Article Text

Abstract
Objective To describe the adherence to quality of care indicators in early rheumatoid arthritis (RA) and to evaluate its impact on the risk of hospitalisation in a real-world setting.
Design Retrospective cohort study.
Setting Patients with early-onset RA identified from healthcare regional administrative databases by means of a validated algorithm between 2006 and 2012 in the Lombardy region (Italy).
Participants The study cohort included 14 203 early-onset RA (71% female, mean age 60 years).
Outcome measures For each patient, a summary adherence score was calculated starting from the compliance to six quality indicators: (1–2) methotrexate or sulfasalazine or leflunomide with/without glucocorticoids, (3–4) other disease-modifying antirheumatic drugs (DMARDs) with/without glucocorticoids, (5) early interruption of glucocorticoids, (6) early clinical assessment.
The relationship between low, intermediate and high categories of the summary score and the 12-month risk of hospitalisation for all causes and for RA was assessed.
Results During a follow-up of 1 year, 2609 hospitalisations occurred, of which 704 were for RA (main or secondary diagnosis) and 252 primarily for RA. In a 7-year period (2006–2012), early DMARDs and timely clinical monitoring treatment increased (from 52% to 62% p trend <0.001 and from 25% to 30% p trend 0.009, respectively).
Intermediate and high summary adherence score categories (compared with the low category) were related significantly with a lower risk of hospitalisation (adjusted HR 0.85 (95% CI 0.77 to 0.93), p<0.001 and HR 0.76 (95% CI 0.69 to 0.84), p<0.001, respectively). Among the indicators of the adherence score, early DMARD prescription showed the strongest positive impact, while long-term use of glucocorticoids was the worst negative one.
Conclusion In early RA, adherence to quality standards of care is associated with a lower risk of hospitalisation. Future interventions to improve the adherence to quality standards of care in this setting should decrease the risk of hospitalisation with a significant impact on individual and population health.
- quality in health care
- public health
- rheumatology
- protocols & guidelines
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This is a population-based study including an unselected large longitudinal cohort of patients with rheumatoid arthritis (RA).
This is the first study developing a regression coefficient-based composite scoring system to measure healthcare quality in early RA.
The robustness of the results was explored with different sensitivity analyses.
The lack of detailed clinical and lifestyle variables is an intrinsic limitation of administrative healthcare data in epidemiological studies.
Introduction
Early diagnosis and treatment of rheumatoid arthritis (RA) have extensively shown a strong potential of improvement of the disease outcome. Established evidence supports the impact of early interventions in terms of early disease activity control, leading to a lower rate of radiographic progression and development of disability.1–4 A recent analysis further reinforces the relevance of early intervention as one of the most important factors to prevent the occurrence of refractory RA.5 Early diagnosis and treatment are also associated with better outcomes in terms of survival, which is mainly dependent on early suppression of disease activity and prevention of functional impairment.6–8 Therefore, the model of care including early diagnosis, prompt access to disease-modifying antirheumatic drugs (DMARDs) and early assessment of response in a treat-to-target management strategy is consistently regarded as a standard of care according to current international RA guidelines.9 The actual translation of this model into everyday clinical practice relies on efficiency of the healthcare systems in integrating clinical pathways, to ensure a continuum of care from early diagnosis, treatment and monitoring.
Despite such strength of evidence and widespread consensus, the actual application of quality standard into the real-life context is not fully accomplished. Being able to measure evidence-based healthcare quality indicators (HCQIs) is advocated to evaluate the performance of healthcare systems and to assess the actual outcome of healthcare models at population level. Several scientific efforts focused on the development of a set of HCQIs to be applied at different care levels, using different sources of information.10–14
When analysed at population level, quality of care is often suboptimal even in efficient healthcare systems, due to delay in referral and diagnosis and low rates of DMARD initiation within the first 6 months from symptom onset.15 Moreover, the real advantages for healthcare systems of implementing the reference clinical pathway of the early management of RA (eg, adhering to sequence quality of care indicators) are not yet fully established. Some data support that the adherence to HCQI may generate cost savings. A recent analysis, using administrative claims in the USA, showed that individual fulfilment of quality standards of treatment and monitoring of disease activity and DMARD toxicity is associated with lower hospital costs.16 Non-adherence to DMARDs in early RA was investigated as an HCQI with potential impact on healthcare systems. A Dutch study analysed data from about 200 patients with early RA, showing that suboptimal drug adherence is associated with higher overall costs, with a +10% expenditure due to hospitalisation.17
Beyond cost savings, the improvement of quality of care is expected to positively impact on other relevant outcomes, such as better pain control, function and participation, limiting adverse events. Hospitalisation for RA in the early course of the disease is a key outcome measure that combines effectiveness and safety of management strategies, and it is a negative prognostic factor for long-term mortality.18
Thus, we conducted an analysis in early RA real-world population to assess the temporal trend of the adherence to the HCQIs and the impact of this adherence on the risk of hospitalisations. For this purpose we took advantage of an ongoing study promoted by the Italian Society for Rheumatology, aiming to set up a national surveillance system to monitor the health burden of rheumatic diseases in Italy.
Patients and methods
Study design and setting
This is a retrospective cohort study performed using data of the Record Linkage of Rheumatic Disease (RECORD) study (promoted by the Italian Society for Rheumatology),19–24 an observational study aimed both to measure prevalence, incidence and mortality of RA and to implement an algorithm which can identify patients with RA using administrative healthcare database (AHD) information.
The data sources for the RECORD study were the AHD of Lombardy, an Italian region with more than 10 000 000 inhabitants (about 16% of the Italian population). The entire Italian population is covered by the National Health Service (NHS), and in Lombardy, an automated system of AHD has been created to collect a variety of information.25
The system of AHD included: (1) an archive of residents who receive NHS assistance (the whole resident population), reporting demographic data; (2) an archive of all hospital discharge forms (HDFs) from public or private hospitals including information on primary and secondary diagnoses and procedures coded according to the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) and Disease-Related Group (24); (3) a database providing information on outpatient NHS-refundable drug delivery, coded according to the Anatomical Therapeutic Chemical (ATC) classification system; (4) an archive containing all the certifications of chronic diseases for the exemption from copayment; (5) an archive of outpatient services (eg, diagnostic test, consultations). Subject-specific data contained in these databases are linked using a single anonymised identification code.
The ICD-9-CM and ATC codes used in the present study are reported in the online supplemental material S1.
Supplemental material
Participants
The target population in RECORD study included all Lombardy residents, aged 18 years and older, who were beneficiaries of the NHS between 2004 and 2013. For the present study, we selected from the RECORD data only patients with RA onset between January 2006 and June 2012 in order to ensure 6 months for the indicator assessment and 12 months of follow-up.
The included patients accumulated person-years of follow-up starting from the cohort entry (ie, RA onset) until the earliest date among outcome onset, death, lost to follow-up or end of follow-up period (18 months after the cohort entry). In the main analysis, patients with death or hospitalisation during the first 6 months of follow-up were excluded to ensure the evaluation of all the indicators of the first 6 months of the care process.
To identify patients with RA, a validated algorithm developed in the RECORD study was applied.21 We applied the first two steps of the algorithm to ensure 85% of sensitivity and 96% of specificity (online supplemental material S2). The RA onset was identified considering the first access to NHS for drug treatment with DMARDs or glucocorticoids (GCs), certified RA or hospitalisation for RA. Finally, to avoid further potential misclassification of patients with RA, we excluded subjects without any exposure to RA drugs or monitoring during follow-up.
To identify incident RA cases, a washout period of 2 years without pharmacological treatment for RA and without hospitalisation for RA before the inclusion in the cohort was considered; so only patients with RA onset after December 2005 were included.
Exposure
For each patient, the main exposure was defined by a summary adherence score based on the compliance (evaluated as 0 or 1) to six quality indicators for early management of RA. These indicators were proposed by the European League Against Rheumatism (EULAR) and adapted in this study to become measurable from data available in AHD.9 The quality indicators concerned the pharmacological treatment with DMARDs (particularly methotrexate (MTX), or leflunomide (LEF) or sulfasalazine (SLZ) for patients with contraindication to MTX or early intolerance) and/or concomitant use of GC (for less than 6 months) and the clinical and laboratory assessments. More specifically, the six quality indicators identified and measurable were: (A) timely exposure to MTX or LEF or SLZ but not to GCs; (B) timely exposure to MTX or LEF or SLZ in association with GCs; (C) timely exposure to other DMARDs but not to GCs; (D) timely exposure to other DMARDs concomitant with GCs; (E) early interruption of GC treatment; (F) monitoring of C-reactive protein (CRP) or erythrocyte sedimentation rate (ESR) and rheumatological consultation within 3 months from the RA onset.
Early treatment with DMARDs was defined as an exposure to at least within 1 month after the RA diagnosis. Early interruption of GCs was defined as drug discontinuation within 6 months from treatment start.
Outcomes
During follow-up, three hierarchical outcomes (with increasing specificity) were considered: (1) hospital admission for all non-surgical ICD-9 in HDF, (2) hospital admission with RA as main or secondary diagnosis (ICD-9-CM: 714.0), (3) hospital admission with RA as main diagnosis. Separately for each outcome, the date of the first hospitalisation during follow-up was considered as the date of outcome onset.
The study design is shown in figure 1.

Study design. DMARD, disease-modifying antirheumatic drug; GCs, glucocorticoids; RA, rheumatoid arthritis.
Covariates
To characterise the clinical profile of patients, health data from AHD related to the 2-year period before RA onset were considered. Data from HDFs were used to derive the Charlson Comorbidity Index (CCI),26 dichotomised in two classes (CCI=0 and CCI>0), and the drug prescription database to calculate a polypharmacy indicator, that is, the number of different drug classes (three digits of ATC) delivered to the patients (discrete variable).27
Statistical methods
Continuous variables were reported as mean (±SD) or as median (IQR) for non-normally distributed data. Categorical variables were reported as absolute and relative frequencies. For each adherence indicator the annual proportion of compliant patients was reported (from 2006 to 2012). A logistic regression model (with calendar year as covariate) was applied to test the statistical significance of trend over the entire period for each adherence indicator.
For each patient a summary adherence score was calculated. To estimate the adherence score combining the selected indicators, the approach suggested by Mehta et al28 was followed. In brief, for each outcome a Cox proportional hazards regression model was fitted including compliance to each quality indicator and the following covariates: age, gender, CCI and number of different drug classes. Weights were assigned to each adherence indicator using a scoring system and then summed to obtain a single score. A weight system has made it possible to identify which items have a greater impact on the outcome of interest without entrusting them with a score deriving from only subjective experience but guided by data. To ensure robustness to the weights system, a thousand bootstrap samples were extracted from the original sample and, for each of them, the Cox proportional hazards regression model was fitted. The final bootstrap estimates of beta coefficients related to the six quality indicators were changed in sign (in order to attribute an increment of risk to covariates with negative sign), multiplied by 10 and rounded to the nearest integer to obtain the weights. In this way, we obtained three weight sets, one for each outcome. In order to select the final weight set we considered the following approach in two steps. First step: each patient was classified into one of the three adherence score categories (low, medium and high) for each weight set, whose cut-offs were identified to ensure a balanced number of events and to identify clinically meaningful differences across groups. More specifically, for each weight set, the highest category corresponds to exposure to DMARDs alone or in combination with GCs for a short period, while the lowest one comprises only exposure to GCs for a long period.
Second step: the Kaplan-Meier curves for each outcome were estimated using the three adherence score categories set as exposure. The adherence score categories set which ensured at the same time greater discrimination for all outcomes was selected. To test the discriminatory capacity of the model, the Harrell’s C-index was calculated.
Finally, to evaluate the relationship between the adherence score categories selected and each outcome adjusted for potential residual confounding due to categorisation, we fitted (for each outcome) a multivariate Cox proportional hazards regression model including the same covariates of the model for weight definition. The proportional hazards hypothesis was formally tested by the Schoenfeld’s residual test.29
To verify the validity of the associations between indicators and hospitalisation in patients with RA, two negative control outcomes—a priori unrelated to the disease—were assessed: hospitalisation for urinary tract infections (ICD-9-CM: 5990) and for acute posthaemorrhagic anaemia (ICD-9-CM: 2851).
AHD collected information about all contacts with NHS of all patients was included in the study, thus no missing data were expected.
All hypothesis tests were two sided and p values for statistical significance were set at 0.05. All the analyses were performed using R statistical software V.3.3 (Foundation for Statistical Computing, Vienna, Austria).
Patient and public involvement
No patient was involved.
Results
A total of 48 277 potential RA cases were identified between 2004 and 2013 applying the algorithm to data of RECORD project. Excluding prevalent cases, a total of 17 332 patients with incident RA were included; 2705 subjects were excluded due to hospitalisation or death during the first 6 months after the RA-onset date. Finally, 424 patients were excluded because they were not treated or monitored during the period of observation. The final cohort included 14 203 patients (see online supplemental material S3).
The subjects were predominantly women (71%) (decreasing during time with a trend p value 0.006) with a mean age of 60 years (±14.1); the proportion of patients with CCI greater than 0 was 12% (decreasing during time with a trend p value <0.001); the median of drug classes prescribed was 4 (2–6). All patients’ characteristics are reported in table 1. A total of 2609 subjects (18.4%) were hospitalised for all non-surgical ICD-9 in HDF diagnosis during follow-up. Seven hundred and four patients (5%) were hospitalised for RA, 252 of whom were reporting RA as main diagnosis.
Description of the study cohort at baseline and during follow-up (n=14 203)
Temporal trend of adherence indicators
Starting treatment with DMARDs during the first month after diagnosis increased to 10% (from 52% in 2006 to 62% in 2012) with a significant trend over the entire period (p value trend <0.001). More specifically, statistically significant increment included: (1) MTX or SLZ or LEF in association with GCs (from 11% to 17%; p value trend <0.001); (2) other DMARDs in association with GCs without early interruption (from 8% to 12%; p value trend <0.001); (3) GCs without early DMARDs and no early interruption (from 19% to 25%; p value trend <0.001). Figure 2 shows the temporal trend of drug treatments in patients with RA. It has also observed a significant decrement of: (1) GC monotherapy with early interruption (from 27% to 12%; p value trend <0.001); (2) MTX or SLZ or LEF without GCs (from 14% to 12%; p value trend 0.003).

Temporal trend (from 2006 to 2012) of RA drug treatment. P values derived from logistic regression models with year of diagnosis as covariate and quality indicator adherence as outcome. DMARD, disease-modifying antirheumatic drug; GCs, glucocorticoids; LEF, leflunomide; MTX, methotrexate; RA, rheumatoid arthritis; SLZ, sulfasalazine.
The proportion of subjects with timely CRP or ESR and a specialist visit assessment significantly increased (from 25% to 30%; p value 0.009).
Adherence score
The better weight set was the one identified using hospitalisation for RA as outcome, which produced a summary adherence score ranging from −4 to 4 (table 2). The summary adherence score is categorised into three groups: low adherence (adherence score from −4 to −2; 36%), intermediate adherence (from −1 to 0; 36%) and high adherence (from 1 to 4; 28%).
Adherence score development
Nineteen (25.3%) subjects belonging to the low adherence group died during the follow-up: 34 (45.3%) in the intermediate group and 22 (29.3%) in the high adherence group, respectively.
Distribution of each outcome for adherence score categories is reported in online supplemental material S4.
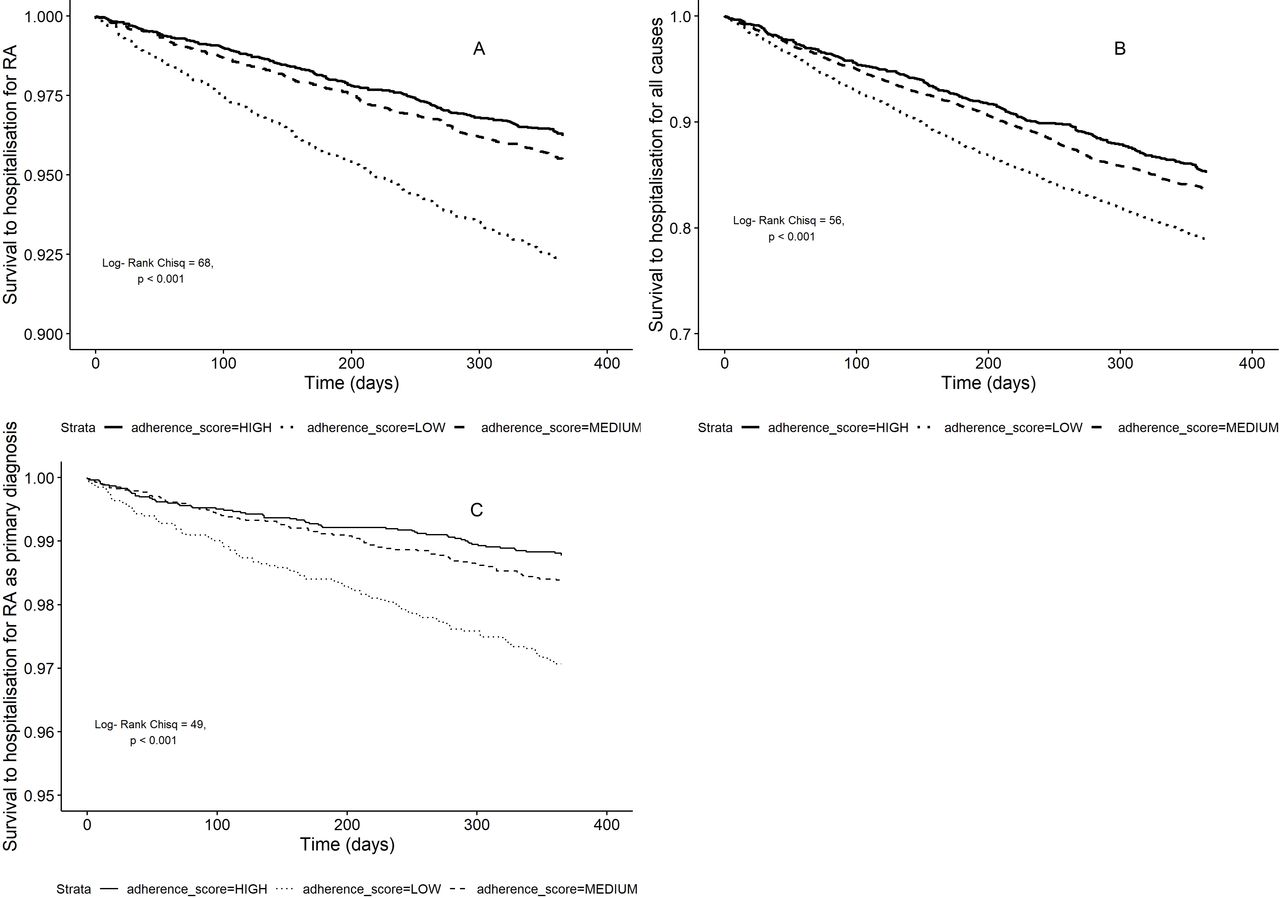
The impact of adherence score categories on the risk of each outcome is shown by means of Kaplan-Meier curves reported in figure 3.

{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier survival curves according to categories of adherence score and risk of hospitalisation. (A) Unadjusted Cox regression model with hospitalisation for RA as outcome. (B) Unadjusted Cox regression model with hospitalisation for medical causes as outcome. (C) Unadjusted Cox regression model with hospitalisation for RA as primary diagnosis as outcome. RA, rheumatoid arthritis.
Low adherence group was associated with a significantly higher probability of hospitalisation than the other two groups for all outcomes (log-rank test p<0.001). The effect of adherence score estimated by Kaplan-Meier curves was confirmed by the multivariate Cox regression model analysis. Taking into account the low adherence group as reference category, the intermediate adherence category was associated with an HR between 0.85 and 0.54 (p<0.001) and high adherence group was associated with an HR between 0.76 and 0.41 (p<0.001), for hospitalisation for all causes and hospitalisation for RA (main diagnosis), respectively (table 3).
Results of Cox regression models
The curves related to Cox regression models with hospitalisation for urinary tract infections and acute posthaemorrhagic anaemia are reported in online supplemental material S5. A substantial robustness of main findings was confirmed by the negative control analyses since the Kaplan-Meier curves did not show any differences in the risk among summary adherence score categories (log-rank test p value 0.07 and 0.12 for posthaemorrhagic anaemia and urinary tract infections, respectively).
Discussion
Despite the great progresses made in the last decades in the understanding of the pathogenetic mechanisms of RA, in the development of new targeted therapies and effective intervention strategies, the translation of this knowledge in everyday clinical practice is not yet complete. The diagnosis and treatment of RA at onset represent a paradigmatic example in which an integrated clinical pathway would be able to modify the course of the disease, to improve patient outcome and consequent cost saving.
We investigated the actual application of selected standards of care of early RA care process through six measurable HCQIs at the level of the general population afferent to NHS and correlated these process indicators with effectiveness and safety outcomes, relevant for the health system. The main results of our analysis have shown that the adherence of the individual care pathway to HCQIs is associated with a decrease in the risk of hospitalisation for RA, with a reduction up to 40% in the case of patients with the highest adherence in a 6-month period. These real-world data reflect at system level what has already been established in clinical studies on limited and selected subjects.16 17 The choice of hospitalisation as the main outcome measure is linked to its relevance both for the individual health and for its impact on the healthcare system.18 Furthermore, early hospitalisation (within the first 2 years from RA onset) is a measure of failure of the RA care pathway and represents one of the most important mortality risk factors after age and persistent disease activity.20 This result is consistent with other studies that have correlated quality indicators with system outcome measures, in particular with costs.17 30–32 A recent population-based analysis measured a set of quality indicators of the pharmacological management of RA, correlating the adherence to HCQIs with health expenditure.16 This study analysed separately eight indicators (one of which was related to the ESR and CRP monitoring at 3 months in the newly diagnosed RA), finding an increase in drug-related expenditures in the groups of patients who met the indicator, along with a reduction in the cost of hospital services. This study suggested the sustainability of the implementation of treatment standards at the population level. In our study, we focused on a limited set of indicators of the early phase of the disease management, which is the setting in which it is more likely to be able to redirect the long-term course of the disease, according to the paradigm of the window of opportunity.33
Our study included a cohort of patients in which a series of indicators could be measured, making possible to construct a composite adherence quality score, potentially useful for monitoring quality of care, perform comparative evaluations across healthcare providers and develop performance-driven incentivisation by the NHS. Analysing the relative weights of the different indicators, we found a preponderant positive effect of early DMARD treatment—that is, started within a month from the diagnosis—in reducing the risk of hospitalisation for RA. This risk reduction was independent of other features, including age and comorbidities, and other potential competing events such as death and very early hospitalisations. The measurement of the indicators in the first 6 months after the diagnosis and the measurement of the outcomes in the following year could have inflated the association between performance and events due to the immortal time bias. However, even the sensitivity analysis that includes early hospitalisation confirmed the main analysis. The further sensitivity analysis that included hospitalisations for causes a priori unrelated to RA supported that the relationship between quality of care and hospitalisation for RA is not confounded by an intrinsic higher risk of hospitalisation in subjects having a lower adherence to the standards of care.
GC therapy had a positive impact only if combined with a DMARD and if prescribed for a period of less than 6 months, as recommended by the EULAR guidelines.9 This finding is also in line with the long-term evidence derived from the Combinatietherapie bij Reumatoide Artritis (COBRA) study, where treatment strategy included high doses of GCs at onset, demonstrating the absence of excess mortality compared with the general population after 23 years.34
On the other hand, short-term monitoring of acute phase reactants and specialist consultation did not relate with the risk of hospitalisation. Another study assessed the influence of ESR or CRP monitoring within 3 months by the diagnosis on healthcare expenditures.18 Brady et al16 found lower costs associated to inpatient services in patients with acute phase reactant monitoring. A possible explanation of this discrepancy might rely on the stringency of our indicators. Many services are not able to warrant a short-term follow-up to all their patients, especially where an early arthritis clinic is not established. For this reason, short-term follow-up could be reserved to more severe patients, with an intrinsically higher risk of hospitalisation, which could be not adequately controlled by the applied adjustment variables (residual confounding).
Analysing the trend of the actual implementation of adherence to treatment standards, we recorded significant variations over time. An increase of about 10% was observed in timely treatment with DMARDs, which represents the major determinant of a favourable outcome. However, a still high proportion of patients did not start any DMARD treatment within the first 6 months of follow-up, indicating a huge gap to fill to translate recommendations into practice. Short-term steroid therapy has also progressively increased, indicating a progressive spread of treatment guidelines in clinical practice. Nevertheless, a still relevant and increasing proportion of patients were exposed to chronic GCs.
Even though AHD is a useful data source for analyses of healthcare service utilisation at population level, providing full completeness of follow-up data, they have some intrinsic limitations. The identification of patients with RA is subjected to misclassification, which may have included patients with self-limiting RA-like diseases, who did not develop a chronic disease. The inclusion of these patients has been limited in the data set using an algorithm with more than 95% of specificity and excluding patients with no relevant healthcare service utilisation. The results relating to the weights assigned to the individual adherence indicators have not been validated externally and their generalisability is not guaranteed. However, the choice of the model derived from two criteria: (1) identifying potential variables through a multidisciplinary activity with clinical experts and based on European guidelines, and (2) correcting for the variables available in the administrative databases. The selection procedure identified a model with a fair discriminatory capacity, measured by the Harrell’s C-index (0.63).
The use of an algorithm of identification of RA including treatments for RA may inflate the adherence to the treatment quality indicators. However, the therapeutic criterion classifies patients with RA in about 10% of cases, and was mainly used to identify the first RA-related event rather than a diagnosis. As a result, the overall adherence to treatments is lower than expected in our cohort. AHD does not directly allow for assessment of patient clinical status, including disease activity and severity of RA. As a result, strict monitoring could be reserved to patients with higher disease activity and severity, masking the positive effect of HCQIs. Patients with more severe disease could be more frequently treated with DMARDs or GCs, underestimating the beneficial effect of DMARDs and the detrimental effects of GCs when administered alone. Conversely, patients exposed to DMARDs early could have lower contraindications to these drugs (eg, comorbidities). Adjusting the estimates for AHD-derived comorbidity indexes and drug exposure would have limited this potential confounding, and the lag time between exposure and outcome attribution would have limited the association between the delay in treatment start and concurrent medical conditions. In some cases, such as chronic obstructive pulmonary disease, chronic GC treatment for other indication than RA might have inflated the risk of hospitalisation. However, even restricting the analyses on hospitalisation for RA, no significant changes were observed.
In conclusion, we provided one of the first evidence of the association between adherence to the quality of care of early RA and the risk of hospitalisation. Overall performance levels are still suboptimal and indicate the need for further health policy interventions aimed at improving access to care both in the diagnostic phase and in the strict monitoring of effectiveness in the early phases of RA. Thus, these results reinforce the need of promoting healthcare models, such as early arthritis clinics to improve early access to disease-modifying treatments in RA and strict clinical monitoring to ameliorate the treatment experience, and limit the use of health resources, leveraging on the improvement of the quality of care.
The next steps of our research will focus on the sustainability of an early and intensive treatment implemented by setting up an early arthritis clinic comparing long-term cost savings with early healthcare investment.
References
Footnotes
Contributors AZan, CAS, AZam and GC contributed to the conception and design of the work and the acquisition of data. AZan, CAS and AZam contributed to the analysis of data and all the authors critically interpreted and analysed on the results. AZan, CAS, LA and AZam wrote the draft of the manuscript and all the authors approved the final version.
Funding The study was supported by the Italian Society for Rheumatology.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study was approved by the Ethical Committee of the Pavia University Hospital and has been performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data may be obtained from a third party and are not publicly available. Data were granted from the General Directorate of Health of the Lombardy Region for the objectives of this project and are not usable for other purposes. R codes of the analyses are available upon request.