Article Text

Abstract
Objective Inoperable chronic thromboembolic pulmonary hypertension (CTEPH) managed medically has a poor prognosis. Balloon pulmonary angioplasty (BPA) offers a new treatment for inoperable patients. The national BPA service for the UK opened in October 2015 and we now describe the treatment of our initial patient cohort.
Methods Thirty consecutive, inoperable, anatomically suitable, symptomatic patients on stable medical therapy for CTEPH were identified and offered BPA. They initially underwent baseline investigations including Cambridge Pulmonary Hypertension Outcome Review (CAMPHOR) quality of life (QoL) questionnaire, cardiopulmonary exercise test, 6 min walk distance (6MWD), transthoracic echocardiography, N-terminal probrain natriuretic peptide (NT pro-BNP) and right heart catheterisation. Serial BPA sessions were then performed and after completion, the treatment effect was gauged by comparing the same investigations at 3 months follow-up.
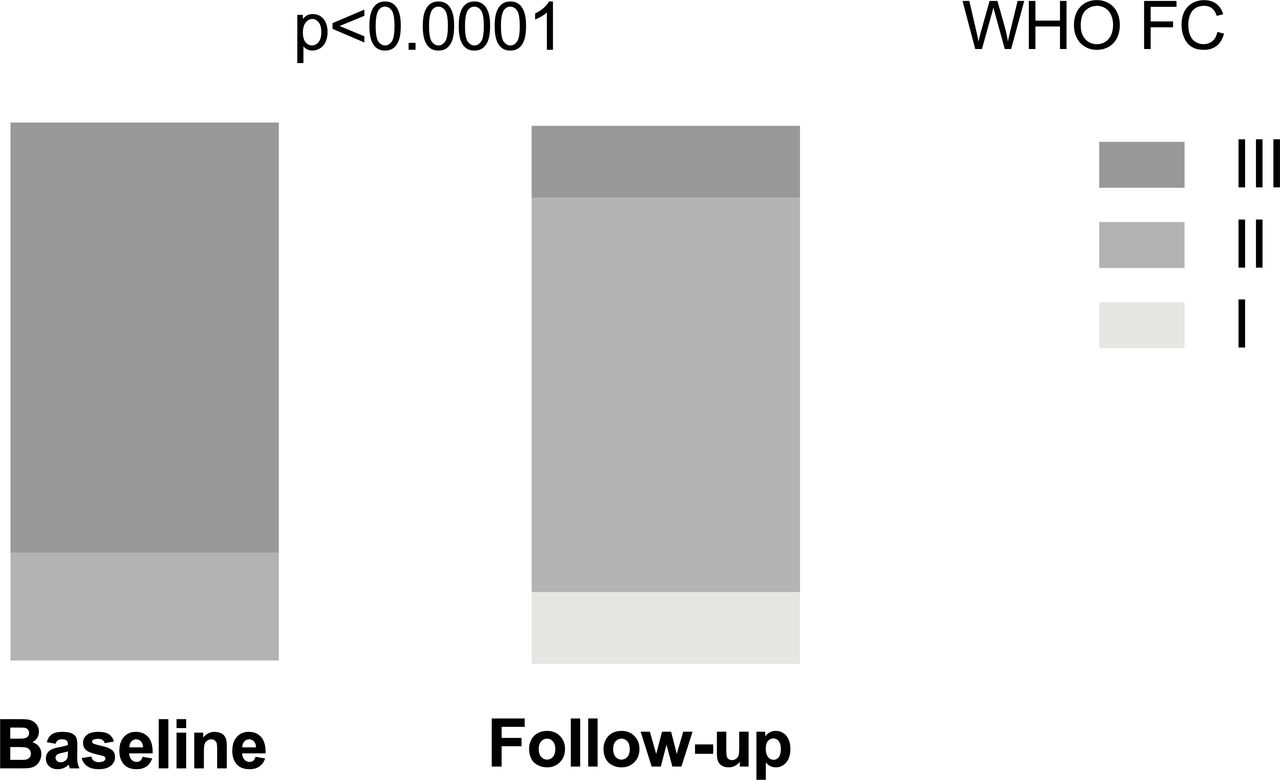
Results A median of 3 (IQR 1–6) BPA sessions per patient resulted in a significant improvement in functional status (WHO functional class ≥3: 24 vs 4, p<0.0001) and QoL (CAMPHOR symptom score: 8.7±5.4 vs 5.6±6.1, p=0.0005) with reductions in pulmonary pressures (mean pulmonary artery pressure: 44.7±11.0 vs 34.4±8.3 mm Hg, p<0.0001) and resistance (pulmonary vascular resistance: 663±281 vs 436±196 dyn.s.cm-5, p<0.0001). Exercise capacity improved (minute ventilation/carbon dioxide production: 55.3±12.2 vs 45.0±7.8, p=0.03 and 6MWD: 366±107 vs 440±94 m, p<0.0001) and there was reduction in right ventricular (RV) stretch (NT pro-BNP: 442 (IQR 168–1607) vs 202 (IQR 105–447) pg/mL, p<0.0001) and dimensions (mid RV diameter: 4.4±1.0 vs 3.8±0.7 cm, p=0.002). There were no deaths or life-threatening complications and the mild-moderate per-procedure complication rate was 10.5%.
Conclusions BPA is safe and improves the functional status, QoL, pulmonary haemodynamics and RV dimensions of patients with inoperable CTEPH.
- Balloon pulmonary angioplasty
- Chronic thromboembolic pulmonary hypertension
- Right heart function
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Balloon pulmonary angioplasty (BPA) is emerging as a viable treatment for patients with inoperable chronic thromboembolic pulmonary hypertension (CTEPH). Studies have shown it improves symptoms, pulmonary haemodynamics and in a limited number of series right heart size and function. However, many of the patients treated to date would have received pulmonary endarterectomy (PEA) in the UK, and therefore, it was important to confirm the therapeutic effect of BPA on a UK cohort of patients with inoperable CTEPH.
What does this study add?
We describe the initial UK experience of BPA delivered within the national CTEPH service with a highly experienced PEA surgical service. We show that BPA performed in patients with inoperable disease, on established PH-targeted therapy and delivered with a focused approach (targeting predominantly basal subsegmental disease distribution and with fewer treatment cycles than previous reports) safely derives benefits of comparable magnitude to other series. We also demonstrate for the first time improvement in patient quality of life measured by Cambridge Pulmonary Hypertension Outcome Review questionnaire and provide compelling data on improvements in cardiopulmonary exercise testing, biomarker levels and right ventricular remodelling/function which are important prognostic surrogates.
How might this impact on clinical practice?
These data clearly show BPA is an effective and safe treatment for patients with inoperable CTEPH. We believe that BPA is now sufficiently developed that appropriately powered randomised controlled trials comparing subsegmental PEA verses BPA and BPA verses PH-targeted therapy can be planned to guide optimal treatment strategy for patients with CTEPH.
Introduction
Chronic thromboembolic pulmonary hypertension (CTEPH) is a condition caused by failure of resolution of pulmonary emboli (PE) and results in fibrotic tissue deposition that occludes the pulmonary arteries.1 CTEPH has an incidence of 0.9–5.7 cases per million and a prevalence of 8–40 cases per million although this is likely to be an underestimate as the condition is often under-reported.2 3 It has been estimated that between 0.56% and 3% of acute PE develop CTEPH.4 Mechanical obstructions and secondary pulmonary vasculopathy cause pulmonary hypertension, right ventricular (RV) remodelling and dilatation culminating in a worsening exercise tolerance, right heart failure and early death.5 Survival at 3 years in unoperated patients is 70% and is not affected by medical therapy, although preliminary data suggest that the soluble guanylate cyclase (sGC) riociguat may improve medium-term survival.6
Pulmonary endarterectomy (PEA) is an established therapeutic intervention and is the guideline recommended treatment for patients with CTEPH.7–9 It is, however, a major surgical procedure and associated with an intraoperative mortality of around 2.2% and a major complication rate of nearly 50%, even in the most experienced centres and therefore for some the risks may outweigh the potential benefit.10 In addition, due to distal distribution of thromboembolic changes, PEA may not be technically feasible. As a result approximately 40% of patients are inoperable and of those undergoing PEA 20% may have incomplete clearance and persistent functional limitation.11 Those patients with inoperable or residual CTEPH may either be treated with PH—targeted medical therapy, for which there is short-medium term evidence of haemodynamic and symptomatic improvement12–15 and/or balloon pulmonary angioplasty (BPA) for which there is only observational evidence to date.16 17
BPA is a novel technique, initially described by Feinstein et al18 in the USA and then refined in Japan and Europe over the past 15 years,19 where balloon mounted catheters are introduced over a guide wire into pulmonary segmental and subsegmental diseased vessels and inflated to unblock them and restore flow. Contemporary data provide compelling evidence of the benefits of BPA with improvements in both symptoms and haemodynamics noted.20 Meta-analysis data suggest that the effects of BPA may be superior to medical therapy and possibly equivalent to PEA,16 although no randomised control data comparing treatment strategies has been published to date. Reassuringly the effects of BPA appear durable out to 5 years, with restenosis being a rare occurrence.21 22 However, the reported therapeutic effect of BPA may be affected by the phenotypic differences in those offered BPA; many patients included in the early BPA studies had surgically operable disease. The effect of BPA in patients with inoperable disease and residual disease after PEA remains uncertain, as does the optimal interventional strategy employed and further studies are required.
Methods
New service and patient pathway
The national BPA service at Royal Papworth Hospital, which also hosts the national CTEPH service and has one of the largest PEA experiences worldwide, was set up in 2015 supported by a charitable grant. Patients with CTEPH are referred to the national CTEPH multidisciplinary team (MDT) meeting for initial consideration of PEA. Only patients deemed inoperable but who potentially have BPA-treatable disease are invited for a conventional pulmonary angiogram and rediscussion at a BPA MDT meeting. Patients are accepted only if symptomatically limited despite PH-targeted medical therapy and where territories with normal or near normal lung parenchyma have reduced lung perfusion subtended by anatomically treatable vessels evident on pulmonary angiography without procedural contraindications, for example, contrast allergy, severe renal dysfunction, inability to breath-hold or access-site issues. To maximise symptomatic and haemodynamic benefit as well as the available limited resources, a targeted approach has been employed, preferentially selecting lower lobe vessels as the primary targets for BPA. Those accepted for BPA are invited to clinic for detailed counselling and written patient information, included within a bespoke consent form. Those patients who agree to proceed are then listed for their procedure.
As per international guidelines,23 prior to the first procedure patients are maintained on PH-targeted therapy and this is not modified during the periprocedural period. Patients then undergo a series of clinically driven preprocedural tests the day before their first BPA procedure that include: cardiopulmonary exercise test (CPET), transthoracic echo, pulmonary function test, blood tests including N-terminal probrain natriuretic peptide (NT-proBNP), 6 min walk distance (6MWD), assessment of functional class (FC), Cambridge Pulmonary Hypertension Outcome Review (CAMPHOR)—a disease-specific patient-reported assessment of quality of life (QoL), where a high score indicates worse symptoms, activity level and QoL24 and right heart catheter (immediately prior to their first BPA). At completion of treatment, they are invited back at 3 months follow-up for assessment of their response guided by repeating the above tests.
Treatment algorithm
This report includes the first 30 consecutive patients treated by BPA at our centre between October 2015 and April 2018.
Preprocedure
Patients stop warfarin 5 days before their procedure and were commenced on bridging, therapeutic dose, low-molecular-weight heparin (LMWH) until the day before admission if their INR (International Normalised Ratio) was <2. Where a direct oral anticoagulant was used these were omitted the day before the procedure without LMWH bridging. In addition to the investigations mentioned above, blood for renal function, haemoglobin, INR (for those on warfarin) and cross-matching was drawn. Patients were nil by mouth for 8 hours before the procedure, although clear fluid was permitted up to 4 hours.
BPA procedure
Procedures were performed under conscious sedation (remifentanyl initially to suppress cough and then midazolam) with anaesthetic support. Oxygen was supplied via nasal cannulae and the saturations monitored non-invasively. In our early experience, a radial arterial sheath was used to monitor systemic pressure during the procedure but this was quickly abandoned. A 6 French sheath was then placed in the right femoral vein under local anaesthesia and unfractionated heparin (70–100 IU/kg) was administered. Activated clotting time (ACT) was measured after 1 hour if the procedure was prolonged and further heparin administered to achieve an ACT >250 s.
Right heart catheterisation including thermodilution cardiac output assessment (Swan-Ganz catheter, Edwards Lifesciences, Irvine, USA) was performed at the beginning of each procedure as standard. The venous sheath was then exchanged for an 80 cm Shuttle Sheath (Cook Medical, Limerick, Ireland) guided by an angled pigtail catheter (Cardinal Health, Dublin, USA) to advance it into the pulmonary artery to provide guide catheter stability required for the intervention. A digital subtraction cine of the relevant lobe performed (right anterior oblique 30o for the left pulmonary artery and left anterior oblique 30o for the right pulmonary artery to guide the intervention). A long 150 cm exchange length 0.035 inch wire was then used to maintain segmental pulmonary artery position and replace the angled pigtail catheter for either a multipurpose or Judkins right four catheters (Cardinal Health). Subsegmental vessels were then wired with a Whisper medium support wire or occasionally a Pilot 50 wire (Abbott Vascular, Santa Clara, USA) and the lesions were balloon dilated with a 2–4 mm x 20 mm Trek balloon (Abbott Vascular) inflated to between 2 and 8 atmospheres. During the initial learning phase only simple discreet web lesions in one segmental territory were treated per session, but, as experience increased, disease of all types (webs, slits, stenoses and occlusions) were treated and when the haemodynamic were favourable (mean PA pressure <40 mm Hg) multiple lesions within the same lobe were cleared in a single session, although none had bilateral BPA in the same sitting.
Postprocedure
Patients invariably had the femoral venous sheath removed in the catheter lab at the end of the procedure and initially had saturations monitored in a high dependency unit setting overnight. A chest radiograph was also routinely requested to assess for early radiological evidence of reperfusion oedema or bleeding. More recently patients have been observed in a theatre recovery for an hour and then returned to the respiratory ward for 4 hours bed rest. Patients with an uncomplicated procedure are recommenced on their oral anticoagulant (with LMWH bridging for those treated with warfarin until the INR is >2) and PH-targeted therapy on the same evening as their procedure and are usually discharged the next day.
Repeated sessions following the same treatment algorithm were performed at monthly intervals as long as there remained suitable targets for BPA and patients continued to be symptomatic. This interval treatment limited to one side at a time minimises the risk of complications. At completion patients were invited back for review at a 3-month follow-up appointment.
Statistical analysis
To assess the efficacy of BPA, the clinical parameters recorded at baseline and 3-month follow-up were compared. Categorical variables were presented as numbers and percentages and compared with the use of the X2 test or Fisher’s exact test. Continuous variables were compared as means (SD) with Student’s t-test for normally distributed data or median (IQR) by Pearson’s coefficient for non-parametric data, as appropriate. A two-sided p<0.05 was considered to indicate statistical significance.
Results
The number of referrals to the national CTEPH MDT meeting between October 2015 and April 2018 and their subsequent allocation to therapy is summarised in figure 1. Of the 943 patients with CTEPH referred, 389 patients had inoperable disease and 93 were then considered for BPA at the MDT meeting. Of these, 47 patients were offered BPA. Four patients declined, 13 were awaiting BPA and 30 completed a course of BPA treatment within the time period and attended for 3-month follow-up. These 30 patients had a mean age of 63.5±11.6 years and were predominantly male (n=22, 73%). All were anticoagulated and most were taking PH-targeted therapy (no therapy (did not tolerate): n=2; monotherapy: phosphodiesterase inhibitor (PDEi) n=12, endothelin receptor antagonist (ERA) n=1, sGC n=7; combination therapy: ERA+PDEi n=6, ERA +sGC n=2) that was not altered during their BPA treatment cycles and follow-up. Despite these drug therapies, patients remained highly symptomatic before BPA, as evidenced by a baseline WHO FC of 3 in 24/30 (80%) and a mean CAMPHOR symptom score of 8.7 at baseline. Their baseline pulmonary haemodynamics were deranged with a mean pulmonary artery pressure (mPAP) of 44 mm Hg and a pulmonary vascular resistance (PVR) of 660 dyn.s/cm5, as well as evidence of a pressure loaded right ventricle with dilatation, altered geometry and early signs of RV decompensation (table 1).

Patient flow through the National CTEPH service. BPA, balloon pulmonary angioplasty; CTEPH, chronic thromboembolic pulmonary hypertension; PEA, pulmonary endarterectomy.
Haemodynamic indices, functional status and right heart function at baseline and at 3 months follow-up after BPA treatment
A total of 95 procedures were undertaken and patients were treated with a median of 3 (IQR 1–6) BPA treatment cycles at monthly intervals focusing predominantly on the basal segmental and sub-segmental vessels; the total number of vessels treated was 198, equally distributed between left and right lung with 183/198 (92%) lesions located in an anterior basal (A8), lateral basal (A9) and posterior (A10) basal arteries of both lungs.
A course of BPA universally improved all haemodynamic parameters (table 1) and in particular significant reductions in mPAP (−21.9±14.1%, p<0.0001) and PVR (−32.4±18.6%, p<0.0001) were observed with more modest improvements in cardiac output (figure 2). This resulted in significant increases in exercise capacity measured by 6MWD (+21.2% ± 27.0%, p<0.0001) and ventilatory efficiency that resulted in an improvement in FC (figure 3) and CAMPHOR score (table 1). The improvement in CAMPHOR was primarily driven by improvement in symptom score (Δ −3.1±4.0, p=0.0005) and activity score (Δ −1.6±3.6, p=0.03) rather than QoL score per se (Δ −1.5±4.8, p=0.11). There was clear biomarker evidence of reduced right heart strain quantified by a reduction in NT-proBNP (−38.4±42.5%, p<0.0001) as well as reverse RV remodelling with beneficial changes in RV geometry, reductions in RV size and improvement in RV function (table 1 and figure 4).

Haemodynamic effect of BPA treatment on (A) mean PAP (B) CO measured by thermodilution and (C) PVR measured by thermodilution. BAP, balloon pulmonary angioplasty; COTD, cardiac output by thermodilution; PAP, pulmonary artery pressure; PVR, pulmonary vascular resistance.
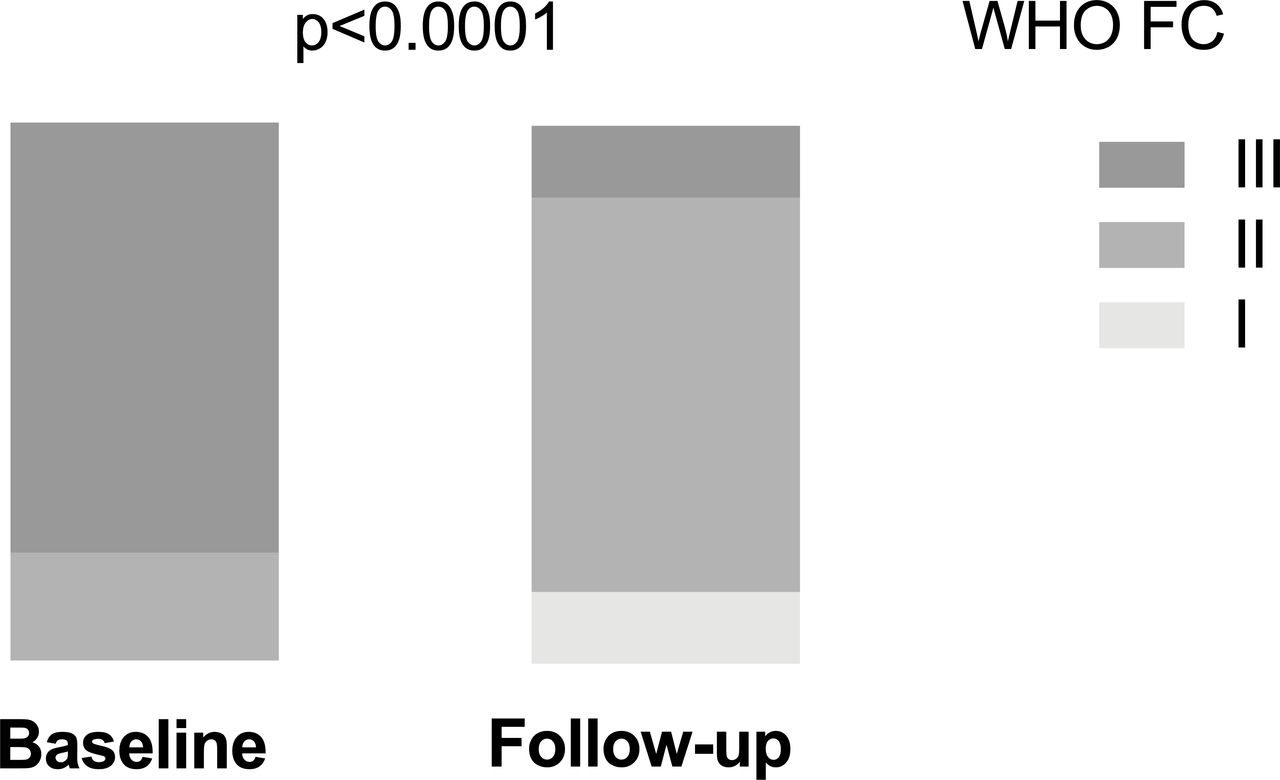
Change in WHO FC of the initial 30 patients treated by BPA. BPA, balloon pulmonary angioplasty; FC, functional class.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
The effect of BPA on the right heart as measured by (A) NT-pro BNP (one high outlier removed from the baseline plot) and (B) mid-cavity RV diameter. BPA, balloon pulmonary angioplasty; NT-pro BNP, N-terminal probrain natriuretic peptide; RV, right ventricular.
This patient benefit came at minimal cost. There were no deaths or life-threatening complications and nor did any patient require intensive care or emergency intubation. In total there were 10 mild-moderate procedure-related complications (a per-procedure rate of 10.5%). There were two access site haematoma, one of which required surgical exploration and a blood transfusion. There were also eight acute lung injuries composed of five procedures complicated by mild haemoptysis (three from distal wire perforations, one of which required placement of a haemostatic coil) and three procedures with lung reperfusion oedema confirmed by chest radiography that all settled with supplementary oxygen therapy and conservative management.
Discussion
We have demonstrated in a non-operable population of patients with predominantly subsegmental distribution CTEPH, as described at the national CTEPH MDT with experienced PEA surgeons present, that BPA delivered with a focused approach, concentrating on lower lobe predominantly subsegmental arteries, can achieve clinically meaningful patient benefits safely with relatively few BPA treatment cycles.
Management of inoperable CTEPH
The cornerstone of therapy is PEA surgery but up to 40% of patients with the disease are not surgical candidates, either due to associated comorbidity or disease burden that fails to justify the risk of major surgery or a distribution of disease that is inaccessible.7 Patients with inoperable CTEPH have a less favourable prognosis and a high symptom burden.4 Recent, double blind, placebo controlled randomised controlled trials of the sGC stimulator—riociguat (Bayer) and ERA—macitentan (Actelion) over a period of 16 weeks have demonstrated modest but significant benefits.13 14 In the chest-1 trial mPAP fell by 10% and the PVR by one-third, while 6MWD increased by just over 10% in the riociguat arm and 33% of patients reported a one-grade improvement in FC. The safety and efficacy of riociguat appears to extend beyond 2 years6 15 although longer-term mortality benefits have not been demonstrated and the treatments are lifelong and expensive.
Efficacy of BPA
BPA may be more effective than medical therapy for the treatment of CTEPH,16 although the study populations may be heterogeneous and the first randomised controlled trial to study this: riociguat versus BPA in non-operable CTEPH (RACE) trial (NCT02634203), has not yet been published. Perhaps in reality the two are complementary—each treating different aspects of the disease process. In a systematic review of published longitudinal cohort studies comparing the ‘before’ and ‘after’ effects of BPA treatment delivered in mean of 2.5–6.6 sessions,20 mPAP reduced by around 14.2 mm Hg, PVR by about 300 dyn.s/cm5, the 6MWD was increased by around 67 m and FC fell by over one grade.
Our data are comparable despite some important differences in approach. First, our patients are from an experienced, national PEA centre and are truly inoperable with distal disease, as exemplified by the higher mPAP and PVR than other reported cohorts. This is important, as the response to BPA may be different when treating more proximal ‘surgical’ disease. Second, the number of BPA sessions we delivered and the number of treated vessels were fewer than other reported data.20 We largely focused our BPA to vessels supplying the lower zones which receive a greater proportion of the cardiac output.25 Relieving the obstruction in these zones is likely to have a greater treatment effect on PVR, achieving symptomatic improvement with fewer treatment cycles. Third, the majority of our patients were on established evidence-based medical therapy, and therefore, the BPA effect we observed was additive. When BPA has been used sequentially in a similar manner, riociguat reduced mPAP from 49 to 43 mm Hg with a further reduction in mPAP to 34 mm Hg and PVR reductions of a further 30% after BPA.26 We saw similar improvements on top of medical therapy in the majority of our patients, confirming that BPA can further offload the right ventricle with clear synergy that may reflect their different disease modifying actions; BPA addresses subsegmental disease whereas medical therapy targets more distal and inaccessible vasculopathy. Fourth, we demonstrate clear benefits in RV geometry, size and function within 3 months of completing a course of BPA. This reverse RV remodelling has been reported before27 28 and improvements in right heart size and function are predictive of adverse outcome.29 Finally, we clearly show for the first time that BPA significantly improves CAMPHOR scores predominantly by improving subjective symptom and activity scores.
Safety of BPA
BPA is an invasive treatment and is associated with complications which are reported at a rate of approximately 10% of procedures in contemporary practice, although where routine CT follow-up is performed, this value may be higher.19 Determining the precise rate of complications is difficult as reporting varies from study to study and variable definitions have been used. A recent systematic review30 has confirmed in contemporary cohorts that mortality is generally below 2%. Mechanical circulatory support was required in 2.4%, endotracheal intubation in 4.6% and non-invasive ventilation in 22.5%. Other complications are generally reported per procedure; haemoptysis was reported in 13.5% and lung reperfusion injury (oedema) in 22%.
Our data compare favourably with that from other institutions. We have not observed any serious or life-threatening patient level complications and our rate of acute lung injury (haemoptysis and reperfusion injury) was lower than reported by others. This may reflect our approach, which does not aim at achieving full clearance, but rather targets important disease in basal segmental and subsegmental vessels, minimising the number of small and treacherous vessels treated which likely limits the procedure-related complications.
Future directions
We believe that BPA is now sufficiently developed that appropriately powered randomised controlled trials comparing subsegmental PEA versus BPA and BPA versus PH-targeted therapy can be planned to potentially broaden the indication for BPA in patients with CTEPH. However, consensus in the interpretation of imaging and standardisation of the surgical and BPA approach will be important to deliver meaningful comparisons. The immediate focus of registries should be to guide which endpoints to use and to define what constitutes a ‘good outcome’ for the patients with CTEPH; ideally this will be long-term survival with a good FC and QoL. Further work is also required to explore the nuances of the optimal BPA strategy. Clarity is required to delineate whether focused (as in our series) is superior to extensive and whether serial widespread balloon dilatations of increasing size is better than serial lobar treatments using balloons of appropriate size, as well as understanding the role of adjunctive technologies. Ultimately the issue of cost efficacy needs addressing to determine if lifelong PH-targeted medical therapy remains necessary. It is unclear whether BPA alone will prevent disease progression from the associated vasculopathy, or whether ongoing PH-targeted therapy after haemodynamically successful BPA is still necessary.
Limitations
Oral anticoagulant was briefly interrupted to allow safe BPA therapy to be performed. This may have resulted in further clot formation and disease progression during the perioperative period. Follow-up CPET, 6MWD and echo data were obtained from standard clinical follow-up tests rather than dedicated research studies, and as a consequence, complete datasets were not available in all cases. Hence, some analyses may have been affected by missing variables. Finally, neither patients nor investigators were blinded to the allocated treatment and subjectively reported data interpretation may have been influenced by bias.
Conclusion
Focused BPA targeting basal subsegmental pulmonary arteries is safe and effective in treating inoperable CTEPH with clinically meaningful improvements in haemodynamics, exercise capacity, ventilatory efficiency and RV dimensions that translate into symptomatic benefit and improved QoL for patients.
Acknowledgments
We would like to thank the catheter laboratory, pulmonary vascular disease unit and cardiology ward staff at Royal Papworth Hospital for their support and our patients.
References
Footnotes
Contributors All authors have contributed to this manuscript and have read and agreed to its submission for publication.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as online supplementary information.