Article Text

Abstract
Aim To reduce the number of invalid surgical consents in the Singapore National Eye Centre Day Surgery Unit over a period of 6 months.
Methodology A multidisciplinary team involving doctors, nurses, day surgery unit, operating theatre, listing and clinical audit staff looked into the listing process and the root causes of the high number of invalid consents. A Pareto chart detailing the top causes of invalid consents was drawn, and with a prioritisation matrix, feasible yet effective changes were identified and effected. Plan-Do-Study-Act (PDSA) cycles included moving consent checks upstream, getting invalid consents amended on the same day, sending emails to raise awareness on invalid consents and posters in clinics to emphasise the correct way to fill up consent forms.
Result There has been a progressive downtrend in the monthly mean percentage of invalid consents since the introduction of PDSA cycles. There was a significant reduction in the mean rate of rejected consents from the preintervention phase of 15.2% to the postintervention phase of 11.3%, shown with a Z score of 6.56 (P<0.05). Sustainability was also demonstrated with multiple consecutive points below the median of 14.5% on the postimplementation phase of the run chart, with estimated time-efficiency savings of USD$19 738.50 annually.
Conclusion Errors in the workplace can be reduced with a concerted effort from multiple stakeholders. It is important to have a thorough look at processes with concerned parties, so that different perspectives and skill sets can be harnessed to determine and implement feasible and effective interventions.
- compliance
- human error
- quality improvement
- root cause analysis
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Problem description
Informed consent for elective surgery has become increasingly important, given the increasing medicolegal litigation,1 and desire to provide patients with more autonomy2 regarding their own treatment. The acquisition of informed consent occurs during the clinical consult, where the risks, benefits and alternatives of any surgical procedure are explained by the surgeon. This process is subsequently documented in a consent form where the doctor, witness and the patient or proxy acknowledges that the process has taken place, usually in the form of a signature or thumbprint. Without any documentation of this process, surgery will not be able to take place.
Problems arise when this documentation process is incomplete or invalid, based on common sense or centre standards. This is especially likely in a national tertiary care and training centre, where surgeons or surgeons-in-training who obtain informed consent are not necessarily the ones performing the surgery for the patient.
In our centre, revalidation of erroneous consents is often performed just before the surgery, in the day surgery unit while the patient is being prepared for the procedure. This results in time wasted by various parties—doctors, day surgery unit nurses, operating theatre staff, patients and their caregivers, while waiting for the consent to be retaken. Potential medicolegal issues arise as well, particularly because the doctor revalidating the consent may not necessarily be a surgeon or surgeon-in-training who understands the procedure that is being revalidated. Who will bear the medicolegal implications should they arise?
Available knowledge
There is currently no available knowledge in the literature regarding invalid surgical consents, the rates of revalidation and the time and effort wasted from doing so. Anecdotal evidence from patients, nurses and surgeons (in the form of solicited and unsolicited feedback) have demonstrated that it is becoming a prevalent problem, especially with the hire of new staff (nurses and surgeons) and the increasing number of surgeries in our centre.
Rationale
During a 1-year period from May 2014 to May 2015, an audit was conducted to determine the baseline rate of consents that were deemed invalid and hence rejected in the day surgery unit. Data were collected from one representative work week every month from May 2014 to April 2015 and every work day in May 2015. All patients who were scheduled for day surgery in Singapore National Eye Centre (SNEC) were included in the analysis. Because data were collected as part of the institution’s regular work processes, it was not deemed necessary to obtain patient consent or to obtain approval from the Central Institutional Review Board.
Data collected over the year showed that out of 4 805 surgeries listed in the sampled period, a monthly mean of 15.2% (SD 2.81%) and median of 14.5% of consents were determined invalid and had to be retaken. To help the team with determining the impact of invalid consents, mean time required to retake each consent was also measured—10 minutes for doctors, 2 minutes for day surgery unit nurses, 10 minutes for patients and 8 minutes for operating staff.
Assuming a baseline rate of 27 000 eye surgeries done per year in our centre, this translates to 4 050 consents retaken annually.
Specific aims
In this study, we aim to reduce the number of invalid surgical consents in day surgery patients of SNEC to less than 10% within 6 months.
Methods
We used quality improvement (QI) methodology in which evidence-based interventions are developed to achieve optimal outcomes at minimal essential cost. It involves a comprehensive systemic view of the consent-taking process, encompassing surgeon and patient characteristics, clinical and administrative work flow and outcomes.3
The QI project was carried out in four phases. In the diagnostic phase, a baseline analysis was conducted to assess the root causes of the problem. In the intervention phase, the team—two ophthalmologists (WC and ACYF), one nurse clinician (LHP), audit personnel (YLY), surgery listing personnel (Tze Ching Lim) and four nurses (APHN, EMLN, VLES and JKJO) from the day surgery unit, operating theatre, private and subsidised clinics, respectively—used various QI tools to identify areas for improvement and potential solutions, which were then put through a few rounds of Plan-Do-Study-Act (PDSA) cycles4 in the implementation phase. Throughout this phase, data were continuously collected and analysed to evaluate the impact of the implemented measures.
Although the project started in June 2015 and was slated to end in December 2015, data collection was extended until May 2016 to determine if the impact of the project could be sustained over a prolonged period. This final sustaining phase is important in ensuring that QI projects yield long-lasting gains instead of fleeting success.
Setting
SNEC is the single designated institution in Singapore’s public healthcare sector that specialises in ophthalmological services. It has an annual workload of 300 000 outpatient visits, 27 000 major eye surgeries and 13 000 laser procedures.
This project was supported by the Quality Assurance Committee of the SNEC and facilitated by the Enhancing Performance Improving Care (EPIC) Framework run by SingHealth—one of the major public healthcare clusters of hospitals and specialty centres, of which SNEC is a part. The framework facilitated the project by sharing its expertise and knowledge on the various QI methodologies and by providing consultation services throughout the course of the project.
Diagnostic phase
Identifying problems
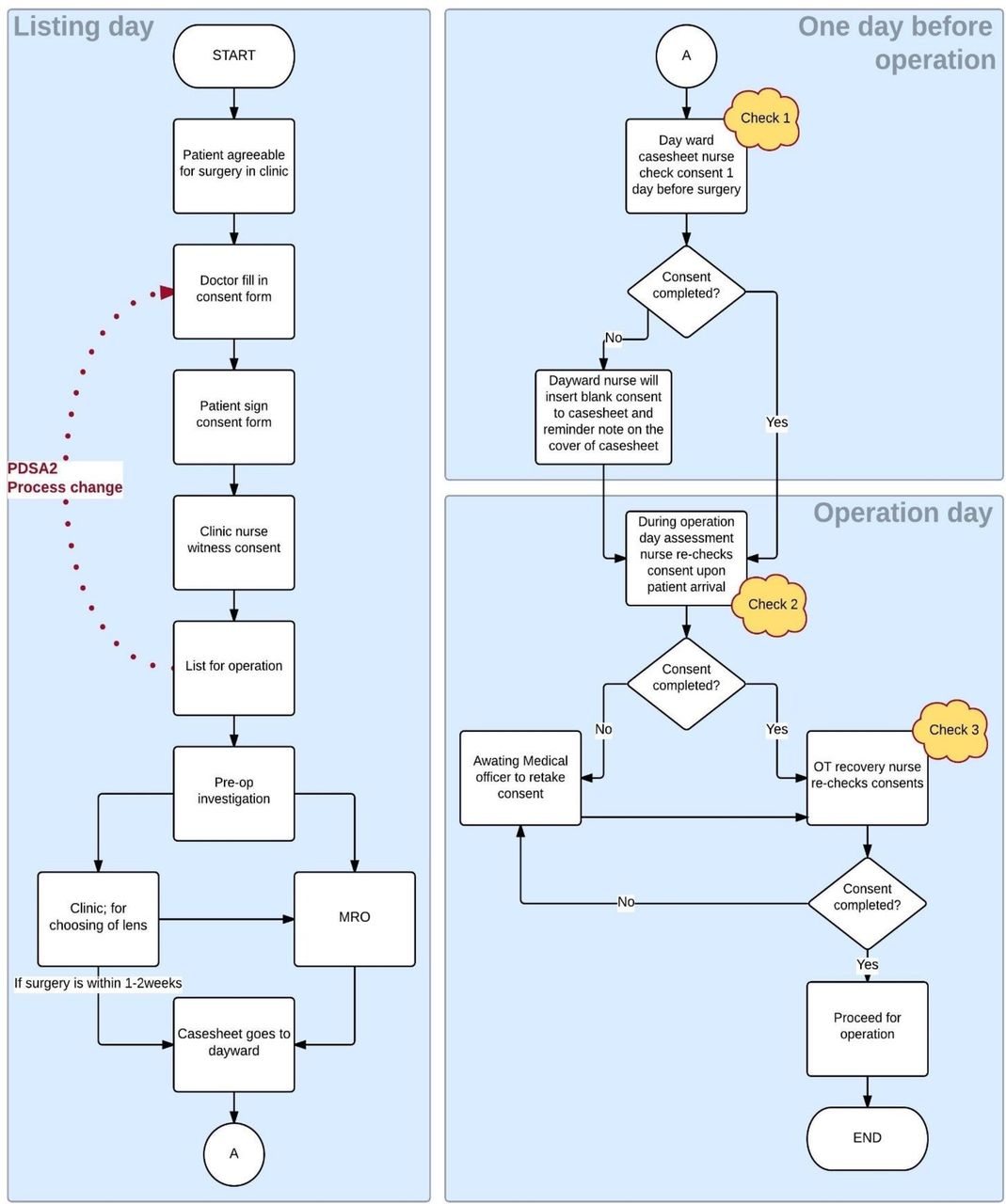
The team leaders (WC and ACYF) spoke to external customers (patients, relatives) and internal stakeholders (surgeons, nurses from various departments, listing staff, operating theatre staff and QI facilitators) to determine the problems faced with invalid consents and the impact it had on the centre—delayed surgery, unnecessary need for surgeons to travel to the day surgery unit to retake invalid consents, relatives and patients having to undergo the consent process under pressure (just before entering the operating theatre). Next, the team mapped out a flow chart of the existing key work processes that occurred from the time consent is obtained to the time patients enter the operating theatre (figure 1).

Existing workflow process—consent taking to operation theatre—three consent checks on D −1 and D0 of surgery (Plan-Do-Study-Act (PDSA) cycle 2 reflected in red).
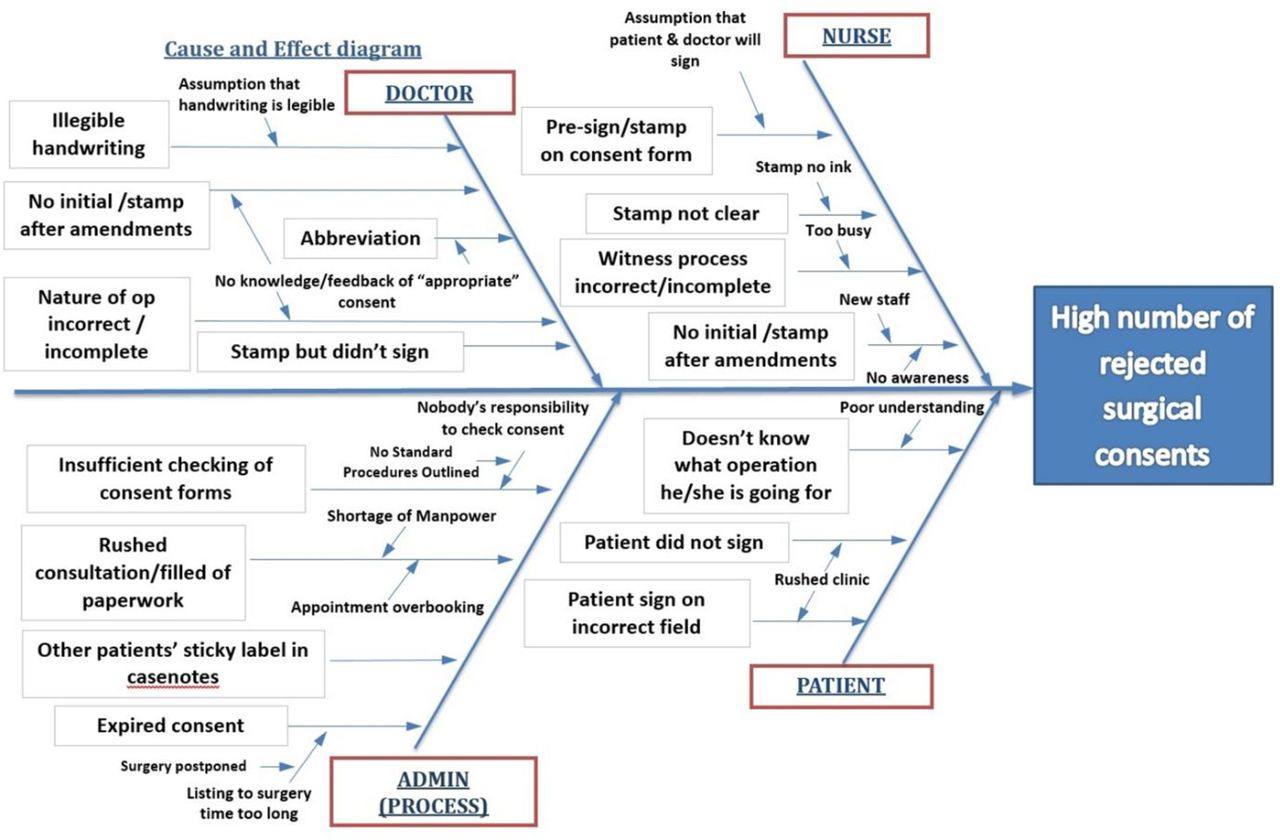
Based on our previous audit, factors contributing to invalid consents in the day surgery unit were identified retrospectively. These factors were then grouped together, and a group brainstorming session was then carried out to understand the underlying problem, which was then organised into an Ishikawa fishbone cause and effect diagram (figure 2).

Cause and effect diagram—causes of invalid consents.
Next, a Pareto chart was created based on our data to identify the top causes accounting for 80% of the rejected consents (figure 3), which were as follows:
No initials or identification made after amendments to consent forms.
Witness initials or identification were incomplete or absent.
Consent forms were expired.
Dates written were incomplete or absent.
Handwriting was illegible.
Abbreviations were used to describe the nature of the procedure.
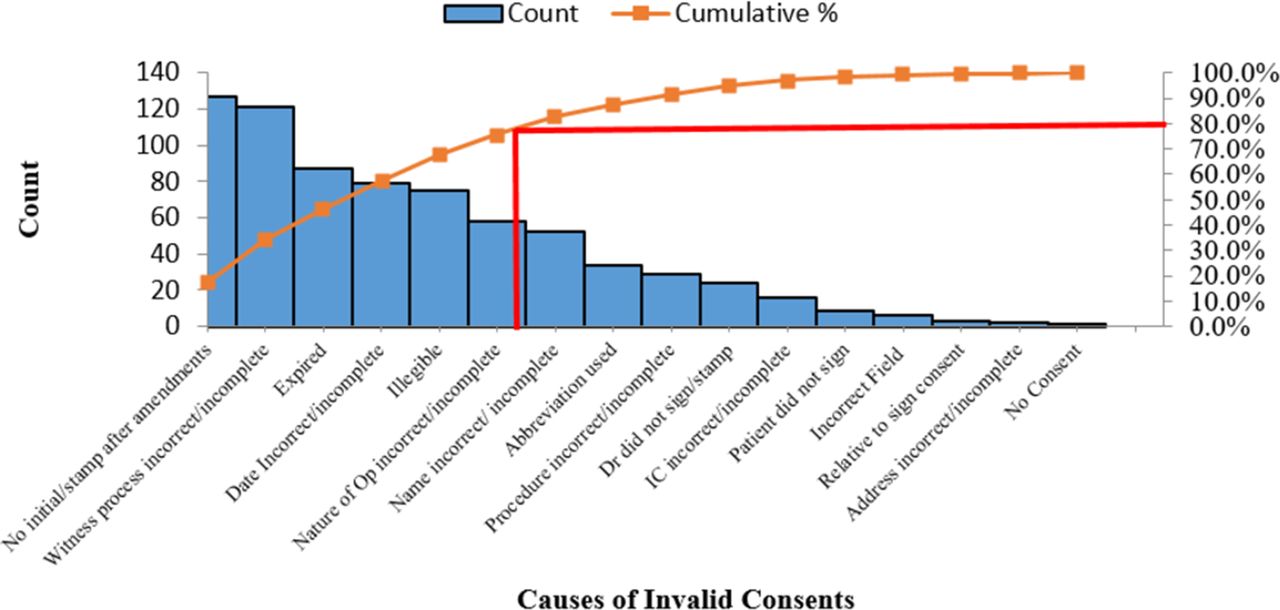
Pareto chart—top causes of invalid consents.
We found the majority of consent forms were determined invalid as they did not conform to our centre standards for a proper consent taken. Many rejected forms did not have clear identification or initials when amendments were made, and the witness was not identifiable. Dates were written incoherently (different dates on each section) when they should all correspond to the same date when all parties present—surgeon, patient and witness—to take part in the process. Also, illegible handwriting from particular surgeons often contributed to invalid consents. Expired consent forms posed a significant problem as well, as they have a limited validity of 90 days (an institution-wide policy) from the day it was taken, to the date of surgery. Unfortunately, a significant proportion of patients postpone their surgeries due to new concomitant medical conditions.
Devising intervention strategies
A group brainstorming session was then carried out to conceive ideas and devise new intervention strategies to address the identified causes of rejected surgical consents. These ideas were then put through a prioritisation matrix (figure 4) to determine which ones should be acted on.

Prioritisation matrix. JCI, Joint Commission International.
Implementation phase
Based on the prioritisation matrix, our team proceeded to plan and carry out two specific interventions.
First intervention
Implementation of the first intervention officially commenced in the second week of June 2015. An email highlighting the problem with rejected consents and containing a pictorial representation of common errors in consent forms and how they should have been filled was sent centre wide (Supplementary appendix—PDSA Cycle 1—Email sent Centre wide) . Awareness was raised by prominently displaying posters in all consultation rooms, with the issue highlighted at centre-wide briefings, explaining common errors in consent forms (Supplementary appendix—PDSA Cycle 1—Poster Displayed in Clinic). Our team believed that the lack of awareness led to a significant proportion of consents being invalid and most staff not understanding the reason why their documentation was deemed so. This was possibly due to lack of a feedback loop, as the day surgery unit nurse and/or surgeon tasked with revalidating consents was not the one who obtained the erroneous consent on the day of consultation, hence, leading to our second intervention.
Supplementary file 3
Second intervention
Our second intervention involved bringing forward consent validity checks to the day of consultation and incorporating it as a process for listing patients for surgery (figure 1—PDSA 2). It was first implemented for patients in clinics on the first floor of SNEC for a week (PDSA Cycle 2A), before being spread centre wide (PDSA Cycle 2B). Listing staff were given talks and hands-on training to teach them how to identify invalid consent forms. Forms explaining why the consent was invalid and what amendments to be made were attached to case sheets with invalid consents and redirected back to the clinician (Supplementary appendix—PDSA Cycle 2—Form). Our team believed that rather than checking for errors on the day before or on surgery day, bringing forward the validity checks to the day of consultation had two advantages. First, it instituted and closed the feedback loop so that the erroneous surgeon or witness were aware of their mistakes. Second, it also avoided the time wastage and last minute revalidation of consent forms in the day surgery unit just prior to surgery.
Supplementary file 7
Study of the interventions
Rate of invalid consents
As determining whether a surgical consent is valid only starts one day prior to surgery—and the time interval from obtaining consent till the date of surgery can range from a few days to 3 months, our interventions could not reflect any immediate or real-time changes in the rates of invalid consents. Hence, study of our interventions were necessary by two measures—one immediate and specific to the intervention and the other in its ability to reduce the number of invalid consents in the long run (up to a period of 3 months). As the interventions were being implemented, the rate of invalid consents at the day surgery unit were continuously tracked.
Study of the first intervention
The first intervention was evaluated in terms of its efficacy in raising awareness among the doctors, nursing and listing staff and in the long term reducing the number of invalid consents. To assess awareness, a preintervention quiz was conducted. Subjects were asked to identify mistakes in two incorrectly filled consent forms (Supplementary appendix—PDSA Cycle 1—Quiz). They were then scored out of six (three mistakes in each consent form) and a postintervention quiz was then repeated with comparison of preintervention and postintervention scores to determine the effectiveness of our intervention.
Study of the second intervention
Study of our second intervention looked at the pick-up rate for invalid consents by listing staff, before the case sheets reach the day surgery unit. Consents screened by listing staff and determined invalid were recorded down, and the pick- up rate monitored on a data collection sheet (Supplementary appendix—PDSA Cycle 2—Data Collection Sheet). Data were collected for the week of PDSA Cycle 2A to determine their effectiveness in picking up invalid consents and collected again as an audit during PDSA Cycle 2B when changes were implemented centre wide to determine if the implementation’s effectiveness has been maintained. Problems encountered along the way included low pick-up rates by listing staff due to unfamiliarity with this new task, leading to a recertification session conducted as a subsequent PDSA cycle. Table 1 lists the actions taken in each PDSA cycle.
Supplementary file 6
Plan-Do-Study-Act Cycles (PDSA), June 2015–September 2015
Results
Rejected consents
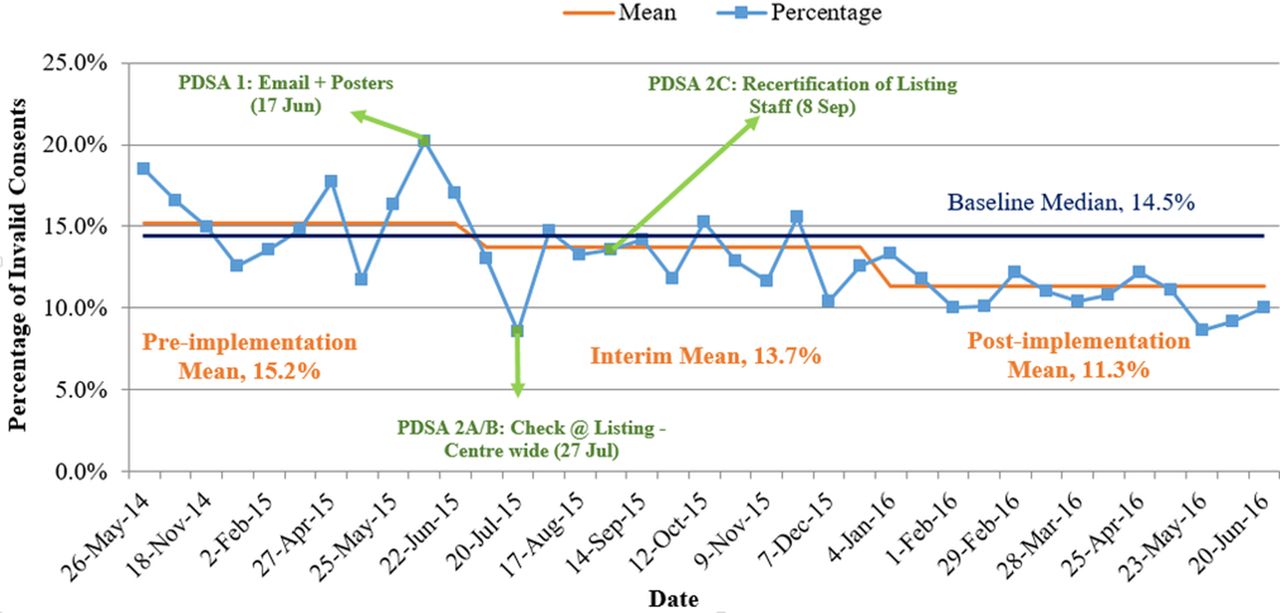
The run chart in figure 5 shows the impact of our QI project on the rate of rejected consents in the day surgery unit from June 2015 to May 2016. As the date of surgery ranged from a few days to 3 months from the date of consultation, the results of our interventions inevitably required time to show effect. After going through the PDSA cycles, the implemented changes reduced the monthly rate of rejected consents from 20.2% in June 2015 to 8.6% in May 2016.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
![[bmjoq-2017-000167-SP3.jpg]](https://bmjopenquality.bmj.com/content/bmjqir/7/1/e000167/DC1/embed/inline-supplementary-material-1.jpg?download=true){kind=link}
![[bmjoq-2017-000167-SP7.jpg]](https://bmjopenquality.bmj.com/content/bmjqir/7/1/e000167/DC2/embed/inline-supplementary-material-2.jpg?download=true){kind=link}
![[bmjoq-2017-000167-SP6.jpg]](https://bmjopenquality.bmj.com/content/bmjqir/7/1/e000167/DC3/embed/inline-supplementary-material-3.jpg?download=true){kind=link}
{kind=link}
Biweekly runchart from May 2015 to June 2016. PDSA, Plan-Do-Study-Act.
Although the project was originally scheduled to end in December 2015 (a 3-month allowance was given from time of last intervention (September 2015) for interventions to show results), data collection continued through till May 2016 to assess if the project’s results were consistently maintained.
There was a significant reduction in the mean rate of rejected consents from the pre-intervention phase (before June 2015) of 15.2% to the post-intervention phase (after December 2015) of 11.3%, shown with a Z score of 6.56 (P<0.05). Sustainability was also demonstrated with multiple consecutive points below the median of 14.5% on the post-implementation phase of the run chart.
Cost savings
The project has resulted in significant time-efficiency savings for the centre. The reduction in rate of invalid consents by 30.6% saved time and potential costs for all parties involved. With a baseline assumption of 27 000 surgeries done in SNEC per year, there is an estimated reduction of 110 invalid consents per month since the implementation of our project.
Relying on our diagnostic phase estimates, this translates to monthly time savings of 1100 minutes by doctors, 1100 minutes by nursing and operating staff combined and 1100 minutes by patients and their caregivers. Based on human resource estimates on hourly wages of doctors, nurses and average Singaporeans, annual time-efficiency savings for the centre and patients can potentially be valued up to S$25 850 (S$13 750 + S$5 500 + S$6 600, respectively) or USD$19 378.50 (one Singapore dollar equals approximately 0.75 US dollar), if the rate of invalid consents remain at its new baseline.
Discussion
By reducing the rate of invalid surgical consents, this QI project saved time for all parties — doctors, day surgery unit nurses, operating theatre staff, patients and caregivers. Validating consents on the day of consultation also created a tight feedback loop between the surgeon and listing staff, allowing the surgeon to be aware of his/her mistakes, and alongside avoiding scenarios where patients are rushed through the consent-taking process just before surgery. The time-cost savings are also significant and could potentially increase as the number of surgeries in SNEC increase annually.
Despite the relative success in decreasing the number of invalid consents, the project had a few limitations. For example, system-inherent factors such as legal processes limited the consent form validity to 90 days, and changing it would have to involve institution-wide reviews and amendments, which our team did not have the authority or resources to do so. In addition, there was a delay in the realisation of the results of our intervention, as changes instituted on consultation/listing day do not manifest till the patient’s case sheets are checked for validity in the day surgery unit later on. This made reviewing the efficacy of our interventions difficult as the turnaround time was prolonged and variable. The team also noted that there was an element of variability in deciding whether a consent was invalid — the legibility of handwriting could be open to interpretation depending on familiarity with the procedure, as well as the surgeon involved. This may account for the inter-month variability in the rate of invalid consents.
To ensure that our efforts are sustained, the team will continue to monitor the rate of rejection of invalid consents by sampling 1 week of day surgery cases once every 3 months. Orientation programmes for new staff will also include a briefing on the proper consent documentation process, with posters prominently displayed in all clinics to remind everyone how it should be done. In the future, when electronic medical records are implemented in our institution, legibility errors in consent forms should also be markedly reduced.
Conclusion
The process of QI need not be a costly or complicated process. As the present project demonstrates, significant time savings for staff and patients can be made through simple retrospect and adjustments to work flow processes.
Supplementary file 1
![[bmjoq-2017-000167-SP1.jpg]](https://bmjopenquality.bmj.com/content/bmjqir/7/1/e000167/DC4/embed/inline-supplementary-material-4.jpg?download=true){kind=link}
Supplementary file 2
![[bmjoq-2017-000167-SP2.jpg]](https://bmjopenquality.bmj.com/content/bmjqir/7/1/e000167/DC5/embed/inline-supplementary-material-5.jpg?download=true){kind=link}
Supplementary file 4
![[bmjoq-2017-000167-SP4.jpg]](https://bmjopenquality.bmj.com/content/bmjqir/7/1/e000167/DC6/embed/inline-supplementary-material-6.jpg?download=true){kind=link}
Supplementary file 5
![[bmjoq-2017-000167-SP5.jpg]](https://bmjopenquality.bmj.com/content/bmjqir/7/1/e000167/DC7/embed/inline-supplementary-material-7.jpg?download=true){kind=link}
Footnotes
WC and ACYF contributed equally.
Contributors WC and ACYF contributed equally as first authors.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.