Article Text

Abstract
Hypertension is a global public health issue and a major cause of morbidity and mortality. Its prevalence is increasing in many Asian countries, with a number of countries with blood pressure above the global average. Although the average systolic blood pressure is decreasing worldwide since the 1980s at the rate of about 1 mm Hg systolic blood pressure per decade, it is increasing in low-income and middle-income countries, especially in the East and South Asian population. Of note, the much larger base Asian population results in a considerably larger absolute number of individuals affected. When compared with Western countries, hypertension among Asian populations has unique features in terms of its onset, clustering of associated cardiovascular risk factors, complications and outcomes. Moreover, only a minority of hypertensive individuals are receiving treatment and achieving control. Projected number of deaths related to hypertension dramatically increased in the last 25 years in some Asian regions with a disproportionately high mortality and morbidity from stroke compared with Western countries. The relation between blood pressure and the risk of stroke is stronger in Asia than in Western regions. Although new Guidelines for hypertension diagnosis and management have been recently released from Europe and North America, the unique features of Asian hypertensive patients raise concerns on the clinical applicability of Western Guidelines to Asian populations. To this purpose, we critically reviewed key elements from the most updated Guidelines. We also discussed their core concepts to verify the impact on hypertension prevention and management in Asian countries.
- hypertension
- EBM
- quality of care and outcomes
- Guidelines
- Prevention
- Blood pressure
Statistics from Altmetric.com
Introduction
Hypertension is a common risk factor for cardiovascular (CV) disease and a serious global health issue, remaining the most powerful predictor of mortality in high-income and low-income countries.1 Results from the Global Burden of Disease, Injuries, and Risk Factor study documented that systolic blood pressure (BP) was associated with the highest burden among risk factors, more than either smoking or obesity.1 The projected number of individuals with systolic BP of 140 mm Hg or higher increased from 442 million (95% uncertainty interval (UI) 437 to 447 million) in 1990 to 874 million (95% UI 864 to 884 million) in 2015, and the associated annual number of projected deaths in 2015 (7.8 million, 95% UI 7.0 to 8.7 million) or 14.0% of total deaths (95% UI 12.5% to 15.5%) and 143 million disability-adjusted life years (95% UI 130.2 to 157.0 million) were related to systolic BP of 140 mm Hg or higher.1
Asia is the world’s most populous region and its rapid economic and population growth has brought un-presented burden of chronic disease (including hypertension) and demand for health services to all countries, in particular China and India.2
Furthermore, although the average systolic BP is decreasing worldwide since the 1980s at the rate of 1 mm Hg systolic BP per decade, it is increasing in low-income and middle-income countries, especially in the South Asian population.2 3 Thus, prevalence of hypertension is increasing in many countries of this region and the much larger base Asian population results in a considerably larger absolute number of individuals affected.4
A systematic review of 33 studies from Member Countries of South Asian Association for Regional Cooperation5 showed that the overall prevalence of hypertension was around 27%. Hypertension varied between the studies, ranging between 13.6% and 47.9%, and was found to be higher in subjects of urban than in rural areas. Prevalence of hypertension from the latest studies5 was Bangladesh, 17.9%; Bhutan, 23.9%; India, 31.4%; Maldives, 31.5%; Mongolia, 47%; Nepal, 33.8%; Pakistan, 25%; Republic of Korea, 30%; and Sri Lanka, 20.9%.2 5
More recently, data from the Patient-Centred Evaluative Assessment of Cardiac Events (PEACE) Million Persons Project (MPP),6 enrolling 1.7 million adults aged 35–75 years from across China, estimated an age-standardised and sex-standardised prevalence of hypertension (defined as either BP >140/90 mm Hg or self-reported use of antihypertensive medication in the previous 2 weeks) equal to 37.2% (95% confidence interval [CI] 37.1 to 37.3).
More importantly, only 22.9% (95% CI 22.7 to 23.0) of these patients were receiving treatment, and only 5.7% (95% CI 5.6 to 5.7) were achieving BP control.
In this context, it is worthy to be mentioned that use of medications to prevent and treat CV disease remains considerably low in Asia7 and most people for whom BP-lowering drugs are clearly indicated receive no treatment whatsoever.2 8
Data from the PEACE MPP study and from a nationwide sample of 3362 primary care facilities9 showed that 8.1% of facilities (95% CI 7.2 to 9.1) did not stock any hypertensive drugs, and only 33.8% (95% CI 32.2 to 35.4) stocked all four standard classes of antihypertensive drug classes. Thus, deficiencies in Asian health system make a large contribution to the disease burden.10
Finally, the phenotypes of CV disease, stroke and heart failure, which are closely associated with BP, are more common in Asia.11 Moreover, the association between hypertension and CV disease is stronger in Asian countries than Western countries11 and deaths associated with systolic BP of 140 mm Hg or higher significantly increased in the last two decades in Asian regions (East Asia, +151.9%; Southeast Asia, +101.0%; Central Asia, +37.7%; South Asia, +130.8%).1
Epidemiology of hypertension revised
New Guidelines for the diagnosis and management of hypertension have been recently released from Europe12 and North America.13
In the recently released 2018 European Society of Cardiology/European Society of Hypertension (ESC/ESH) Guidelines,12 definition of hypertension remained unchanged (office BP ≥140/90 mm Hg) when compared with the previous one (table 1).
Blood pressure categories according to the 2017 American College of Cardiology/American Heart Association (ACC/AHA) and 2018 European Society of Cardiology/European Society of Hypertension (ESC/ESH) Guidelines12 13
Conversely, the 2017 American College of Cardiology/American Heart Association (ACC/AHA) Guidelines for the Prevention, Detection, Evaluation, and Management of High BP in Adults13 lowered the systolic and diastolic BP thresholds for diagnosis of hypertension (table 1) to 130/80 mm Hg, a shift that inevitably leads to define more subjects as hypertensive. For example, a cross-sectional analysis from the population-based 2016 Nepal Demographic and Health Survey14 documented that when the new definition of hypertension by the ACC/AHA Guidelines13 is being adopted, the overall prevalence of hypertension in Nepal would approximately double and the number of individuals requiring pharmacotherapy would increase. Briefly, among 13 519 participants recruited, 44.2% had hypertension according to the 2017 ACC/AHA Guidelines compared with 21.2% by the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure Guidelines.14 When estimating the proportion of hypertension by background characteristics, the new 2017 ACC/AHA Guidelines definition increased the prevalence to 50% or greater for some categories, with the highest prevalence among those with a body mass index greater than or equal to 30 and between 25 and 29.9 kg/m2.
Similarly, Khera and coworkers estimated the relative increase of prevalence among adults aged 45 to 75 years in China and found an overall relative increase of 26.8% in this country15 (figure 1).
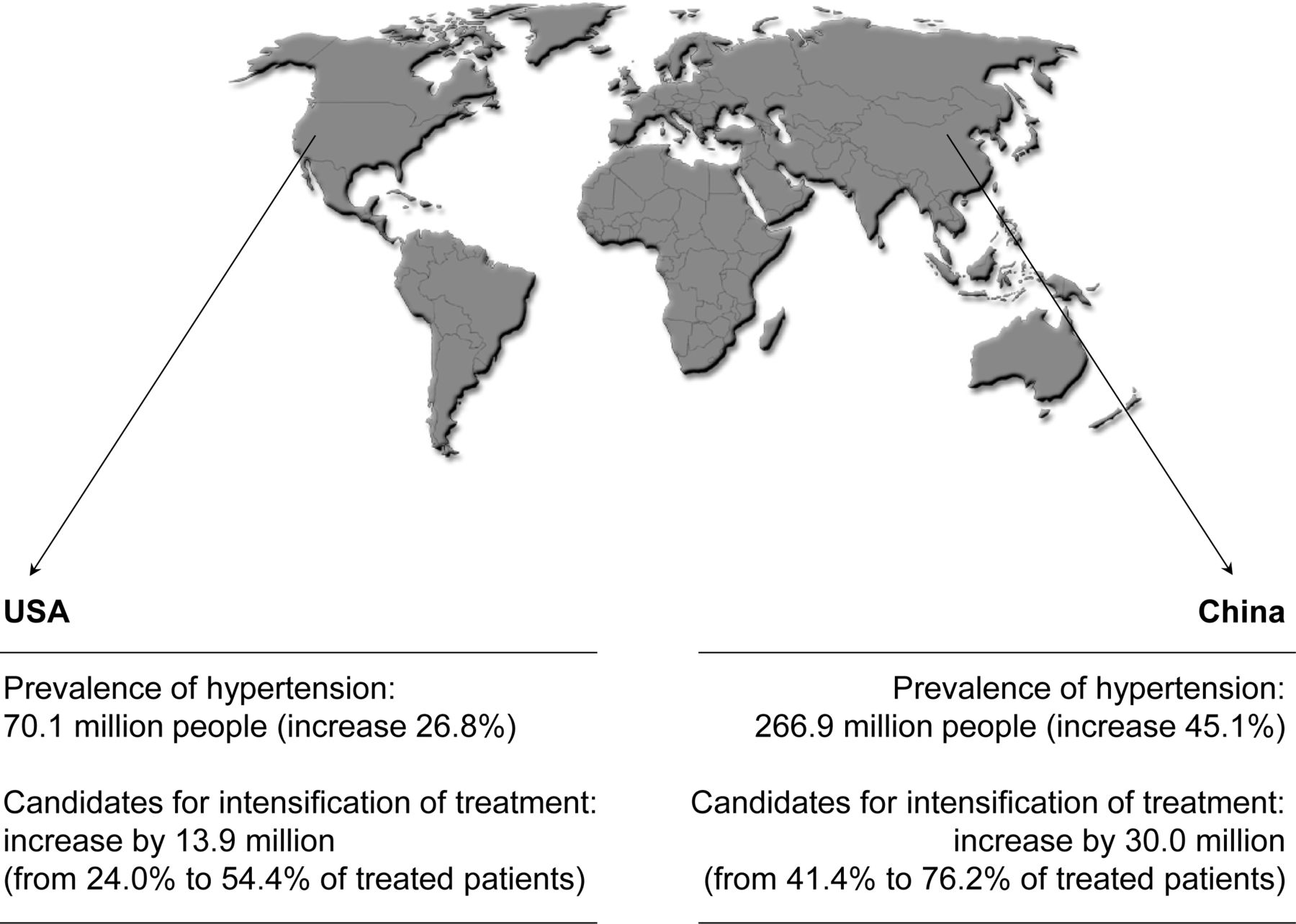
Effects of the 2017 American College of Cardiology/American Heart Association hypertension guidelines on the prevalence of hypertension and eligibility for initiation and intensification of treatment in nationally representative populations from the USA and China. Data from Khera et al.15
It has been also reported that CV events were often diagnosed at lower BP levels than the 140/90 mm Hg cut-off points in some Asian regions, questioning whether appropriate (and lower) limit values of BP to define hypertension should be used, especially for developing country populations.16
Of note, epidemiological studies on hypertension in western Indian urban and rural cohorts17 showed that distributions of BP are different in various age groups; for example, in men aged 20–29 years, a systolic BP of 140 mm Hg is not reached until the 95th percentile while at 60–69 years it is achieved at the 70th percentile.17 Similar variations are seen in diastolic BP.17 In other words, either percentile values for diagnosis of hypertension should be different at various age groups or the systolic/diastolic BP for the diagnosis of hypertension should be lower in younger subjects.
Impact of ‘SPRINT ’
The 2017 ACC/AHA Guidelines for the Prevention, Detection, Evaluation, and Management of High BP in Adults13 recommend a systolic BP target <130 mm Hg in almost all hypertensive patients. They fully endorse the evidence of benefit for a lower systolic BP target than that currently recommended, as documented in the Systolic Blood Pressure Intervention Trial (SPRINT).18
Briefly, the SPRINT trial included 9361 participants with a systolic BP of 130 mm Hg or higher and an increased CV risk randomly assigned to a systolic BP target of <120 mm Hg (intensive treatment) or a target of <140 mm Hg (standard treatment).
Findings indicated that patients in the intensive treatment group had a 25% risk reduction in the primary composite end point of major CV events (eg, myocardial infarction, non–myocardial infarction acute coronary syndrome, stroke, acute decompensated heart failure and CV disease death) and a 27% risk reduction in mortality compared with those who received standard treatment.18
Of note, the SPRINT trial18 used programmable automated oscillometric devices to measure BP. Nonetheless, there is confusion in recent publications regarding whether the BP measurements at SPRINT clinics were unattended.19 Concern has also been expressed that the BP readings obtained in SPRINT were not comparable with BP readings in other trials where the measurement was attended and that the intensive treatment goal of <120 mm Hg in SPRINT would actually correspond to higher systolic BP values in other trials.19 20
As pointed out by a recent report by Johnson and coworkers,20 there were 4082 participants at 38 sites that measured BP after leaving the participant alone the entire time (always alone), 2247 at 25 sites that had personnel in the room the entire time (never alone), 1746 at 19 sites that left the participant alone only during the rest period (alone for rest) and 570 at 6 sites that left the participant alone only during the BP readings (alone for BP measurement). Importantly, similar BP levels and CV disease risk reduction were observed in the intensive group in SPRINT participants whether the measurement technique used was primarily attended or unattended.
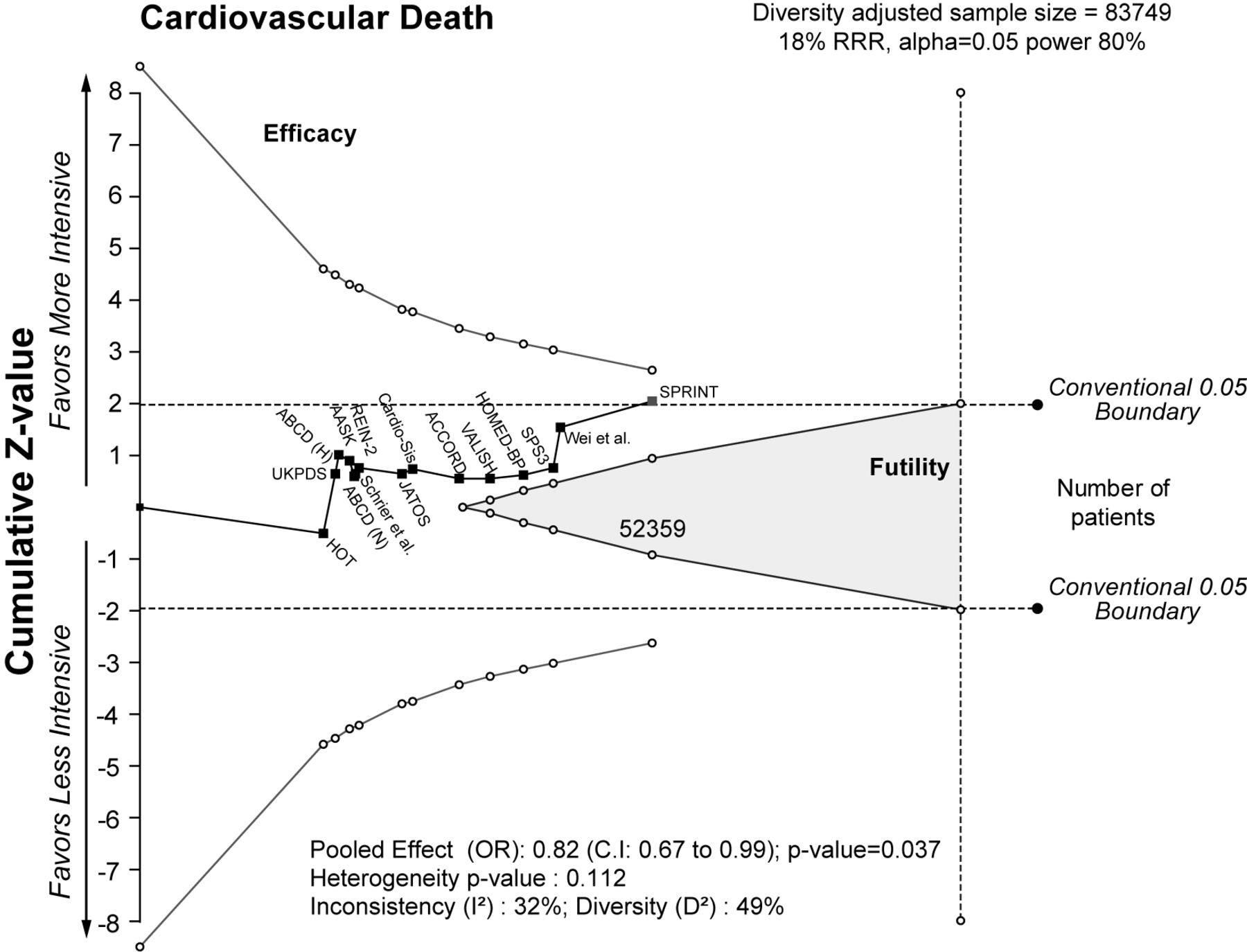
Although the available evidence clearly supports the notion that even a small decrease in BP reduces risks of CV morbidity and mortality21 (figure 2) and that an intensive BP-lowering strategy significantly reduces the risk of CV mortality without evidence of harm (figure 3),22 the ESC/ESH Guidelines stated that BP should be lowered to levels <140/90 mm Hg in all patients (I A recommendation) and to ≤130/80 mm Hg ‘in most patients’ provided that the treatment is ‘well tolerated’ (I A recommendation).12 Nevertheless, the European Guidelines12 recommend that systolic BP should be lowered (1) to <140 mm Hg, but not to <130 mm Hg, in patients aged ≥65 years and (2) <130 mm Hg, but not below 120 mm Hg in younger patients (<65 years; I A recommendation).12 Similarly, 2018 ESC/ESH European Guidelines12 recommend to lower systolic BP to a range 130 to <140 mm Hg in patients with diabetic or non-diabetic chronic kidney disease.23
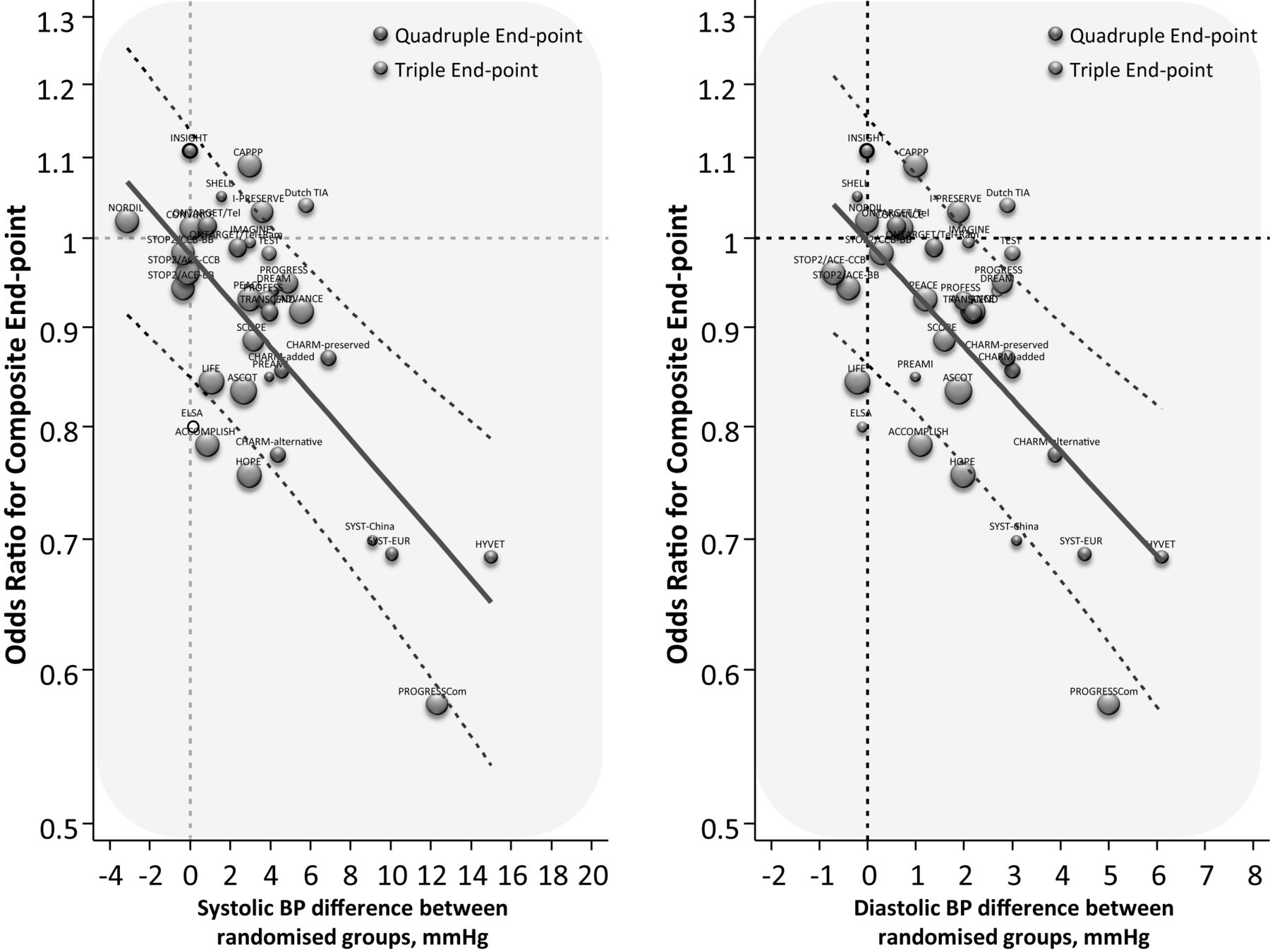
Relationship between the reduction in blood pressure (BP) and the risk of composite cardiovascular endpoints (triple: myocardial infarction, stroke and cardiovascular death; quadruple: myocardial infarction, stroke, cardiovascular death and congestive heart failure). Thirty trials are included for a total of 221 024 patients. For each trial, the difference in BP between randomised groups is depicted. Data from Verdecchia et al 21 (with permission). BP, blood pressure.

{kind=link}
{kind=link}
{kind=link}
Trial sequential analysis (TSA) of the effect of more intensive vs less intensive blood pressure reduction on cardiovascular mortality. See Verdecchia et al 22 for guidance on TSA and plot interpretation (with permission). RRR, relative risk reduction; OR, odds ratio; CI, confidence interval.
In other words, the European Guidelines12 support the clinical use of ‘safety boundaries’, not to be crossed towards lower BP levels even in patients with a perfect tolerability of treatment.
Safety boundaries in the Asian context
Lowering the threshold for diagnosis of hypertension, as recommended by the ACC/AHA Guidelines, may be considered a valuable achievement in the light of evidence that a higher BP is associated with adverse CV outcomes even at levels below 140/90 mm Hg13.
An analysis of an ongoing cluster-randomised community-based screening trial from India demonstrated that BP was associated with CV mortality at thresholds lower than the ESC/ESH hypertension definition.16 Specifically, 167 331 adults aged 35–90 years were included in the analysis. Death rates were calculated according to systolic and diastolic BP, and their associations were examined in multivariable analyses. The nadir of CV death rates was observed at 110 mm Hg for casual systolic BP and 75–80 mm Hg for casual diastolic BP. In the multivariable analyses, systolic BP from 120 mm Hg and diastolic BP from 90 mm Hg were significantly associated with risks of ischaemic heart disease and stroke.
Furthermore, in the Mumbai Cohort Study, pre-stage hypertension (systolic BP 130–139 and/or diastolic BP 85–89 mm Hg) was associated to an increased risk of cerebrovascular death in men (hazard ratio [HR] 1.73, 95% CI 1.15 to 2.61) when compared with normal BP (systolic BP <120 and diastolic BP <80 mm Hg).24
More recently, a prospective study of 5752 subjects free of CV disease (Chinese Multi-provincial Cohort Study)25 evaluated to what extent the new BP stratum of stage 1 hypertension (systolic/diastolic BP of 130 to 139/80 to 89 mm Hg) affects the CV risk. The participants with baseline systolic/diastolic BP <130/80 mm Hg, 130–139/80–89 mm Hg and ≥140/90 mm Hg were 2892 (50.3%), 1328 (23.1%) and 1532 (26.6%), respectively. After adjustment for several confounders (including age, sex, body mass index, smoking status, diabetes, total cholesterol and high-density lipoprotein cholesterol at baseline), participants who maintained a systolic/diastolic BP at 130–139/80–89 mm Hg during follow-up had a higher risk of developing acute CV events, coronary heart disease and stroke with the HRs of 2.04 (95% CI 1.16 to 3.57), 3.29 (95% CI 1.30 to 8.35) and 1.63 (95% CI 0.80 to 3.33), compared with those who maintained their systolic BP <130 mm Hg and diastolic BP <80 mm Hg. Participants whose BP increased from 130–139/80–89 mm Hg to hypertension over the follow-up period had 2.81-fold (95% CI 1.84 to 4.29), 3.17-fold (95% CI 1.43 to 7.03) and 2.71-fold (95% CI 1.65 to 4.44) higher risk for the incidence of acute CV events, coronary heart disease and stroke, respectively, compared with participants who maintained their systolic BP <130 mm Hg and diastolic BP <80 mm Hg.
Overall, the BP targets recommended by the ACC/AHA Guidelines13 considerably differ from the indications released by the ESC/ESH Guidelines.12
Furthermore, the use of ‘safety boundaries’, as suggested by the European Guidelines,12 raises important concerns in the treatment of hypertension in Asian populations.
A first consideration regards the management of elderly subjects. With a rapidly ageing population, the prevalence of hypertension in Asia continues to rise, and older adults account for the bulk of hypertension-related morbidity and mortality.2 4 In many Asian countries, hypertension is very common in the elderly. For example, the prevalence of hypertension in China is 39% overall, 59.4% in patients aged ≥60 years and 72.8% in those aged ≥75 years.26 Although none of the available Asian intervention trials provided strong support for more ambitious BP targets in elderly patients with hypertension,2 a recent meta-analysis by Yano and coworkers27 showed a benefit in terms of CV and stroke prevention when a BP target of less than 140/80 mm Hg is achieved in Asian hypertensive patients. More specifically, in the subgroup analysis of elderly patients, stroke risk was decreased by intervention in trials comparing an active treatment with a placebo, or a more intensive with less intensive BP control (odds ratio [OR] 0.74, 95% CI 0.58 to 0.93).27
In this context, Asian physicians need to consider specific features of their hypertensive patients4 regarding the association between elevated BP and the risk of CV disease.2 28 The Asia Pacific Cohort Studies Collaboration, which involved >500 000 individuals followed for several years, has demonstrated28 that the association of BP with the risk of stroke was about twice as steep as that with coronary heart disease risk. While the association with coronary risk was similar in the Asian and Caucasian populations, the association with stroke risk was steeper among Asians.2 8 29 Moreover, in the aforementioned meta-analysis by Yano and coworkers,27 a 10 mm Hg reduction in systolic BP was associated with a 30% reduced risk for stroke.27
Taken together, these findings suggest that the clinical use of ‘safety boundaries’ (ie, treated systolic BP not below 130 mm Hg in subjects aged 65 years or more, and not below 120 mm Hg in subjects aged less than 65 years), as recommended by the European Guidelines,12 might be counterproductive in Asia. Implementation of ‘safety boundaries’ could induce doctors to refrain from achieving lower BP targets that, if well tolerated, would reasonably result in a lesser risk of stroke, so frequent in Asia, and other major complications of hypertension.
Conclusions
The high prevalence of hypertension in Asia notably contributes to the growing worldwide burden of CV disease and death.2 The Asia Pacific Cohort Studies Collaboration clearly showed a progressive reduction in the risk of stroke, ischaemic heart disease and CV death up to BP values of about 115/75 mm Hg.28 Notably, such relation held in both genders, and a 10 mm Hg lower systolic BP was associated with a 41% lower risk of stroke.28 Similar results were also obtained from the aforementioned Trivandrum community-based study16 and Mumbai Cohort Study.24
Being stroke a dominant complication of hypertension in Asia, the substantial benefit of an intensive BP reduction on the risk of stroke should be considered in future Guidelines on the management of hypertension in Asian populations.
In general, adaptation of western Hypertension Guidelines to the Asian context is not automatic. The use of relatively low diagnostic thresholds and therapeutic targets (130/80 mm Hg), as suggested by the ACC/AHA Guidelines,13 appears acceptable in an Asian context. Conversely, the message of European Guidelines12 should be probably applied with more caution. The European recommendation12 that systolic BP should not be lowered <130 mm Hg in patients aged ≥65 years and <120 mm Hg in patients aged <65 years is not supported by at least three well-conducted systematic reviews and meta-analyses. In a meta-regression analysis by Ettehad and coworkers, a greater reduction in systolic BP was associated with a greater risk reduction without any evidence of a J-curve effect.30 In a network meta-analysis by Bundy and coworkers, a mean achieved systolic BP 120–124 mm Hg was associated with a significant reduction in the risk of cardiovascular disease and all-cause mortality even in the comparison with achieved systolic BP levels 125–129 mm Hg.31 Bangalore and coworkers published a network meta-analysis of trials designed to compare different BP targets and concluded that systolic BP targets <120 mm Hg and <130 mm Hg ranked number 1 and number 2, respectively, as the most efficacious for preventing stroke and myocardial infarction.32 Conversely, systolic BP targets <140 mm Hg and <150 mm Hg ranked as number 1 and number 2, respectively, for safety. Overall, a systolic BP target <130 mm Hg achieved the best balance between efficacy and safety.32
In summary, the use of 130/80 mm Hg as a diagnostic threshold and management goal of BP may contribute to more sustained target organ protection and CV disease prevention. Instead of fixing rigid BP targets or safety boundaries, what we should pursue in the daily practice is an optimal balance between the magnitude of achieved BP reduction and the tolerability of treatment in the single patient.33 34 An aphorism might be: ‘The lowest well-tolerated blood pressure, the better’. This conclusion seems to particularly applicable to Asia, where the achievement of normal or optimal BP levels for prevention of stroke remains a priority in the treatment of hypertension.
Acknowledgments
Supported in part by the non-profit foundation ‘Fondazione Umbra Cuore e Ipertensione-ONLUS’, Perugia, Italy.
References
Footnotes
Contributors All authors have read and approved the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.