Article Text

Abstract
Background Hip and knee total joint arthroplasty (TJA) procedures are two of the most common inpatient surgical procedures worldwide. Outpatient TJA has emerged as a feasible option. COVID-19 caused significant constraints on inpatient surgical resources and contributed to a growing surgical backlog. We present a quality improvement (QI) initiative aimed at adding an outpatient TJA pathway to our pre-existing inpatient TJA programme, with the target of performing 25% of our primary TJA as outpatients.
Methods This was a QI study at a tertiary level arthroplasty centre. To achieve our aim, a patient-centred needs analysis revealed the need to develop patient selection criteria, perform a specific and tailored anaesthetic, provide patient education and conduct virtual care follow-up. Based on these findings, an outpatient TJA intervention bundle was developed and implemented.
Results After implementing the outpatient pathway, 65 patients were scheduled for outpatient TJA. Fifty-five (84.6%) patients were successfully discharged home on the day of surgery. Successful outpatient TJA accounted for 33.3% of all primary TJAs performed at our intuition throughout the study period. There was excellent adherence to the intervention protocols, with the success hinging on multidisciplinary team and supported QI culture. Thirty-day emergency department visits for inpatient and outpatient TJAs were 8.93% and 6.15%, respectively. No outpatient TJA patients required hospital readmission within 30 days.
Conclusion Our study demonstrates that implementation of an outpatient TJA pathway in response to inpatient resource constraints during the COVID-19 pandemic is feasible. The findings of this report will be of interest to surgical centres facing surgical backlog and constraints on inpatient resources during and after the pandemic.
- ambulatory care
- healthcare quality improvement
- COVID-19
- teamwork
- transitions in care
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Hip and knee total joint arthroplasty (TJA) are established procedures for end-stage hip and knee osteoarthritis (OA) and are among the most common inpatient surgeries performed in the USA. Over 1 million TJAs are performed in the USA annually.1 2 In recent years, the length of stay (LOS) for TJA patients has dramatically decreased such that some patients are discharged home within hours of their procedure.3 Much of this reduction in LOS stems from advancements in surgical and perioperative care, including novel strategies for multimodal analgesia and the goal of hospitals to reduce inpatient care costs.4 The benefits of outpatient TJA are well aligned with the Institute of Health Improvement’s triple aim, as it is associated with reduced costs and high rates of patient satisfaction.3 5–8
Despite the benefits and ongoing uptake of outpatient TJA, the majority of TJA procedures are still performed as inpatient, which has presented significant challenges for many TJA centres across the world throughout the COVID-19 pandemic. Surgical resources such as inpatient beds and ward nurses have been diverted towards care of patients with COVID-19, subsequently leading to cancellation or rescheduling of many TJA procedures.9 Furthermore, directives from governing bodies to cease all elective surgical procedures during peak waves of the pandemic have further contributed to surgical backlogs, which are estimated to take years to overcome.10 The impact of delaying TJA for end-stage OA patients has been substantial, with one scoping review highlighting the physical, psychological and financial implications to patients and concluding that the COVID-19 pandemic emphasises the need for outpatient TJA.11
While outpatient TJA is feasible for a subset of patients, successful implementation requires a patient-centred approach including explicit patient selection criteria, managing patient expectations and concerns, providing education on pain management, mobility and physiotherapy exercises and availability of outpatient care and follow-up.4 7 8 12–15
At our tertiary healthcare centre, 600 primary TJA procedures are performed annually. Using enhanced recovery after surgery protocols and quality improvement (QI) methodologies which are embraced and supported within our institution, we previously reduced inpatient LOS to under 2 days.16 However, our programme has traditionally relied on an inpatient model and had no existing pathway or resources for outpatient surgery, with no TJA surgeries being performed as outpatient prior to the pandemic. During the first wave of the pandemic, suspension of all elective procedures such as TJA due to advanced provincial directives resulted in an extensive local surgical backlog.10 A subsequent provincial report published in June 2020 by Ontario Health emphasised that transitioning traditionally short-stay surgeries to outpatient would be needed to offload inpatient resources for COVID-19 inpatients and other surgical patients.17 At our institution, we recognised the challenge of continuing to deliver elective TJA to patients throughout the pandemic, where they might not be prioritised in the same fashion as oncology cases. With this context in mind as well as Ontario Health recommendation, we promptly pivoted to meet the needs of our population by delivering outpatient TJA within a system set up for inpatient care.
The purpose of this QI project was to add an outpatient TJA pathway to our pre-existing inpatient TJA programme. Specifically, our aim was to successfully perform 25% or more of local primary TJA as outpatient surgeries by 30 June 2021.
Methods
A multidisciplinary project team was formed that comprised of surgical services leadership, surgeons, anaesthesiologists, physiotherapists, nurses, a pharmacist, an information technologist and a social worker. This project was designed as a prospective QI study. This QI project report follows the Standards for Quality Improvement Reporting Excellence (SQUIRE) 2.0 publication guidelines for QI reporting.18
Each team member took the lead in their area of expertise, with a senior director organising meetings and following up on assigned tasks. Meetings were scheduled weekly for the first 3 months and monthly thereafter. These meeting were used to examine data collected, learn from successes and discharge failures and identify areas for improvement for the next iterative improvement cycles, using plan–do–study–act (PDSA) cycles.
As a first step, a qualitative needs analysis was performed by reviewing available local resources, surveying practices of a nearby ambulatory surgical centre and conducting a review of all pertinent literature.3 19–25 Pilot cases were performed over a 3-month period to help identify barriers for successful outpatient TJA.
Patient involvement
A random sample of four patients from the pilot ambulatory group was interviewed to review the patient education material for content and clarity, to obtain feedback on their experience and to identify areas of improvement with respect to education, perioperative management and postoperative care. Their satisfaction was then assessed using a simple binary question posed at the end of the interview: ‘Are you overall satisfied with the ambulatory programme’. Patients were not compensated for their participation.
Interventions
Our pre-existing inpatient TJA pathway has previously been described and includes a multimodal analgesia protocol and patient education materials.16 The multidisciplinary group decided to complete a needs assessment and pilot cases to identify barriers to the programme. Inclusion and exclusion criteria agreed on by the anaesthesiology and surgical teams can be found in online supplemental appendix A. The agreed-on perioperative anaesthetic care plan can be found in online supplemental appendix B.
Supplemental material
Supplemental material
Measures
The primary outcome measure was defined as the number of successful TJA outpatient procedures performed as a percentage of all TJAs performed. Process measures were intended to capture adherence to our new outpatient pathway interventions and included the following:
Preoperative
Use and adherence to the preoperative patient selection criteria.
Completion of perioperative analgesia education by the acute pain service (APS).
Intraoperative
Type and dose of spinal anaesthetic medication.
Nerve blocks provided.
Postoperative
Completion of postanaesthetic care unit (PACU) physiotherapy assessment prior to discharge.
Virtual postoperative surveillance and follow-up 24 and 48 hours post discharge.
Balance measures included any associated patient safety events in the PACU or at home such as falls, hypotension, vasovagal episodes, urinary retention, uncontrolled nausea, uncontrolled pain preventing discharge or advice to return to hospital based on issues identified in the follow-up phone call. Thirty-day postoperative emergency department (ED) visits and hospital readmissions were captured as well.
Statistical analysis
Descriptive statistics were used to summarise the number of successful TJA outpatient procedures performed as a percentage of all TJAs performed during the period of interest as well as patient characteristics for inpatient and outpatient TJA groups. A logistic regression explored clinical and procedure-related predictors for unsuccessful discharge home from PACU (eg, procedure type, scheduled time of day) with a p value>0.05 considered significant (table 1).
Predictors for unsuccessful discharge home from PACU
Results
Lessons from pilot cases
PDSA cycle analysis started with the pilot cases (online supplemental appendix C). All four patients interviewed during the pilot phase for feedback reported overall satisfaction with the programme. Suggestion on improving clarity and content of the educational material and process changes in terms of education and follow-up on pain management strategies were incorporated into the programme. Drivers for the outpatient pathway and new change ideas for the outpatient patients were developed based on a needs analysis and pilot cases and are illustrated in figure 1.
Supplemental material

Driver diagram illustrating the outpatient TJA pathway. Created by authors.
Pilot outpatient cases and process flow mapping revealed the barriers for early patient mobilisation. These included access to a PACU physiotherapy assessment and the duration of the spinal anaesthetic as many patients were not ready to mobilise during daytime physiotherapy shifts due to residual spinal motor block. Moreover, a philosophy of the ‘well patient’ model needed to be adopted throughout the spectrum of care of these patients; this included preparing them early for mobilisation, dressing them soon after the spinal motor block receded, ensuring they would tolerate oral intake and medications and focusing on return of function early in the postoperative period.24 Patients’ input highlighted the need for more robust education regarding home analgesia medications and mobilisation exercises. Lastly, our inpatient model did not have any formal virtual patient assessment once they were discharged home (figure 1).
Intervention implementation
Implementation of the project was achieved via education rounds, team meetings and continuous engagement with stakeholders and patients. Patients who met the selection criteria and were agreeable to undergo TJA in the outpatient setting were scheduled from 1 January to 30 June 2021. Unfortunately, elective arthroplasty procedures were suspended because of an advanced provincial directive suspending all non-urgent surgeries in April–May 2021 due to a severe third wave of COVID-19 in Ontario.
Patient characteristics
From January to June 2021, 165 patients were scheduled for primary TJA. Sixty-five (39%) of these patients met the selection criteria and were scheduled for the outpatient TJA pathway. There were no differences between in the inpatient and planned outpatient TJA groups with respect to age or sex. An American Society of Anesthesia (ASA) classification of 3 or higher was in 78.53% of inpatients and 47.27% of outpatients. This was in keeping with our preoperative patient selection criteria which excluded ‘high risk’ medically complex patients for the outpatient pathway.
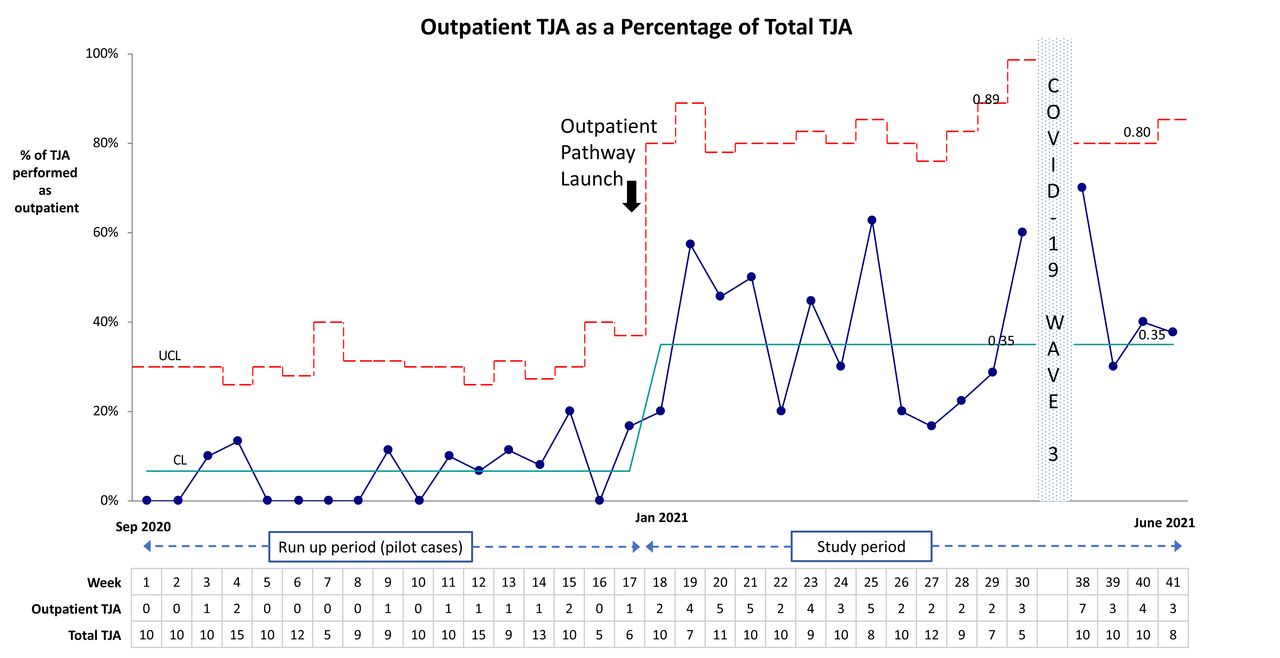
Of the 65 patients scheduled for outpatient TJA, 55 (84.6%) achieved successful discharge home from the PACU. Successful outpatient TJA accounted for 33.3% of all primary TJAs performed at our intuition throughout the project period (figure 2).
{kind=link}
{kind=link}
A statistical process control P chart showing successful outpatient TJA as a percentage of all TJAs performed. All elective procedures were suspended during weeks 31–37 due to the third wave of COVID-19 in Ontario. Created by authors. TJA, total joint arthroplasty. UCL (upper control limit); CL (control limit)
Review of process measures indicated that there was overall excellent adherence to the interventions. There were no outpatient TJA candidates with ‘high risk’ conditions as per the patient selection criteria (online supplemental appendix A). The APS consulted on 97% of patients for analgesia education. Overall, 98% of patients received the short-acting spinal anaesthetic (details described in online supplemental appendix B), the exception being a single patient who inadvertently received long-acting spinal morphine (commonly used in the inpatient pathway), necessitating an unplanned hospital admission. All patients received the recommended nerve blocks. Physiotherapy team (PT) assessed 97% of patients within 3 hours of arrival in the PACU to ensure safe mobility. Of the patients who were successfully discharged home from the PACU, 81% and 60% received telephone follow-up assessments on postoperative days 1 and 2, respectively. All patients were called a minimum of two times, but they did not always answer the phone, causing the disparity in follow-up phone calls.
There were 10 cases of unsuccessful discharge home from PACU. Causes were pain in 4/10, hypotension in 3/10, hypoxia 2/10 and long duration spinal from inappropriate spinal medication in 1/10. Predictors for unsuccessful discharge home from PACU included type of procedure and scheduled time of day for the procedure are provided in table 1.
Balance measures revealed two vagal episodes on patient mobilisation in the PACU, both total hip arthroplasty (THA), four patients with uncontrollable pain in PACU and three patients with hypotension. No uncontrolled nausea prevented same-day discharge. Thirty-day ED visits for inpatient and outpatient TJAs were 8.93% and 6.15%, respectively. No outpatient TJA patients required hospital readmission within 30 days. No falls were reported during follow-up phone calls at 24 and 48 hours post discharge. No episodes of urinary retention requiring Foley catheterisation or unplanned admission were recorded.
Discussion
The purpose of this QI project was to increase the percentage of TJA performed as outpatient surgeries by establishing a dedicated outpatient clinical pathway. We achieved our aim of successfully performing a minimum of 25% of TJA as outpatient surgeries (our final rate was 33%), which translated into a significant reduction in inpatient resource utilisation. The strength of our project was that in a relatively short period during the COVID-19 pandemic, we were able to expedite the development and implementation of an outpatient TJA pathway and fill a significant clinical need.
Our QI project used and adapted previously published principles for outpatient TJA,3 4 including careful patient selection, enhanced patient education and alternative analgesia and anaesthesia techniques. Given the pain associated with TJA, ensuring optimal analgesia was crucial for success and was a barrier in the subset of patients that failed discharge on the day of surgery. Early mobilisation could not have been achieved without modifying our anaesthetic and having a dedicated PT in the PACU to assist with patient ambulation and assess discharge readiness. The needs analysis identified the requisite for explicit patient criteria, given that our patient population has complex comorbidities with 65% having an ASA classification 3 or greater.16 Most importantly, there was a clear need to maintain a parallel inpatient pathway for the more complex patients and to establish a communication process for care providers to identify whether an individual patient is a candidate for the inpatient or outpatient pathway.
A recent systematic review of 10 prospective outpatient TJA studies involving 955 patients demonstrated a 95% successful discharge rate, with only 1 major complication and no deaths.3 In our study, we observed a successful discharge rate of 84.6% with the vast majority (9/10) of failed discharges being THA cases. An audit of failed discharges via PDSA cycles highlighted variables that were amenable to future process (Appendix C). Overall, 100% of patients scheduled as the first case of the day were successfully discharged home compared with only 72% and 71% of the second and third cases, respectively, highlighting that given enough time, most TJA candidates patients can be safely discharged home from the PACU. We used this finding as an actionable item to schedule outpatient TJA candidates who have predictors of failed discharge such as anxiety, chronic pain or those undergoing THA. Other observed causes for failed same-day discharge were consistent with the existing literature (ie, hypotension and pain).4 This led us to add pre-emptive opioids and outpatient nerve catheters for analgesia and to provide more timely goal-directed resuscitation of estimated blood loss prior to patient mobilisation.
Enabling factors that contributed to the success of our initiative included having a multidisciplinary project team endorsed and supported by hospital leadership. As outlined by Parkes et al, experience and insight from multidisciplinary teams allow for a broad view of the patient with a discipline specific lens and promotes buy-in from stakeholders.26 We believe that the high adherence rate to the outpatient pathway interventions reflected change and improvement culture established by our TJA programme during prior QI initiatives.16 27 Process flow mapping of the existing inpatient pathway and identifying steps that required change proved helpful during development of the outpatient pathway. Lastly, even with extensive planning and preparation, there is no substitute for testing outpatient TJA during PDSA cycles via pilot cases.
The COVID-19 pandemic continues to pose problems globally for elective surgeries, with cancellations and rescheduling of many procedures contributing to massive surgical backlogs for millions of patients.28 Estimates from the COVIDSurg Collaborative following the initial first COVID-19 wave suggest that even if countries increased their normal surgical volume by 20% following the pandemic, it would take close to a year to clear the backlog of surgical cases caused by the first wave alone.29 Continuing to perform elective surgery, such as TJA despite the strain of the pandemic on healthcare inpatient resources, is crucial for addressing the surgical backlog and avoiding further increases to it. To ensure sustainability of the programme throughout the pandemic and beyond, we continue to fine-tune our processes. A system for postoperative virtual care follow-up has been put in place and is led by the APS. Periodic monthly audits of unsuccessful discharge home from PACU are performed by clinical champions.
In recent years, the uptake of QI science has increased globally. The COVID-19 pandemic presented an opportunity for clinical leaders to take advantage of the QI cultures and infrastructures that have gradually been evolving.30 31 QI change methodologies have already been used to help address challenges such as surges in COVID-19 hospitalisations and to perform rapid testing of new information and ideas for COVID-19 management.32 33 A UK survey of local QI leaders indicated that improvement tools have played an important role in supporting change and adaptation during the COVID-19 pandemic.34 Not surprisingly, the survey noted that ‘improvement appears to have played a more important, valuable and strategic role during COVID-19 in organisations that had a well-developed approach to improvement pre-pandemic’. This has proved true in our hospital, as rapid change groundwork for improving TJA management was already well developed and previously generated reductions in hospitalisation LOS, pain scores, opioid consumption and operating room times.16 27 Leveraging this infrastructure for developing an outpatient pathway during the pandemic was feasible and attainable in a relatively short time period.
The findings of our QI project must be interpreted within the context of their limitations. This was not a research project but rather a QI project driven by need during the COVID-19 pandemic. Advantages of outpatient TJA and some interventions needed for outpatient pathways have already been described. Furthermore, this was a single-centre project at a tertiary centre with inpatient resources and therefore our hybrid system may not be generalisable to ambulatory surgery centres that exclusively perform outpatient surgery. Despite these limitations, this project does have several strengths. It clearly exemplifies the benefits of investing in QI culture and resources, particularly during the pandemic. Furthermore, it provides an important example of how the ever-growing pandemic-induced surgical backlog may be addressed.
Conclusions
This QI initiative demonstrates the rapid implementation of an outpatient TJA pathway in response to inpatient resource constraints. This is the first example of a centre designing, testing and implementing an outpatient surgical pathway as a consequence of the COVID-19 pandemic. The rapid implementation of a hybrid inpatient/outpatient system required a dedicated multidisciplinary team and a well-established improvement culture. The findings of this report will be of interest to surgical centres facing surgical backlog and constraints on inpatient resources during and after the pandemic.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
Institutional approval was granted for implementation and ethics board approval was granted for a prospective quality improvement project.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors SP, JG and JW contributed to the design and implementation of the research. SP and JG wrote the manuscript including analysis of the results. JW and MP contributed to editing and finalising of the manuscript. SP is guarantor of this manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.