characteristics and disease activity of axial and peripheral SpA according to the ASAS criteria, leading to the following conclusions: (1) patients classified as axial SpA according to the ASAS criteria in fact consist of two separate groups of equal size—patients with exclusively axial disease and patients with combined axial and peripheral disease, defined as active back pain plus arthritis, enthesitis and/or dactylitis; (2) patients with combined axial and peripheral disease consistently showed higher disease activity than patients with purely axial disease; and (3) patients with combined axial and peripheral disease were less often treated with csDMARDs than patients with purely peripheral SpA.
In line with previous reports, axial SpA was more prevalent than peripheral SpA and was associated with specific features such as younger age, higher prevalence of HLA-B27 and uveitis, and lower prevalence of psoriasis and IBD.21 And in line with treatment guidelines,22 a majority of axial SpA was treated with NSAID whereas the use of csDMARDs was higher in peripheral SpA. The overall disease activity, as evaluated by patient’s and physician’s global assessment of disease activity as well as composite indices such as BASDAI and ASDAS, was higher in axial SpA but did not lead to a higher use of highly effective targeted therapies such as TNF inhibition, suggesting that treatment was not completely tailored to disease activity. For the sake of clarity, it needs to be specified there are no major restrictions to access to TNF inhibition in the Netherlands and that other targeted therapies, such as IL-17 inhibition, were not available at the time of this cross-sectional cohort study.
A striking finding in this axial versus peripheral SpA analysis was the fact that 21% of the patients with peripheral SpA had a history of back pain. The back pain can be explained by the fact that the criteria for axial SpA require present back pain; therefore, a patient with peripheral SpA and a history of back pain will still be classified as peripheral SpA and it remains unknown if this back pain is related to SpA or to other, concomitant conditions such as degenerative disc disease. This question could be addressed by MRI of the axial skeleton in these patients, an approach that was not systematically applied in the current study.
The main finding of the study, however, is that half of the patients with axial SpA also have signs of peripheral disease. Further analysis of ‘pure axial SpA’ versus combined axial and peripheral SpA revealed that, although both subgroups were very similar in terms of demographics, HLA-B27 positivity, family history and presence of extra-articular manifestations, the combined SpA had significantly higher disease activity despite increased use of csDMARDs. Moreover, a comparison with peripheral SpA revealed that patients with combined SpA used less csDMARDs despite higher disease activity (data not shown). Interestingly, we noted that the higher disease activity in combined SpA did not translate in higher use of TNF inhibition in this patient subset. Whereas cDMARDs are not effective for axial disease23–25 and may have limited efficacy for peripheral disease,23 25–27 it is well established that TNF inhibition is effective for both axial and peripheral disease.28–37 In the setting of the current study, patients with combined axial and peripheral SpA are eligible for targeted therapies and access to TNF inhibition was not restricted. Collectively, these data therefore indicate that patients with combined axial and peripheral disease form an important subgroup of patients with axial SpA as defined by the ASAS criteria as they represent half of the patients with axial SpA and have a higher disease activity. However, they do not appear to be treated ‘to target’ based on disease activity, suggesting that the additional disease activity related to concomitant peripheral disease is underestimated in axial SpA.
Our study has limitations. First, identifying the impact of each individual peripheral disease manifestation (arthritis vs enthesitis vs dactylitis) would be of interest. To that purpose, we have divided the patients with ASAS axSpA into subgroups with arthritis, enthesitis and dactylitis and measured the disease activity in those subgroups. However, since disease manifestations largely overlapped (roughly half of the patients with arthritis also had enthesitis, two-thirds of the patients with dactylitis also had enthesitis and two-thirds of the patients with dactylitis also had arthritis, data not shown), the influence of each individual peripheral disease manifestation should me measured in other, larger axSpA populations. Second, for this analysis, we did include only those patients clinically diagnosed with axial SpA and fulfilling the ASAS axial SpA criteria since the classification criteria were developed to define homogeneous patient groups for clinical research. Including only patients fulfilling the criteria might potentially induce selection bias. However, including the 75 patients who did not fulfil the ASAS criteria did not change the results (data not shown).
Although the design of this cross-sectional cohort study did not allow to test the possible advantage of treatment intensification in patients with SpA with combined axial and peripheral disease, several other study approaches might help to increase recognition and appropriate treatment of peripheral disease in patients classified as axial SpA. For example, several previous studies used the ASAS criteria differently than postulated—that is, classifying patients with both axial and peripheral disease exclusively as axial SpA—in order to better justify the real phenotype of the patients. The Leiden early arthritis cohort applied the ASAS peripheral SpA criteria in patients with early arthritis with a history of or current back pain,38 whereas strictly the ASAS axial SpA criteria should be applied in case of back pain. The Cochin SpondyloArthritis study cohort of patients with established SpA used either the ASAS axial or peripheral SpA criteria based on the predominant manifestation.39 A study within the ESPERANZA programme analysing the performance of the ASAS criteria in early SpA applied the axial SpA criteria only in patients with exclusively back pain and the peripheral SpA criteria only in patients with peripheral arthritis, dactylitis or enthesitis in the absence of axial pain,40 which is also not in line with the ASAS classification criteria. A study assessing the prevalence of SpA in southern Sweden concluded that 57% fulfilled the ASAS classification criteria for peripheral SpA, 91% the ASAS classification criteria for axial SpA and that 45% of this latter group also fulfilled the ASAS criteria for peripheral SpA,41 while according to the ASAS criteria fulfilling both sets of criteria is not an option. Finally, in our proof-of-concept clinical trial with adalimumab in non-AS, non-PsA peripheral SpA according to the European Spondyloarthritis Study Group (ESSG) criteria post hoc application of the ASAS criteria revealed that 38/40 patients would fulfil the ASAS criteria for peripheral SpA if not taking into account that 22/40 patients also had current back pain when questioned for axial complaints.33 Theoretically, we could use the ASAS criteria differently and either classify patients according to the most prominent disease manifestation (rather than use axial SpA as a starting point) or classify them as axial, peripheral, or axial and peripheral SpA.
The key question, however, is if merely changing the criteria would impact recognition and treatment of peripheral disease in clinical practice. It may be more relevant to maintain the current classification but clarify in management and treatment guidelines how this should be applied. Careful evaluation and monitoring of peripheral disease (and similarly: extra-articular manifestations and comorbidities) remains needed in all patients with SpA, even in the axial SpA subset. And treatment decisions should be based on axial disease targets and/or peripheral disease targets and also should include composite indices and/or patient reported outcomes (PROs) reflecting the global disease activity where appropriate.6 42 An example of such an approach is the Minimal Disease Activity in psoriatic arthritis, which includes different domains of the disease.43 44 Interestingly, we previously demonstrated that both BASDAI and ASDAS perform well in peripheral SpA.45 Therefore, it would be relevant to evaluate in a real-life study if systematic use of these tools to monitor disease activity and guide treatment decisions—for axial SpA and also for combined axial and peripheral SpA—may favourably impact outcome in purely axial SpA and also combined axial and peripheral SpA.
Half of the patients classified as axial SpA according to the ASAS criteria also have peripheral disease manifestations such as arthritis, enthesitis and/or dactylitis. These patients have higher disease activity than patients with purely axial SpA and patients with peripheral SpA. Further research should (1) assess in a longitudinal study if the additional disease activity related to concomitant peripheral disease negatively impacts the burden of disease and long-term outcome in axial SpA, and (2) evaluate whether adaption of the classification criteria and/or systematic monitoring of disease activity using composite indices may lead to better recognition and treatment of peripheral disease in axial SpA.
Acknowledgments
We would like to thank all physicians working in the SpA outpatient clinics during the inclusion of the study. This manuscript partly overlaps with chapter 5 of the PhD thesis of JEP, one of the authors of this manuscript.
References
Footnotes
Contributors All authors were involved in drafting the article or revising it critically for important intellectual content, and all authors approved the final version to be published.
Funding DLB was supported by a VIDI grant from The Netherlands Organization for Scientific Research (NWO), by a grant from the Dutch Arthritis Foundation (Reumafonds) and by a grant from the European Research Council (ERC).
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Approved by the Medical Ethics Committee of the Academic Medical Center/University of Amsterdam, Amsterdam, the Netherlands and by the Medical Ethics Committee of the University Medical Center Utrecht, Utrecht, the Netherlands.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.