Article Text

Abstract
Introduction Chronic, non-cancer, axial or radicular spinal pain is a common condition associated with considerable socioeconomic burden. Clinicians frequently offer patients various interventional procedures for the treatment of chronic spine pain; however, the comparative effectiveness and safety of available procedures remains uncertain.
Methods We will conduct a systematic review of randomised controlled trials that explores the effectiveness and harms of interventional procedures for the management of axial or radicular, chronic, non-cancer, spine pain. We will identify eligible studies through a systematic search of Medline, EMBASE, CINAHL, Cochrane Central Register of Controlled Trials and Web of Science from inception without language restrictions. Eligible trials will: (1) enrol primarily adult patients (≥18 years old) with axial or radicular, chronic, non-cancer, spine pain, (2) randomise patients to different, currently available, interventional procedures or to an interventional procedure and a placebo/sham procedure or usual care, and (3) measure outcomes at least 1 month after randomisation.
Pairs of reviewers will independently screen articles identified through searches and extract information and assess risk of bias of eligible trials. We will use a modified Cochrane instrument to evaluate risk of bias. We will use frequentist random-effects network meta-analyses to assess the relative effects of interventional procedures, and five a priori hypotheses to explore between studies subgroup effects. We will use the Grading of Recommendations Assessment, Development and Evaluation approach to assess the certainty in evidence for each outcome, including direct, indirect and network estimates.
Ethics and dissemination No research ethics approval is required for this systematic review, as no confidential patient data will be used. We will disseminate our findings through publication in a peer-reviewed journal and conference presentations, and our review will support development of a BMJ Rapid Recommendations providing contextualised clinical guidance based on this body of evidence.
PROSPERO registration number CRD42020170667.
- pain management
- rehabilitation medicine
- back pain
- spine
- interventional radiology
- pain management
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Our broad study eligibility criteria and consideration of trials in any language will increase generalisability of our results.
We will use the Grading of Recommendations Assessment, Development and Evaluation approach to evaluate our certainty in treatment effects.
We will optimise interpretability by presenting risk differences and measures of relative effect for all outcomes reported, and by presenting findings for comparative effectiveness of interventional procedures using a minimally-contextualised approach that considers effect estimates, precision and certainty of evidence.
Our results will be limited by possible shortcomings of primary studies.
Introduction
Chronic, non-cancer, spinal pain is defined as any painful condition, local (axial) to or radiating from (radicular) the spine, that persists for more than 3 months and is not associated with a diagnosis of cancer.1 Chronic non-cancer pain is a complex and multifactorial condition that continues to be a significant health challenge worldwide, and is associated with considerable socioeconomic burden.2 In Canada, population-based surveys conducted between 1994 and 2008 suggest 15%–19% of adults live with chronic non-cancer pain,3 with 21% related to spinal conditions.4 Twenty percent of US adults currently live with chronic non-cancer pain, and the prevalence of chronic low back pain in US adults aged 20–69 years old is estimated to be 13%.5 6 Similarly, 19% of adult Europeans are affected by chronic pain of moderate to severe intensity, among whom approximately half report back pain.7
Clinicians frequently offer patients non-surgical interventional procedures such as epidural steroid injections, medial branch blocks and radiofrequency ablation for the management of chronic non-cancer spinal pain.8 9 However, clinical practice guidelines provide conflicting recommendations regarding their use. The 2009 American Pain Society guideline found insufficient evidence to make recommendations for the use of most interventional procedures.10 In 2013, the American Society of Interventional Pain Physicians (ASIPP) stated there was fair to good evidence to support the use of many interventional therapies for chronic spinal pain.1 11 In 2016, the National Institute for Health and Care Excellence (NICE) recommended against spinal injections for managing low back pain,12 and in 2018 the UK National Health Services proposed to defund injections for non-specific low back pain without sciatica due to the lack of supporting evidence.13 In 2020, NICE updated their guideline and reaffirmed this recommendation.14 In 2020, the ASIPP released their updated guideline reaffirming recommendations in favour of radiofrequency ablation, nerve blocks and facet joint injections for chronic neck, mid-back and low back pain,15 and in 2021 the ASIPP published guidelines recommending epidural steroid injections for chronic spinal pain secondary to disc herniation, spine stenosis, discogenic pain and postsurgery syndrome.16
There are several conventional systematic reviews that have explored the effectiveness of interventional procedures for chronic non-cancer spinal pain17–19; however, they do not explore the relative effectiveness of competing interventions. Two systematic reviews with network meta-analysis (NMA) have focused on interventional procedures for spinal pain,20 21 but each combined acute and chronic pain complaints and none assessed the overall certainty of the evidence. Thus, we propose to conduct a systematic review and NMA of randomised trials to assess the comparative effectiveness and harms of available interventional procedures for the treatment of patients with chronic, axial or radicular, non-cancer, spinal pain.
Methods
Standardised reporting and registration
We prepared our protocol in accordance with the Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols checklist.22
Eligibility criteria
We will include randomised trials that: (1) enrolled participants among which at least 80% were adult patients (≥18 years old) presenting with chronic, axial and/or radicular, non-cancer spine pain (pain with ≥12 weeks duration or defined by authors as ‘chronic’) and (2) randomised patients to alternative, currently available, interventional procedures or to an interventional procedure and a placebo/sham procedure or usual care. We will include trials that allowed co-interventions, if patients in all study arms received the same co-interventions (eg, exercise, physiotherapy). Table 1 provides further details of our inclusion and exclusion criteria.
Study eligibility criteria
Data sources and search strategy
An experienced medical librarian (RJC) developed and refined our search strategy for individual databases (online supplemental appendix 1). We will conduct our systematic searches for eligible studies in Medline, EMBASE, Cumulative Index to Nursing and Allied Health Literature (CINAHL), Cochrane Central Register of Controlled Trials (CENTRAL) and Web of Science without language restrictions. We will review the reference lists of included trials and relevant reviews for additional eligible studies.
Supplemental material
Study selection
Pairs of trained reviewers will screen titles and abstracts of identified citations independently and in duplicate, using a standardised, pilot-tested form. Subsequently, reviewers will assess full texts of potentially eligible studies. Reviewers will resolve any disagreements through discussion or by adjudication with a third reviewer. We will use DistillerSR, an online systematic review software (Evidence Partners, Ottawa, Canada; http://systematic-review.net) for screening titles and abstracts and full-text articles. We will contact study authors if limitations in reporting lead to uncertainties in eligibility.
Data extraction
We designed a standardised form and a detailed instruction manual for data abstraction. We will conduct calibration exercises prior to starting the abstraction process to promote consistency and accuracy of extracted data. Six pairs of reviewers will extract data independently and in duplicate.
For all included studies, reviewers will abstract the following data: study characteristics (eg, bibliographic information, country of origin, funding source), participant characteristics (eg, sample size, age and sex of participants, location and severity of pain, clinical diagnosis, duration of pain, the proportion of patients involved in litigation or receiving disability benefits), characteristics of interventions and comparators (eg, number and frequency of procedures, overall treatment duration, length of follow-up), characteristics of healthcare providers (eg, experience performing interventional procedures or formal certification), use of image guidance and patient-important outcomes as guided by the Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials recommendations,23–25 including pain intensity, physical functioning, emotional functioning, role functioning, social functioning, sleep quality, return to work, opioid use and adverse events. All abstracted information will be recorded in an excel spreadsheet (Microsoft Office Excel 2019). We will contact the authors of included trials for unreported data or additional details when necessary. We will investigate the potential clinical and statistical heterogeneity of non-interventional control arms (eg, usual care, standard care, exercise) to determine whether to consider them as a single node.
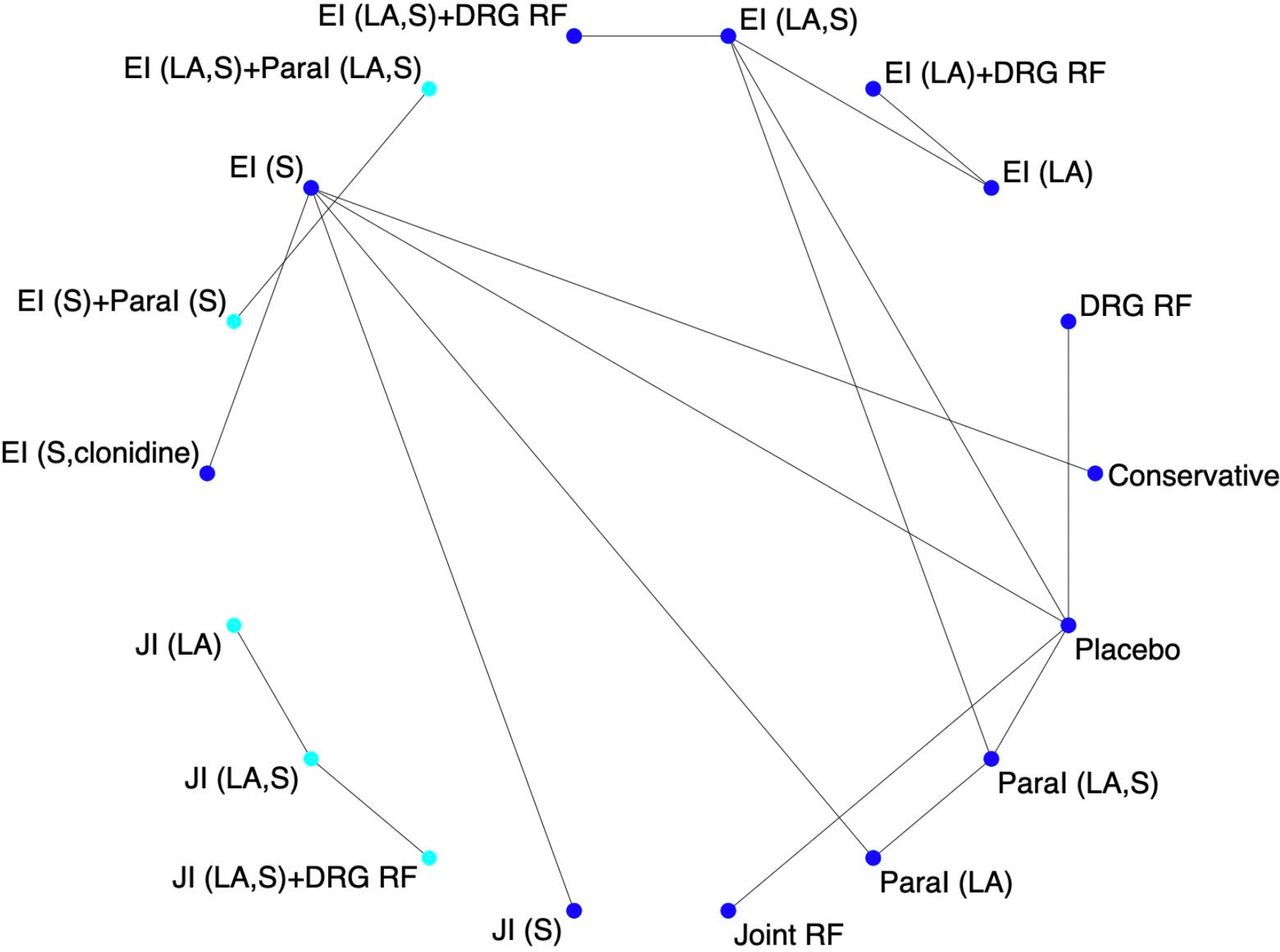
A preliminary literature search suggests there will be approximately 100 trials eligible for this review, and figures 1 and 2 illustrate potential networks of treatments that may be developed.

Model network of possible pairwise comparisons of interventional procedures for chronic axial spine pain (from a preliminary search of the literature). LA, local anaesthetic, including lidocaine, bupivacaine, ropivacaine, carbocaine; S, steroids, including betamethasone, methylprednisolone, triamcinolone, dexamethasone, hydrocortisone; conservative: conservative therapies, including oral analgesics, exercise, standard treatment as per described; JI, joint injection (facet intraarticular injection or medial branch injection, or sacroiliac joint injection); RF, radiofrequency ablation (joint RF is radiofrequency ablation for the facet joint or sacroiliac joint, DRG RF is radiofrequency ablation of dorsal root ganglion); EI, epidural injection (transforaminal epidural, interlaminar epidural or caudal epidural); ParaI, paravertebral injection; TPI, trigger point injection; MI, intramuscular injection along the spine.
{kind=link}
{kind=link}
Model network of possible pairwise comparisons of interventional procedures for chronic radicular spine pain (from a preliminary search of the literature). LA, local anaesthetic, including lidocaine, bupivacaine, ropivacaine, carbocaine; S, steroids, including betamethasone, methylprednisolone, triamcinolone, dexamethasone, hydrocortisone; conservative: conservative therapies, including oral analgesics, exercise, standard treatment as per described; JI, joint injection (facet intraarticular injection or medial branch injection, or sacroiliac joint injection); RF, radiofrequency ablation (joint RF is radiofrequency ablation for the facet joint or sacroiliac joint, DRG RF is radiofrequency ablation of dorsal root ganglion); EI, epidural injection (transforaminal epidural, interlaminar epidural or caudal epidural); ParaI, paravertebral injection.
Risk of bias assessment
Pairs of reviewers will independently assess the risk of bias (RoB) among eligible studies using a modified Cochrane risk of bias instrument, which includes response options of ‘definitely yes’ and ‘probably yes’ (assigned low RoB), and ‘probably no’ and ‘definitely no’ (assigned high RoB). A revised Cochrane tool has been published (RoB 2); however, formal testing has found low interrater reliability and challenges in applying this instrument.26 We will assess the following RoB criteria: random sequence generation; allocation concealment; blinding of participants, healthcare providers, data collectors, outcome assessor/adjudicator and incomplete outcome data (≥20% missing data will be considered high RoB).27 Any disagreements between reviewers will be resolved through discussion or with the help of an adjudicator.
Data synthesis
For direct comparisons, we will pool all outcomes reported by at least two trials addressing the same comparison. We will narratively describe study results if quantitative synthesis is not possible. For dichotomous outcomes that are reported by >1 randomised controlled trial (RCT), we will calculate the relative risk (RR) and the associated 95% CIs to inform relative effectiveness.
For continuous outcomes that are reported by >1 RCT, we will calculate the weighted mean difference and associated 95% CI. We will use the methods described in Cochrane Handbook28 and by Hozo et al29 to impute means and SDs when only median, range and sample size are reported, or to impute the SD when the SE or SD for the differences are not reported and we are unable to acquire these details from trial authors. For continuous outcomes, when studies report effect estimates using different measurement instruments that capture a common construct (eg, pain), we will first transform all outcomes to a common instrument score.30
We will use change scores from baseline to the end of follow-up to account for interpatient variability. If change scores are not reported, we will calculate them using the baseline and end-of-study scores and the associated SDs using a correlation coefficient derived from the largest trial at the lowest RoB that reported a change score. We will use DerSimonian-Laird random-effects models for meta-analysis of all direct comparisons. For all direct comparisons, when there are at least 10 trials contributing to a meta-analysis, we will assess small study effects using Harbord’s test for binary outcomes and Egger’s test for continuous outcomes.31
We will perform NMA using a frequentist random-effects model applying the methodology of multivariable meta-analysis.32 33 We will use the ‘design-by-treatment’ model (global test) to assess the coherence assumption for each network.32 We will use the side splitting method to evaluate local (loop-specific) incoherence34 35 in each closed loop of the network as the difference between direct and indirect evidence. If we find significant incoherence in the network, we will perform NMA using an inconsistency model. We will explore the network for the source(s) of incoherence and further expand or exclude the node(s) introducing incoherence into the network.
When networks are sparse, random-effects models may generate noncredible wide CIs for the network estimates even when the direct and indirect estimates are coherent (ie, the CI of the network estimate is wider than both the estimates of precision associated with the direct and indirect effect estimates).36 We will use a fixed-effect model for pooling in such cases. We will not perform NMA when 10 or fewer studies report an outcome.
We will co-present the minimally important difference (MID) for all pooled effect estimates for continuous outcomes to optimise interpretability. The MID is the smallest change in an outcome that patients perceive as important.37 We will identify anchor-based MIDs for all continuous outcome measures pooled in our analysis. In cases in which more than one MID is identified, we will evaluate their credibility using the instrument by Devji T et al and select the most credible estimate.38 39
We will use the network estimate of treatment effects to calculate the risk difference (RD) for achieving the MID. Specifically, for each individual study, we will assume that the SDs of outcome measurements are the same in both the treatment and control groups, and that change scores in both groups are normally distributed. We will use the median or mean, and SD of the control group, with the established MID for the outcome in question to estimate the probability of achieving ≥MID in the control group. We will use the pooled mean difference to estimate the mean in the treatment group and calculate the probability of achieving ≥MID in the treatment group. Finally, we will use risks in both groups to acquire the RD for achieving ≥MID. To generate measures of absolute effective (RD) for binary outcomes, we will use estimates of baseline risk from the control arm of eligible trials.
NMAs typically estimate ranking probabilities among competing therapies using the surface under the cumulative ranking curve (SUCRA), mean ranks and rankograms. An intervention with an SUCRA value of 100 is considered the most effective, whereas an intervention with 0 is the least effective.40 However, SUCRA values are mostly dependent on the point estimate of effect and ignore the associated precision and certainty of evidence. Thus, we will apply a minimally-contextualised approach41 42 to convey the relative effectiveness of available interventional pain procedures. Specifically, for each outcome, we will place interventions in categories from best to worst based on the treatment effect estimates for benefits and harms obtained from NMA, and their associated certainty of evidence.
For categorisation of interventions, we will use the following approach. For each effectiveness outcome, we will create groups of interventions as follows: (1) The reference intervention (placebo/sham procedure) and interventions no different from placebo, which we refer to as ‘among the least effective’; (2) Interventions superior to placebo but not superior to other intervention(s), which we describe as ‘inferior to the most effective, but superior to the least effective’ (category 2 interventions) and (3) Interventions that prove superior to at least one category 2 intervention (which we define as ‘among the most effective’). We will use the same approach for adverse events but will create groups of interventions as follows: (1) no more harmful than placebo; (2) less harmful than some alternatives, but more harmful than placebo and (3) among the most harmful. For both benefits and harms, we will then categorise interventions as those with moderate or high certainty, and those with low or very low certainty of evidence relative to placebo.43
We will use STATA V.16.0 (StataCorp) for all analyses. All comparisons will be two tailed using a threshold p≤0.05.
Subgroup analysis
We will use the Q statistic and I2 to explore statistical heterogeneity for direct meta-analysis, and five a priori hypotheses to explain heterogeneity between trials: (1) different clinical conditions (eg, neuropathic, nociceptive, nociplastic pain, as defined by the International Association for the Study of Pain44 will show different treatment effects; (2) studies at higher RoB will show larger treatment effects; (3) shorter follow-up will show larger treatment effects than longer follow-up times; (4) patients receiving disability benefits or engaged in litigation will show smaller treatment effects45 and (5) using a positive response on diagnostic screening as an entry criteria for participants vs not will be associate with larger treatment effects. We will perform subgroup analyses regardless of heterogeneity estimates if there are at least two trials in each subgroup.
Assessing certainty of the evidence
We will use the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach to assess the certainty of the direct, indirect and the network estimate for all outcomes. The starting point for certainty of evidence for randomised trials is high, and the direct evidence can be rated down for: RoB, inconsistency, indirectness or small study effects.46 Certainty ratings of indirect estimates start at the lowest GRADE rating of the direct comparisons that contributed to the most-dominant first order loop with further rating down for intransitivity when present.47 48 We will assess the imprecision at the network level. If incoherence is present, we will rate down the certainty of the network estimates. The certainty of evidence for network estimate will be informed by the higher rating of the direct and indirect evidence.47 We will categorise certainty in evidence as high, moderate, low or very low.
Patient and public involvement
No patients were involved in the development of this protocol. However, patient partners will be included in the accompanying BMJ Rapid Recommendation which will provide contextualised clinical guidance based on this evidence synthesis.
Discussion
Interventional pain procedures are increasingly used to manage chronic non-cancer spinal pain. In Ontario, Canada, physician billings for interventional procedures more than doubled from 2011 to 201549; however, this is a controversial treatment.50 Many jurisdictions, including Canada,51 have no standards for interventional procedure training and practice. A 2016/2017 survey of Canadian physicians practicing pain medicine found that only 37% of respondents believed that their colleagues provided interventional procedures in accordance with the best current evidence.52 Moreover, current guidelines for interventional procedures provide conflicting recommendations.12 13 16 As such, there is an urgent need for a high-quality review to summarise the evidence for the effectiveness and harms associated with interventional procedures for chronic spinal pain.
Our study will have several strengths in relation to existing reviews. First, we will explore the comparative effectiveness of all currently available interventional procedures for patients with chronic, non-cancer, axial or radicular, spinal pain. Second, rather than restricting by condition, we will investigate whether the effects of treatment vary across neuropathic, nociceptive and nociplastic pain. Third, we will use the GRADE approach to evaluate the certainty of evidence supporting treatment effects and use state-of-the-art methodology to summarise the relative effectiveness of competing interventions. A potential limitation will be the nature of available treatment comparisons to build robust networks for analyses. The findings of our review will help inform patients with chronic non-cancer spinal pain about the role of interventional pain procedures, and identify key areas for research. This systematic review will also inform a BMJ Rapid Recommendations—a collaborative effort from the MAGIC Evidence Ecosystem Foundation (www.magicevidence.org) and BMJ—that will provide contextualised clinical guidance based on this body of evidence.
Ethics and dissemination
No research ethics approval is required for this systematic review, as no confidential patient data will be used. We will disseminate our findings through publication in a peer-reviewed journal and conference presentations, and our review will support development of an international clinical practice guideline.
Ethics statements
Acknowledgments
We would like to thank Dena Zeraatkar, Yaad Shergill, Devyani Bakshi, Ngai Chow, Taha Elghamudi, Brian Vinh, and Iva Okaj for technical assistance.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @ivand_florez, @laxsanaa, @JasonWBusse
Contributors XW, GM, BS, AJD, RJC, IDF, HNC, EK, YC, MAE, LS, FM, NKS, PR, RZM, DNB, GHG, YRR, CJS, TA and JWB made substantial contributions to conception and design of the protocol. XW, GM and BS drafted the manuscript and JWB, YRR, RJC, AJD, CJS and TA revised it critically for important intellectual content. XW, GM, BS, AJD, RJC, IDF, HNC, EK, YC, MAE, LS, FM, NKS, PR, RZM, DNB, GHG, YRR, CJS, TA and JWB provided final approval of the version to be published. JWB is the guarantor of the review protocol.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests DNB and CJS declare intellectual and financial conflicts of interest, as pain physicians that perform interventional procedures for chronic spinal complaints as part of their practices. BS and TA are member of the GRADE Working Group.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.