Article Text

Abstract
Despite widespread adoption of the Surgical Care Improvement Programme, the incidence of surgical site infections (SSIs) remains high. It is possible that lapses in appropriate administration of antimicrobial prophylaxis may play a role. We noted significant discordance with national guidelines with regards to intraoperative antibiotic administration at our institution, leading to implementation of a quality improvement initiative using multidisciplinary education and reminder-based interventions to improve prescribing practices and increase compliance with national guidelines. We observed a significant improvement in adherence to all aspects of antibiotic administration guidelines as a result of such interventions. Targeted multidisciplinary interventions may help improve prescribing practices of surgical antimicrobial prophylaxis and provide an opportunity to potentially decrease the burden of SSI and the related morbidity and mortality.
- infection control
- quality improvement
- surgical wound infection
- antibiotic management
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Surgical site infections (SSIs) make up approximately a third of all hospital-acquired infections and can have an appreciable impact on the rising healthcare costs.1 2 Furthermore, SSIs are a significant predictor of morbidity and mortality, with 38% of deaths in SSI patients attributed to infections.3 However, it is estimated that 40%–60% of these infections are preventable.4 Appropriate use of antibiotic prophylaxis can potentially reduce the incidence by preventing the development of infection caused by organisms that colonise or contaminate the surgical site. Studies have proven the importance and efficacy of antibiotic prophylaxis in surgical procedures,5–11 however, in order for antibiotic prophylaxis to be effective, appropriate administration practices are important.
Guidelines to address antibiotic administration prior to surgical procedures have been developed,12 and are considered the standard of care in most US hospitals, however, adherence is variable. Varying aspects of the guidelines including weight-based dosing, timing of dose and appropriate re-dosing intervals are common reasons for non-adherence.6 13–15 This non-adherence predisposes patients to an increased risk for SSIs.16 While efforts have been made nationwide to reduce the number of SSIs through the Surgical Care Improvement Project (SCIP),4 the results have been suboptimal.17 There seems to be a potential disconnect between the implementation of the programme and a measurable reduction in the SSI rate,18 and it may be possible that inappropriate administration of antimicrobial prophylaxis is one of the reasons. The goal of this quality improvement project was to improve compliance with all aspects of antibiotic administration, and we hypothesised that there would be significant improvement in adherence to national guidelines after such interventions.
Problem
Our institution is a 550-bed academic tertiary care centre with about 35 000 inpatient surgical procedures performed annually. The standard practice for surgical antimicrobial prophylaxis, prior to our interventions involved the administration of antibiotics by the anaesthesia providers as ordered by the surgical team. The type, dose and time of antibiotic administration were documented by the anaesthesia providers in the patients' electronic anaesthesia record. During the surgical ‘time-out’ (STO), the administration of antibiotics (yes/no) was discussed among the surgery providers, operating room nursing and anaesthesia providers. We found that there was significant non-adherence with the national guidelines with respect to dosing and re-dosing of antibiotics within our institution.19
Design and strategy
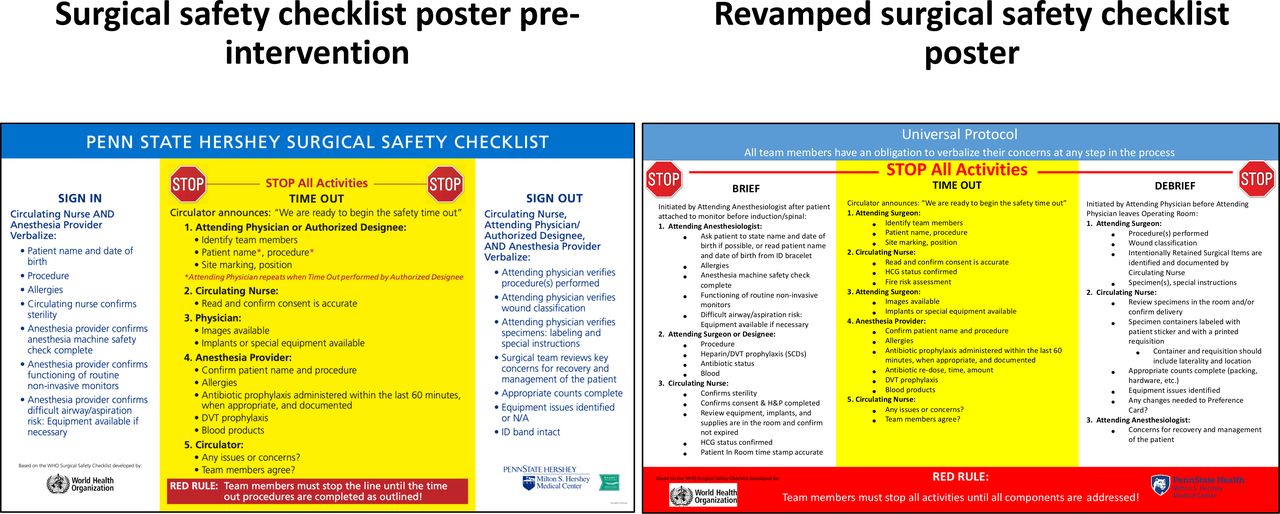
A combination of educational and reminder-based interventions was implemented targeting perioperative providers at our institution over 7 months from 1 January 2015 to 31 July 2015, with ongoing education every month in the form of email reminders. The following interventions were implemented: (1) Providing education to surgery providers (house staff, mid-level providers, faculty, operating room nursing staff) via classroom-based training sessions and email newsletters to increase awareness on appropriate choice, dosing and re-dosing intervals of antibiotics, (2) Providing similar education to anaesthesia providers (house staff, certified registered nurse anaesthetists, faculty), (3) Ensuring easy online access (via department intranet) to antibiotic administration guidelines, (4) Including the choice, dose and re-dosing intervals of antibiotics as part of the STO (figure 1), (5) Encouraging the use of reminders for antibiotic re-dosing in the electronic anaesthesia records, (6) Providing posters in all operating rooms depicting correct weight-based dosing and re-dosing intervals of commonly used antibiotics (figure 2).
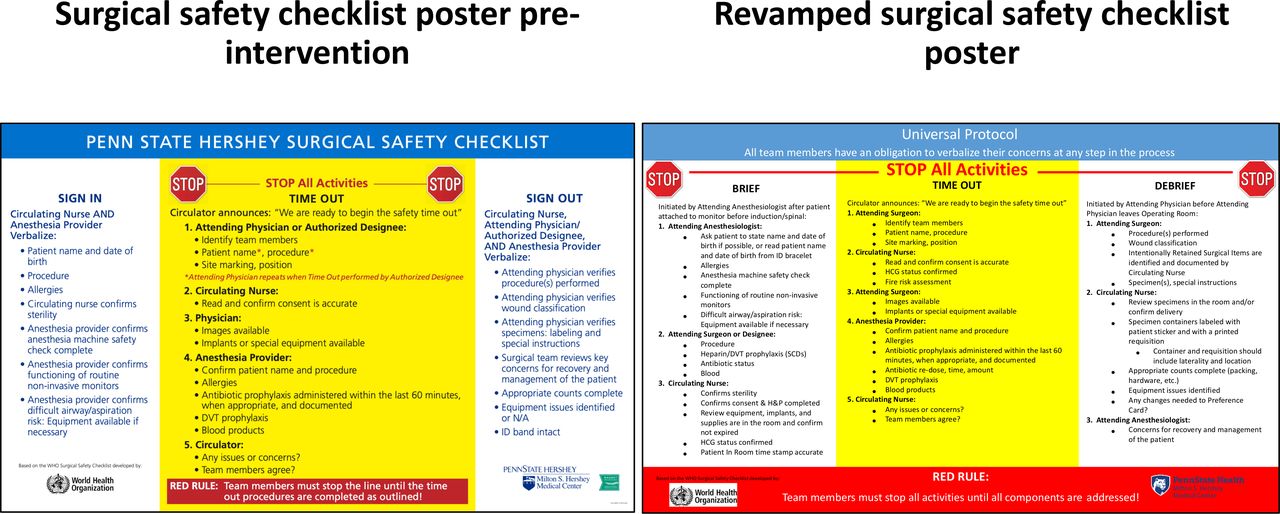
Preintervention and revamped surgical safety checklist posters depicting the inclusion of choice, dose and re-dosing intervals for antibiotics in the ‘time out’ process. SCD, sequential compression device; DVT, deep vein thrombosis; ID, identity; H&P, history and physical examination; HCG, human chorionic gonadotropin

Poster depicting correct weight-based dosing and re-dosing intervals of commonly used antibiotics.
Measurement
The appropriateness of antibiotic prophylaxis was determined by the ‘Clinical Practice Guidelines for Antimicrobial Prophylaxis in Surgery‘ which have been developed by the American Society of Health-System Pharmacists, the Infectious Disease Society of America, the Surgical Infection Society, and the Society for Healthcare Epidemiology of America.12 Adherence to these national guidelines was assessed in a preintervention and postintervention cohort of patients. The guidelines make recommendations on the choice of prophylactic antibiotics for various surgical procedures, the appropriate dose and the frequency of re-dosing. Any divergence from the guidelines in the prescription of one of the drugs led to a final assessment of the prophylactic course as discordant with the guidelines.
The study population included adult patients who had a surgical procedure at our institution with involvement of an anaesthesia provider during the surgery. There was no specific exclusion criterion. The preintervention group included patients who underwent surgery between 1 January 2013 and 31 December 2014, and the postintervention group included patients who underwent surgery between 1 August 2015 and 31 July 2017. Although approximately 35 000 surgical procedures are performed annually at our institution, and since we had already published our findings indicating inappropriate administration practices for a cohort of patients that had developed SSIs, we chose to analyse the same cohort (in a different time frame) to assess the impact of our interventions. A waiver of informed consent was granted.
The electronic anaesthesia records of the included patients were reviewed for patient demographics (age, weight, sex, allergies), surgical procedure, intraoperative antibiotic administration (name, dose, time of first dose, dosing interval) and surgery start/incision time. Patients’ allergies, weight and renal impairment, if any, were taken into consideration while evaluating the choice and dose of antibiotics. In each time period, it was determined if the established criterion for appropriate antibiotic administration was satisfied (box 1). The choice of antibiotic was considered appropriate if it met the criteria in the guidelines with respect to the type of surgery. For the dosing to be considered appropriate, standardised weight-based doses recommended in the guidelines had to be administered. The timing of the antibiotic administration was considered appropriate if the initial dose of antibiotic was administered within 1 hour of surgical incision (with the exception of vancomycin and fluoroquinolones, which had to be given within 120 min before surgical incision because of the prolonged infusion times required for these drugs). Appropriate re-dosing meant that the timing of all subsequent doses met the criteria specified for each antibiotic in the guidelines. Overall 226 patients were part of the preintervention group and 238 patients were included in the postintervention group.
Criteria for appropriate administration of surgical antimicrobial prophylaxis
Correct choice of antibiotic.
Correct dose (weight-based) of the antibiotic.
Correct timing of administration.
Correct re-dosing of antibiotic if applicable.
Statistical analysis
In each time period, counts of patients were computed for which each criterion either was or was not satisfied. The resulting values were organised into separate two-by-two contingency tables for each criterion. To test the null hypothesis that the proportion of patients meeting a given criterion was the same in each time period χ2 tests were applied, and values of p<0.05 were considered statistically significant. R V.3.4.1 (R Core Team) was used to perform all calculations.
Results
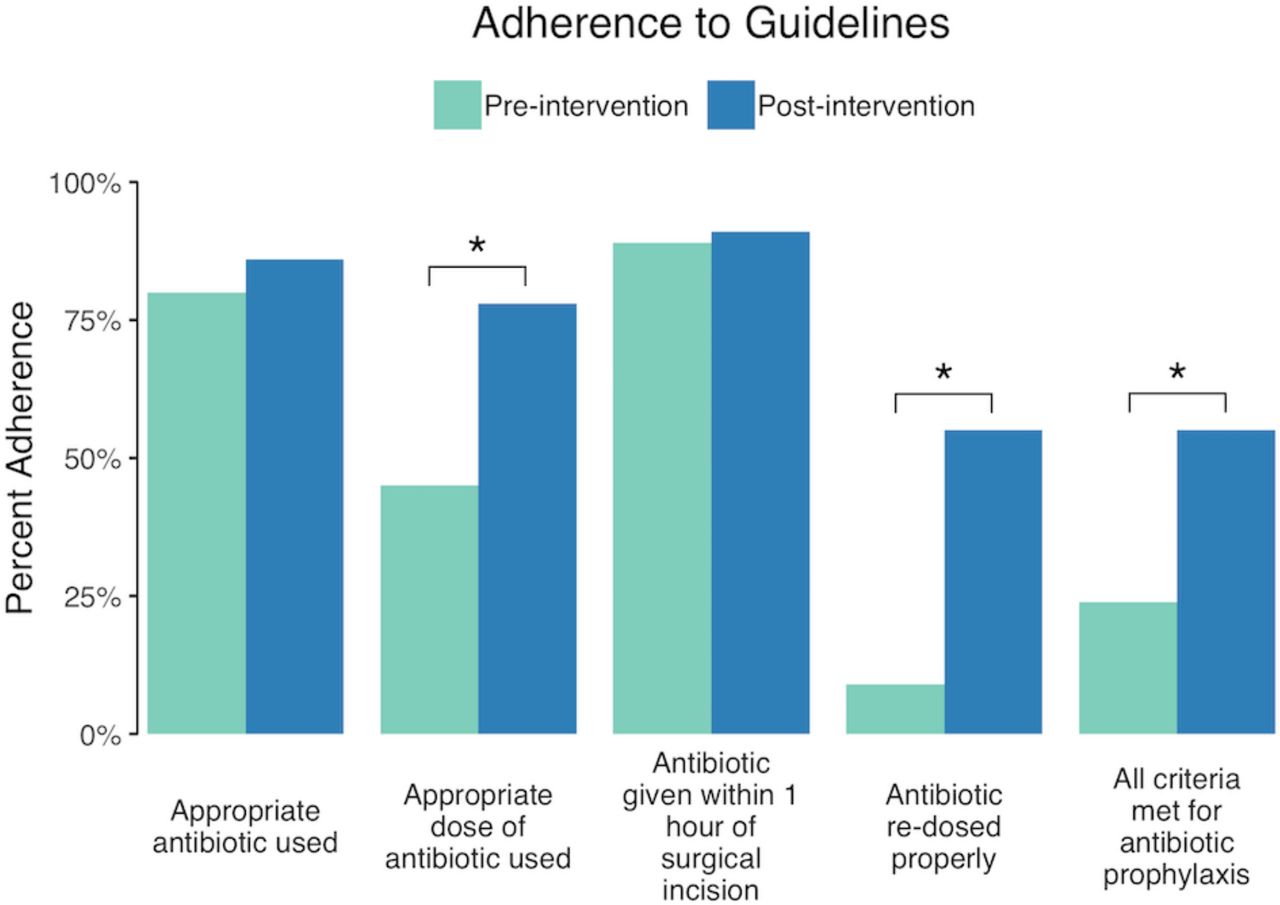
In the preintervention group, all criteria for antibiotic prophylaxis were met in 24% of patients compared with 55% in the postintervention group. There was a statistically significant difference with respect to appropriate initial dosing of antibiotics according to the guidelines, between the two groups (45% vs 78%; p<0.001). When determining the compliance with re-dosing (where applicable), we observed that 55% of patients were re-dosed appropriately in the postintervention group compared with only 9% in the preintervention group (p<0.001). There was also an improvement in the appropriate choice (80% vs 86%) and timing of antibiotic administration (89% vs 91%) between the preintervention and postintervention groups; this difference, however, was not statistically significant. The differences in various aspects of antibiotic administration between the preintervention and postintervention patient groups are illustrated in figure 3.
{kind=link}
{kind=link}
{kind=link}
Adherence to guidelines between the preintervention and postintervention patient groups.
Lessons and limitations
In this quality improvement report, we describe our efforts at improving the prescribing practices of surgical antimicrobial prophylaxis at our institution using a set of multidisciplinary interventions. We were able to show an improvement in all aspects of antibiotic administration between the preintervention and postintervention groups, with significant differences in dosing, re-dosing and the overall adherence to all the components of antibiotic administration (choice, dose, timing and re-dosing). Our report highlights the importance of targeted interventions involving all caregivers to achieve change in practice.
Significant efforts have been made to reduce the incidence of SSIs via national policy-level initiatives such as the SCIP, a programme implemented by the Centers for Medicare and Medicaid to improve perioperative outcomes.20 Additionally, guidelines have been established to help perioperative providers deliver appropriate, evidence-based surgical antibiotic prophylaxis.12 However, despite the almost universal adherence to the SCIP measures, very little, if any, reduction in SSI has occurred.17 The compliance with antibiotic administration guidelines is also variable and oftentimes suboptimal.21 In this scenario, it is possible that we might have satisfied the administrative requirement of administering antibiotics without paying attention to the appropriateness.19 Few studies have shown non-adherence to guidelines for administration of surgical antibiotic prophylaxis and have suggested educational interventions to help improve provider compliance.6 14 16 There are various reasons for non-compliance with guidelines, including, inappropriate weight-based dosing19 and improper dosing related to patient allergies.13 Since improper adherence to antibiotic prophylaxis significantly increases the risk for SSIs, it is imperative that steps are taken to improve compliance.14 Our quality improvement project is an attempt to improve intraoperative prescribing practices of surgical antibiotic prophylaxis with the overall goal to prevent the incidence of SSI.
The use of antibiotic prophylaxis is essential to prevent SSIs and may help decrease the morbidity, mortality as well as healthcare costs associated with this condition.3 8 It is important to select an effective antibiotic, administer an appropriate initial dose and follow correct re-dosing intervals when necessary to maintain effective serum and tissue levels throughout the surgery.16 In non-allergic patients, β-lactams are the most commonly recommended antibiotics for surgical prophylaxis.12 These antibiotics exhibit ‘Time-dependent killing’ and the fraction of time the drug concentration exceeds minimal inhibitory concentration is the primary determinant of effectiveness.22–30 The β-lactams also demonstrate a limited postantibiotic effect. Hence, for this class of antibiotics to be effective, the initial dose and re-dosing intervals are extremely important. Incorrect dosing and inappropriate re-dosing are not uncommon and have been reported before.6 14 16 21 Lack of awareness among providers and omission of specific details pertaining to dose and re-dosing intervals during the preincision STO are potential causes of incorrect administration.
The success of our interventions in improving overall compliance with antibiotic administration was due to an amalgamation of educational and reminder-based interventions as well as improvement in the process of STO. Educational interventions have had mixed results in this field;31 32 similarly, electronic medical record (EMR)-based decision support and reminder interventions have shown success in improving re-dosing, but not with timely administration.33 34 Adoption of a multidisciplinary approach, with modification of the STO, contributed to the significant improvement in prescribing practices at our institution. We were able to achieve significant improvements in initial dosing as well as re-dosing through interventions targeted at educating providers, providing ready-to-access resources and including discussions of dose and re-dosing intervals during the STO. We feel that such interventions are easy to institute, can be replicated and may help improve compliance with national guidelines.
The STO or pause performed immediately prior to starting the procedure is one of the three components of the ‘Universal Protocol’ which became a mandatory quality standard introduced by the Joint Commission on 1 July 2004.35 The STO, at a minimum, should include identification of the correct patient, correct site and correct procedure. An extended STO including additional quality parameters such as the anaesthetic plan, administered medications, prophylactic antibiotics administered, possible medication needed during the operation, blood product availability, need for special equipment, and so on, has been developed and found to improve communication in the operating room without disrupting workflow.36 Although our institution followed a similar STO and administration of prophylactic antibiotics was discussed, the choice, dose and re-dosing intervals were not discussed. Inclusion of such discussions in the extended STO, as a component of our multidisciplinary interventions partially explains our results. Appropriate utilisation of the STO to address the various components of antibiotic regimen (choice, dose and re-dosing interval) may be an effective way to improve adherence with prescribed guidelines and also provides an opportunity for multidisciplinary discussions prior to surgical incision. Discussions about antibiotic dosing also create awareness among the entire operating room team and promote a team-based approach rather than leaving it to the discretion of the anaesthesia provider. It also encourages the anaesthesia provider to set appropriate reminders in the electronic anaesthesia record. We feel that inclusion of such discussions in the STO is easy to implement and could be applied in varied practice models.
Our study has limitations. It is a retrospective chart review at a single tertiary academic medical center and the generalisability of our findings as well as the effect of our interventions in other hospital settings is questionable. However, our ability to improve compliance at a tertiary care academic centre with significant variability in the level of training of house staff as well as heterogeneity in advanced practice clinicians (APCs) as well as nursing staff makes us believe that these interventions can be uniformly implemented. Provider-dependent EMR documentation, lack of control study population for all patients who underwent a surgical procedure during the same time frame and lack of follow-up data to analyse the long-term effectiveness of our interventions are some of the other limitations. Finally, the inability to evaluate the impact of our interventions on patient outcomes is another limitation.
Conclusion
In conclusion, we demonstrate the importance of multifaceted, multidisciplinary quality improvement measures to improve the intraoperative prescribing practices of surgical antibiotic prophylaxis to reduce SSIs, and the associated patient morbidity and mortality. We have previously shown that merely ‘checking the box’ for antibiotic administration does not imply appropriate surgical prophylaxis and via this quality improvement project, we were able to significantly improve the dosing and re-dosing of antibiotics, as well as the overall practice of administration of surgical prophylaxis at our institution.19 Since the aim of our study was to investigate process adherence, we did not evaluate the impact of our interventions on patient outcomes. Although a direct relationship between prophylactic antibiotic administration and SSI rate has not been established, it has been proven that appropriate use of antibiotic prophylaxis can prevent the organisms that colonise or contaminate the surgical site from causing an infection.4 Thus, we believe that improvement in the administration of surgical prophylaxis can potentially reduce the risk of SSI, and further studies are needed to assess that impact.
References
Footnotes
Twitter @KunalKaramchan2
Contributors VH and SM helped conduct the study and prepare the manuscript. JP and DB helped plan the study and edit the manuscript. KK helped conceptualise and conduct the study and prepare the manuscript.
Funding SM was supported by the National Center for Advancing Translational Sciences, NIH Grants TL1 TR002016 and UL1 TR002014. The content is solely the responsibility of the author and does not necessarily represent the official views of the NIH.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Ethics approval The Institutional Review Board approved the research protocol (Study no. 2950).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon request.