Article Text

Abstract
Background People belonging to sexual minority groups have higher levels of suicidality than heterosexuals. However, findings regarding suicide death are sparse. Using unique national data from two countries, we investigated whether individuals entering a same-sex marriage (SSM), a proxy group of sexual minority individuals, had higher suicide rates than those entering opposite-sex marriage (OSM).
Methods A cohort study of all males and females who entered an SSM (n=28 649) or OSM (n=3 918 617) in Denmark and Sweden during 1989–2016 was conducted. Incidence rate ratios (IRRs) for suicide were calculated using adjusted Poisson regression models.
Results In total, 97 suicides occurred among individuals who had entered an SSM compared with 6074 among those who entered an OSM, corresponding to an adjusted IRR of 2.3 (95% CI 1.9 to 2.8). For people who entered SSM, a 46% decline was noted over time from an IRR of 2.8 (95% CI 1.9 to 4.0) during 1989–2002 to 1.5 (95% CI 1.2 to 1.9) during 2003–2016. The excess suicide mortality was present in all age groups but most pronounced among younger individuals aged 18–34 years of age (IRR 2.7, 95% CI 1.5 to 4.8) and females (IRR 2.7, 95% CI 1.8 to 3.9).
Conclusion This large register-based study found higher suicide rates among individuals who entered an SSM, compared with those who entered an OSM. A lower suicide rate was noted for individuals in SSMs in recent years. More research is needed to identify the unique suicide risk and protective factors for sexual minority people.
- suicide
- suicidal behaviour
- sexual minorities
- register data
- Denmark
- Sweden, same-sex marriage
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Studies across several decades and many different countries have found sexual minority individuals, defined as people who identify as lesbian, gay, or bisexual, or engage in same-sex sexual relationships regardless of sexual identity, more frequently report serious suicide ideation and suicide attempts compared with heterosexual individuals.1–4 A recent Swedish study noted elevated rates of suicide attempts among both male and female sexual minority individuals relative to heterosexual persons.5 Still, knowledge of the patterns and causes of suicidal behaviour in sexual minority populations are lacking. Yet, both the WHO and the US National Action Alliance for Suicide Prevention have called for more research to better understand and reduce suicide among sexual minority populations.6 7
Few population-based studies have examined whether sexual minority groups are more likely than heterosexuals to die by suicide and robust analysis is needed.8–10 The few psychological autopsy studies that have attempted to identify the sexual orientation of suicide decedents found no indication of elevated risk, but this conclusion has been challenged, in particular, because of the small number of sexual minority decedents identified through interviews with family members.1
Following the minority stress hypothesis, sexual minority groups are more likely to be exposed to prejudice, stigmatisation, and discrimination, leading to higher levels of distress.11 12 Stressful life-events and feelings of thwarted belongingness have been linked to suicidal behaviour.13
The legal recognition of same-sex marriage (SSM) by Denmark (1989) and Sweden (1995), and the inclusion of data related to SSMs in these countries’ national registers, made possible a population-based approach for examining suicide deaths among individuals who enter an SSM. In recent years, independent studies of the Danish and Swedish registers have reported suicide rates of diverging magnitude among persons who entered an SSM while acknowledging small study population sizes.8–10 14 The small numbers of same-sex married persons and suicides in each country has limited identification of differences in suicide risk with respect to, for instance, age group and period.14–17
To overcome these limitations, this study combined data from the Danish and Swedish registers to determine whether males and females who entered an SSM had higher rates of suicide than those who entered an opposite-sex marriage (OSM). We also examined whether suicide rates varied with respect to country, period under risk, sex, age and current civil status.
Methods
Design
A cohort study design was applied.
Study data and study period
Study data were obtained from national population registers maintained by Denmark and Sweden. The Danish Centralized Civil Register18 and the Swedish Total Population Register contain longitudinal, individual-level data on all persons living in the country, including date of birth and dates of any changes to civil status. Information on causes of death was obtained from the Danish and Swedish Cause of Death Registers. The unique personal identifier that is available in both countries allows individual-level data to be linked across registers.19 20
Data from the two countries were obtained for a period beginning with the date when same-sex unions were first legally recognised, which was in 1989 for Denmark and 1995 for Sweden. For both countries, the study period covers 1 January 1989–31 December 2016.
Study participants and follow-up
Study participants consisted of all individuals in Denmark and Sweden who were 18 years or older and entered marriage during the study period. All participants who entered a new marriage were included as of the date they entered marriage, irrespective of whether their previous marital status was never married, divorced, or widowed. Based on information listed in the civil registers, individuals were placed into one of two studied types of marriage, that is, SSM or OSM.
Using longitudinal data on changes in civil status, the participants current civil status was updated during follow-up with respect to divorce or widowhood as well as subsequent remarriage. We also accounted for participants who switched between types of marriage, that is, SSM or OSM. End of follow-up occurred on: (1) participant’s date of emigration, (2) participant’s date of death, or (3) the end of study on 31 December 2016, whichever happened first.
Outcomes
The primary outcome of interest was suicide as recorded in the Cause of Death Registers in Denmark and Sweden using the following codes from the International Classification of Diseases (ICD): ICD-8: E950-959; ICD-9: E950-959; or ICD-10: X60-X84. It has been suggested that suicide might be under-recorded,21 and Swedish researchers tend to include injuries of undetermined intent (ICD-9: E980-989; ICD-10: Y10-Y34) when studying suicide death.22 This category was implemented in Denmark in 1994 and in Sweden in 1995. The category of ‘undetermined death’ is used more frequently in Sweden than Denmark.23 As a secondary outcome, suicide and deaths by undetermined intent were merged into one measure in order to account for any differences in registration practices between the two countries.
Covariates
The following covariates were examined: country (Denmark, Sweden), period (1989–2002, 2003–2016), sex (males, females), age group (18–34, 35–64, 65+) and current civil status (married, divorced/widowed). The covariates were updated with the accuracy of a month.
Statistical analysis
Incidence rates per 100 000 person-years were calculated based on the number of suicide events and person-months at risk. Poisson regressions were fitted to calculate incidence rate ratios (IRRs) of suicide among males and females who entered SSM versus OSM with 95% CIs. Unadjusted and adjusted regression analyses were carried out in addition to interaction models. We adjusted for country, period, sex, age group and current civil status in the multivariate analyses. There were no missing data.
The statistical analyses were carried out using SAS V.9.4.
Results
Over the entire follow-up, 28 649 (0.7%) individuals entered or re-entered an SSM and 3 918 617 (99.3%) an OSM. In all, 13 442 males (mean age 40.6 years, SD 11.8) and 15 207 females (mean age 36.2 years, SD 9.6) entered or re-entered an SSM while 1 973 388 males (mean age 36.2 years, SD 10.3) and 1 945 229 females (mean age 33.5 years, SD 9.8) entered or re-entered an OSM. Data from Denmark and Sweden were merged prior to analysis, they covered more than 52 million person-years. This included 320 427 person-years for people living in an SSM (0.6%) and 52 244 886 person-years for OSM (99.4%).
In total, 6171 suicide deaths were recorded. Among the 28 649 individuals in an SSM, 97 (0.3%) died by suicide, compared with 6074 (0.2%) of the 3 918 617 individuals in an OSM. The secondary outcome, suicide and undetermined intent, accounted for 7414 deaths; 13% more deaths in Denmark than the outcome restricted to suicides while a 27% difference was noted for Sweden.
Males who entered SSM had a suicide rate of 41.7 (95% CI 34.1 to 49.4) per 100 000 person-years, compared with 16.8 (95% CI 16.8 to 16.9) per 100 000 person-years among those in an OSM. Females who had entered an SSM had a rate of 18.1 (95% CI 12.7 to 23.4) per 100 000 person-years, while those in an OSM had a rate of 6.5 (95% CI 6.4 to 6.5) per 100 000 person-years. The distribution of person-years differed between SSM and OSM with respect to the examined covariates, hence adjusted analyses were called for (table 1). A 2.3-fold (95% CI 1.9 to 2.8) higher rate of suicide was found for people who had entered SSM than for people who had entered OSM when adjusting for differences related to country, calendar years, sex, age and current civil status (online supplementary figure 1). A 2.3-fold (95% CI 1.9 to 2.7) higher rate was also noted with respect to deaths by suicide and undetermined intent.
Supplemental material
Distribution of person-years at risk
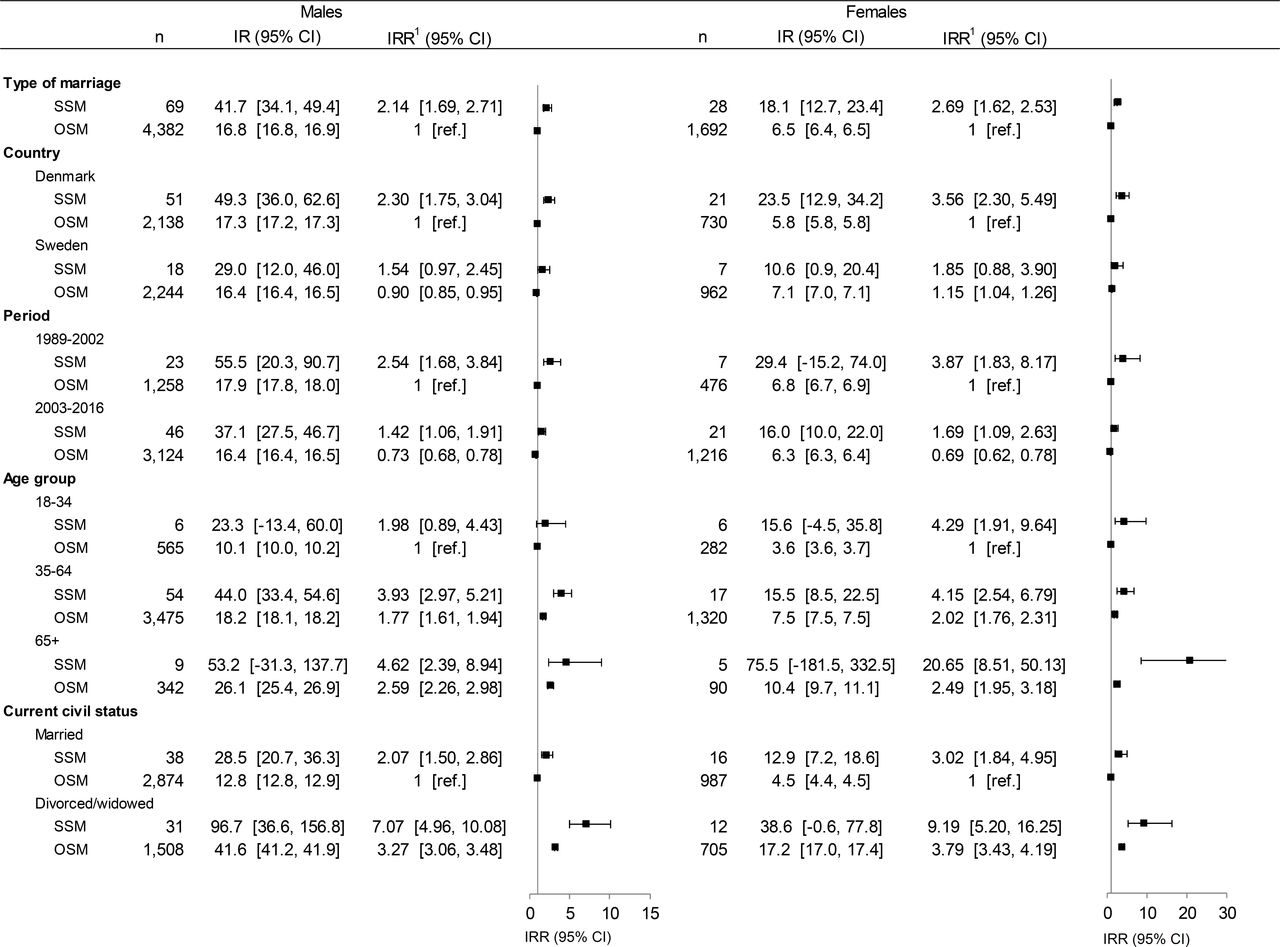
During the follow-up period, the suicide rate ratio of persons entering an SSM was found to be reduced by 46% (figure 1). In the period 1989–2002, the IRR for persons who entered an SSM was 2.78 (95% CI 1.93 to 3.99), compared with 1.50 (95% CI 1.17 to 1.91) in 2003–2016. For persons who had entered OSM, the reduction was 28% from the reference level of 1.0 in 1989–2002 to an IRR of 0.72 (95% CI 0.68 to 0.76) in 2003–2016.

Adjusted IRRs for suicide for males and females. The following covariates were adjusted for: country, period, sex, age group, current civil status. In each interaction model the covariates that were not a part of the main model (presented) were included as adjusting covariates. For instance, when examining for interaction effects between country and type of marriage, the model was adjusted for calendar years, sex, age group and current civil status. IRR, incidence rate ratio.
Among persons who entered SSM, males had a 2.1-fold higher rate than females (males IRR 5.5, 95% CI 4.3 to 7.0 vs females IRR 2.7, 95% CI 1.8 to 3.9). Among people who entered an OSM, a 2.6-fold difference was found between the sexes (males IRR 2.6, 95% CI 2.5 to 2.7 vs females IRR 1.0, ie, the reference category).
Across all age groups, a higher suicide rate was noted among people in SSM than in OSM. Younger adults, aged 18–34 years, who had entered an SSM had an IRR of 2.7 (95% CI 1.5 to 4.8) when compared with those who had entered an OSM (IRR 1.0, ie, the reference category). However, this estimate was based on relatively few observations. For people aged 35–64 years, a 2.2-fold higher rate of suicide was noted among those of SSM when compared with those of OSM (IRR 4.0, 95% CI 3.2 to 5.1 vs IRR 1.8, 95% CI 1.7 to 2.0). For those aged 65 and above, a 2.5-fold higher rate was noted among SSM (IRR 6.6, 95% CI 3.9 to 11.2 vs IRR 2.6, 95% CI 2.3 to 2.9). When assessing people in an SSM, we found that older adults had a higher suicide rate (IRR 2.8, 95% CI 1.3 to 6.1) than young persons (IRR 1.0, ie, the reference category).
With respect to being married, persons who were currently in an SSM had a 2.3-fold higher suicide rate (95% CI 1.8 to 2.9) than those currently in an OSM (IRR 1.0, ie, the reference category). Among individuals who were divorced or widowed, those who had been in an SSM had a 2.2-fold higher suicide rate than those who had been in an OSM (IRR 7.6, 95% CI 5.6 to 10.1 vs IRR 3.4, 95% CI 3.2 to 3.5).
A higher rate of suicide was found for both males and females who lived in an SSM (figure 2); a 2.1-fold (95% CI 1.7 to 2.7) higher rate was found for males and a 2.7-fold higher rate for females (95% CI 1.6 to 2.5). In general, those who were currently divorced or widowed had higher suicide rates than those currently married (SSM, IRR 3.4, 95% CI 2.3 to 5.2; OSM, IRR 3.4, 95% CI 3.2 to 3.6) as seen in online supplementary figure 1. The higher suicide rate among divorced or widowed after SSM was confirmed for both males and females; for males, those currently married had an IRR of 2.1 (95% CI 1.5 to 2.9) while those divorced or widowed had an IRR of 7.1 (95% CI 5.0 to 10.1). The same was observed for females who had entered an SSM (married IRR 3.0, 95% CI 1.8 to 5.0 vs divorced/widowed IRR 9.2, 95% CI 5.2 to 16.3).
{kind=link}
{kind=link}
Adjusted IRRs by type of marriage, country, period, age group and current civil status. The following covariates were adjusted for: country, period, age group, current civil status. In each interaction model the covariates that were not a part of the main model (presented) were included as adjusting covariates. For instance, when examining for interaction effects between country and type of marriage, the model was adjusted for period, age group and current civil status. IR, incidence rate per 100 000 person-years; IRR, incidence rate ratio; OSM, opposite-sex marriage; SSM, same-sex marriage.
Discussion
This is, to the authors’ knowledge, the largest study to date on suicide death among sexual minority individuals, made possible by merging data from the extensive, high quality population registers of Denmark and Sweden. In our adjusted analysis, we found that persons who had ever entered an SSM experienced a suicide rate twice that of those who had entered an OSM. When comparing SSM to OSM, we found particularly elevated rate ratios among younger individuals while the excess suicide mortality has decreased in recent years. We observed independent effects for males and females.
Our findings support previous studies in relation to suicide risks in sexual minorities in Scandinavia8–10 and underline the plausible and harmful role of minority stress.11
Experiences of prejudice and sanctioning—or anxieties of such experiences—might make people with same-sex orientation more vulnerable to suicidal ideation.11 13 These stressors have also been linked to higher levels of psychiatric morbidity among people belonging to sexual minorities, which in turn may affect the risk of suicide.24 25
The rate ratio between persons who entered SSM and OSM was slightly higher for females than for males. While one study8 26 has also shown an independent effect for females, others have not9 10; these differences in reporting are likely related to limitations in statistical power. Although based on a small number of observations, our finding that young adults who entered an SSM experienced the highest excess suicide rate when compared with those in OSM is worrisome. This supports the observation that young adults belonging to sexual minority groups might be particularly vulnerable to social prejudice.27
Previous register-based studies on SSM reported higher rates of those who were divorced or widowed.26 Our more robust findings, based on a larger study population, support the notion that the protective effects of marriage, which have been documented for OSM,17 hold true for those in SSMs as well.
We observed a reduction over time in the suicide rate for persons who entered an SSM. Although suicide rates in the general populations of Denmark and Sweden have been decreasing in recent decades,16 the rate for those living in SSM was declining at a steeper pace, which has not been noted previously. The reasons for this are not entirely clear, but it is possible that persons who entered an SSM in earlier years were different in some respects from those in later marriage cohorts. Prevalence of HIV, coupled with limited treatment options, might have led some, primarily male, couples during 1989–2002 to seek the legal protection regarding inheritance that the status of SSM provided. This is supported by the fact that HIV-virus has been linked to suicide, although these findings are not conclusive.10 28 A second and more plausible explanation could be that, with the passage of time, legalisation of SSM and the expansion of rights and protections to same-sex couples, those minorities have become much more accepted in the Nordic countries and elsewhere. This might have decreased the stigmatisation, psychological stress and level of distress experienced by sexual minority people,29–31 thereby reducing their suicide risk.11 12 Nevertheless, the finding that between 2003 and 2016, people who entered an SSM in the relatively progressive countries of Denmark and Sweden continued to have a suicide rate that was around twice as high as that of people who entered an OSM is worrisome. This points to the critical need for better understanding of suicide risk and protective factors in sexual minority populations.
Strengths and limitations
Nationwide register data were collected on a uniform basis for both persons who entered SSM and OSM, thus, improving the internal validity. All individuals who entered an SSM were identified, avoiding selection and response biases. Longitudinal data allowed us to continuously account for changes in civil status. Furthermore, by including data on people who enter as well as re-enter SSM or OSM, we improved the external validity of the study. Attrition bias was avoided as register data allow for a complete follow-up. The lack of differentials in SSM and OSM suicide rates between Denmark and Sweden, supports the decision to combine the data from the two countries’ registers. The long follow-up period of up to 28 years and nationwide data from two countries were other strengths of the study.
The findings of the current study pertain specifically to people who entered an SSM and may not be representative of all sexual minority individuals in Denmark and Sweden. Among persons who formed a new marriage, 0.7% entered an SSM. In comparison, about 1% of adults in Denmark and Sweden describe themselves as having a minority sexual orientation.4 5 This is comparable to international estimates, although US reports range between 1.0% and 2.5%.32 The study population should thus be considered a subsample of persons in Denmark and Sweden with a same-sex orientation.
The suicide registration is evaluated as reliable in Denmark and Sweden.21 Still, to circumvent the impact of any misclassification of deaths, we included the secondary outcome of deaths by suicide and undetermined intent in our analyses. Furthermore, misclassification is not likely to have been systematically different for participants entering SSM and OSM. A limitation of the study is that the nature of the data did not allow many factors to be considered that may have helped to explain findings about suicide rates, for example, stigma and discrimination, individual coping strategies, and social support. Although it would have been preferred, it was not feasible to include data on socioeconomic status or mental health as these were not available to both research teams.
Clinical implications
People belonging to sexual minority groups sometimes anticipate negative sanctioning from clinicians,33 making it important to promote positive encounters with healthcare providers. While more research is needed to better understand the underlying factors for suicide risk in SSM people, clinicians should be familiar with best practice guidelines for treating sexual minority people.34 35
In sum, people who entered SSM were found to have a markedly higher rate of suicide than people who entered OSM in adjusted analysis. Although not representative for all sexual minority individuals and despite an improvement over time, elevated rates were noted, in particular among females and younger individuals.
What is already known on this subject
Excess suicide risks have been found for males and females living in same-sex marriages (SSMs), yet, little is known with respect to whether rates differ with respect to age group, period and current civil status. Furthermore, methodological shortcomings due to difficulties in sampling representative study groups have restrained researchers from drawing conclusions.
What this study adds
This population-based study found a robust estimate of a 2.3-fold higher rate of suicide among people living in SSMs in Denmark and Sweden during 1989–2016. Interestingly, a lower excess suicide rate was noted in recent years. The excess suicide risk across sociodemographic characteristics has not previously been demonstrated for females who entered an SSM. Our findings emphasise that awareness and understanding of needs for support towards these groups are called for.
References
Footnotes
Contributors All authors were actively involved in planning the study and engaged in discussing ongoing progress of analyses and interpretation of findings. AE, SD and GA were in charge of the data management and analyses with feedback from AH, MN and CB. AE drafted and revised the manuscript based on comments provided by all authors. All authors approved the final version of the report. AE and GA are the final guarantors of the study.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The research project was approved by the Danish and Swedish Data Protection Agencies.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available.