Article Text

Abstract
Objective Creating an appropriate antithrombotic therapy for patients with atrial fibrillation (AF) who have undergone percutaneous coronary intervention (PCI) remains a dilemma. Several clinical trials compared the use of a dual antithrombotic therapy (DAT) regimen with a direct oral anticoagulants including (apixaban, dabigatran, edoxaban or rivaroxaban) and a P2Y12 inhibitor versus a triple antithrombotic therapy (TAT) that includes a vitamin K antagonist plus aspirin and a P2Y12 inhibitor in patients with AF who have undergone PCI. However, there are no head-to-head trials comparing the DAT regimens to each other. We aimed to compare the efficacy and safety of DAT regimens using a network meta-analysis (NMA) approach.
Design A systematic review and NMA of randomised clinical trials.
Methods We conducted a systematic literature review to identify relevant randomised clinical trials and performed a Bayesian NMA for International Society on Thrombosis and Haemostasis (ISTH) major or clinically relevant non-major (CRNM) bleeding, all-cause mortality, stroke, myocardial infarction (MI) and stent thrombosis outcomes. We used NetMetaXL V.1.6.1 and WinBUGS V.1.4.3 for the NMA and estimated the probability of ranking the treatments based on the surface under the cumulative ranking curve.
Results The comparison between DAT regimens showed no significant difference in the safety or efficacy outcomes. Apixaban regimen was ranked first as the preferred therapy in terms of ISTH major or CRNM bleeding and stroke, with a probability of 52% and 54%, respectively. Rivaroxaban regimen was the preferred therapy in terms of MI and stent thrombosis, with a probability of 34% and 27%, respectively. Dabigatran regimen was ranked first in terms of all-cause mortality, with a probability of 28%.
Conclusion The DAT regimens are as safe and effective as TAT regimens. However, ranking probabilities for the best option in the selected outcomes can be used to guide the selection among these agents based on different patients’ conditions.
- anticoagulation
- myocardial infarction
- coronary heart disease
- thromboembolism
- bleeding disorders & coagulopathies
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- anticoagulation
- myocardial infarction
- coronary heart disease
- thromboembolism
- bleeding disorders & coagulopathies
Strengths and limitations of this study
The used network meta-analysis technique facilitated the comparison of dual antithrombotic therapy regimens versus triple antithrombotic therapy regimen in patients with atrial fibrillation who have undergone percutaneous coronary intervention.
Only randomised clinical trials were included in this network meta-analysis.
All the included studies were of high quality with a low risk of bias.
The results were associated with wide CIs, which might affect the precision of the findings.
Introduction
Atrial fibrillation (AF) is a common comorbidity in patients with acute coronary syndrome (ACS) due to similar risk factors. The incidence rate of AF in patients with ACS ranges from 5% to 23%.1–5 Appropriate antithrombotic therapy for patients with AF who had ACS or have undergone percutaneous coronary intervention (PCI) is controversial. In patients with AF, oral anticoagulation is recommended for the prevention of cardioembolic stroke,6 but its efficacy in preventing stent thrombosis for patients who have undergone PCI is not well established.
Dual antiplatelet therapy (DAPT), with aspirin plus a P2Y12 inhibitor, is recommended in patients with ACS for secondary prevention of ischaemic events and stent thrombosis.7 Triple therapy, including an oral anticoagulant (OAC) on top of the DAPT, was recommended by previous guidelines and considered a standard of care for patients with AF who experienced ACS or underwent PCI.7 8 However, the most recent American Heart Association/American College of Cardiology/Heart Rhythm Society (AHA/ACC/HRS) 2019 guidelines suggested the use of dual antithrombotic therapy (DAT) (vitamin K antagonist (VKA) or a direct oral anticoagulant (DOAC) plus a P2Y12 inhibitor) over the triple antithrombotic therapy (TAT) (OAC, aspirin and a P2Y12 inhibitor),6 due to the increased risk of bleeding with the triple therapy that was reported in multiple studies.9–14
In an attempt to clarify this controversy, six randomised control trials (WOEST, ISAR-TRIPLE, PIONEER AF-PCI, RE-DUAL PCI, AUGUSTUS and ENTRUST AF-PCI) were conducted to assess the efficacy and safety of the TAT compared with the DAT for patients with AF receiving oral anticoagulation after experiencing ACS or undergoing PCI.9–14 Although these trials reported a higher incidence of major bleeding in patients receiving the TAT compared with the DAT without significant differences in the risk of ischaemic events, it is noteworthy to recognise that these trials were underpowered to detect ischaemic events.
Several observational studies found a higher risk of bleeding with the triple therapy that involved VKA, aspirin and a P2Y12 inhibitor.15–17 The objective of this network meta-analysis (NMA) is to assess the safety and efficacy of a DAT regimen with a DOAC versus a TAT regimen with a VKA in patients with AF who experienced ACS or underwent PCI.
Methods
A systemic literature search was conducted using Medline and Embase through October 2019 to identify randomised clinical trials that evaluated the use of DOACs in patients with AF who experienced ACS or underwent PCI. The search terms included percutaneous coronary intervention, PCI, atrial fibrillation, acute coronary syndrome, ACS, stent, anticoagulants, rivaroxaban, edoxaban, apixaban, dabigatran, DOACs, vitamin K antagonist, VKA, warfarin, aspirin, clopidogrel, triple therapy, double therapy, dual antithrombotic therapy, DAT, triple antithrombotic therapy and TAT. We also searched for other systematic reviews and meta-analyses and reviewed their references to identify any relevant studies. The search was limited to studies that were published in English within the last 10 years.
For each study, episodes of major or clinically relevant non-major (CRNM) bleeding events based on the International Society on Thrombosis and Haemostasis (ISTH) definition,18 all-cause mortality, stroke, myocardial infarction (MI), stent thrombosis were extracted (see online supplemental table 1). Data were extracted from the published studies and assessed for eligibility by two independent investigators (RMA and RAA) and verified by a third investigator (OAA). The risk of bias assessment was conducted for each study using the Cochrane Collaboration risk of bias assessment tool.19 A Bayesian NMA, a statistical method that can incorporate both direct and indirect comparisons including treatment arms that were not previously compared in head-to-head trials from a clinical trial, was conducted for the pre-specified outcomes using NetMetaXL V.1.6.1 (Canadian Agency for Drugs and Technologies in Health, Ottawa, Canada)20 and WinBUGS V.1.4.3 (MRC Biostatistics Unit, Cambridge, UK). We used the random effect binomial model with vague priors and employed Markov chain Monte Carlo simulation for 60 000 iterations after discarding 30 000 iterations as burn-in simulations initially. Estimates of the outcomes were presented in OR and 95% credible intervals. Also, we estimated the probability of ranking the treatments based on the surface under the cumulative ranking curve.21 We reported this NMA according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses for NMA.22
Supplemental material
Patient and public involvement
Patients and the public were not involved in the design or conduct of the study.
Results
A total of 662 articles were identified in the systematic search. Four studies, PIONEER AF-PCI, RE-DUAL PCI, AUGUSTUS and ENTRUST AF-PCI, met the inclusion criteria and were included in the current NMA.11–14 The flowchart in figure 1 illustrates the process of including and excluding articles for this NMA. The risk of bias assessment of the included trials showed low risk of bias (see online supplemental table 2).
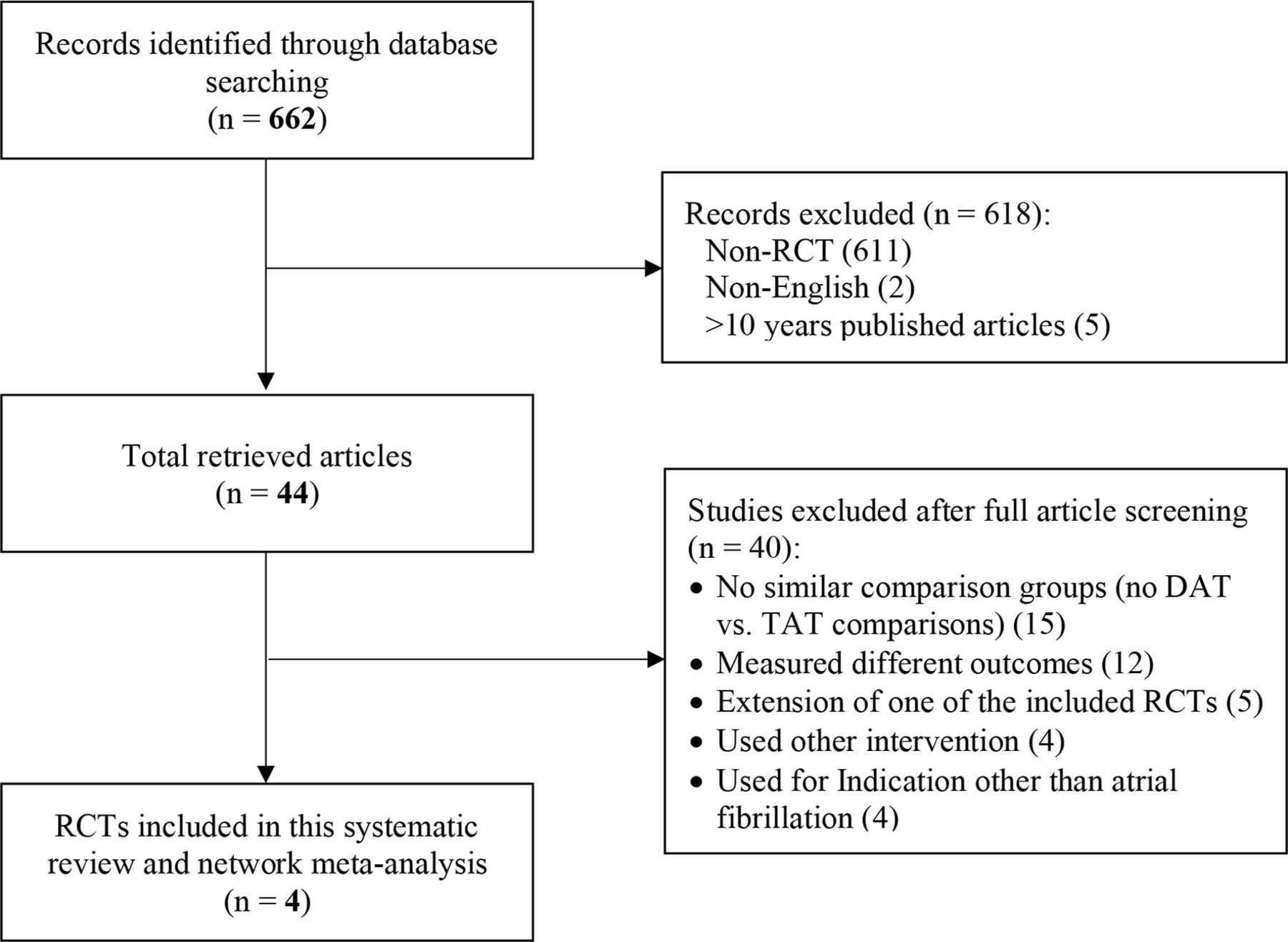
Flow diagram for studies included in the network meta-analysis. DAT, dual antithrombotic therapy; RCTs, randomised controlled trials; TAT, triple antithrombotic therapy.
Summary of the included trials
The trials that were included demonstrated favourable results for the pre-specified outcomes towards DOACs when mainly used in a DAT regimen in combination with a P2Y12 inhibitor only.11–14 The PIONEER AF-PCI trial was conducted to compare the safety and efficacy of using DOACs agent in a DAT regimen to TAT regimen. A DAT regimen including low-dose rivaroxaban (15 mg once per day) in combination with a P2Y12 inhibitor (group 1) was compared with a TAT regimen that included a P2Y12 inhibitor and aspirin in combination with either a very low-dose rivaroxaban (2.5 mg two times per day; group 2) or VKA (group 3). The study found the bleeding rates were significantly reduced for groups 1 and 2 compared with group 3 (16.8%, 18.0% and 26.7%, respectively; HR for group 1 vs 3=0.59; 95% CI 0.47–0.76; HR for group 2 vs 3=0.63; 95% CI 0.50–0.80). However, the rivaroxaban dose that was used in the trial is lower than the recommended daily dose for stroke prevention in AF (20 mg), and the very low dose was not included in the NMA.11
The RE-DUAL PCI Study was conducted to compare the safety and efficacy of using dabigatran (110 or 150 mg two times per day) in a DAT regimen with a P2Y12 inhibitor to a TAT regimen that included a P2Y12 inhibitor and aspirin in combination with a VKA. The findings of the study demonstrated a significantly lower risk of bleeding for the DAT regimen that included dabigatran to the TAT regimen (HR=0.52; 95% CI 0.42–0.63; p<0.001 for superiority).12 However, it is to be noted that both studies, the PIONEER AF-PCI and RE-DUAL PCI, were not powered to detect any significant disparities in efficacy between the DOACs and VKA.
The AUGUSTUS trial compared the use of apixaban to a VKA along with clopidogrel and aspirin to a placebo using a 2×2 factorial design. The study concluded that a DAT regimen with apixaban and clopidogrel only was both non-inferior and superior to a TAT regimen in terms of reducing the risk of major or CRNM bleeding (HR=0.69; 95% CI 0.58–0.81; p<0.001 for both non-inferiority and superiority), while there was no difference in the ischaemic event outcomes.13
The most recent ENTRUST AF-PCI trial was designed to assess a DAT regimen, that included edoxaban plus a P2Y12 inhibitor, to a TAT regimen, that included a VKA plus a P2Y12 inhibitor and aspirin. Similar to the previous trials, they found a lower rate of bleeding in the DAT regimen in comparison to the TAT regimen (HR=0.83, 95% CI 0.65–1.05; p=0·0010 for non-inferiority). However, unlike other DOACs, the trial found the edoxaban regimen to be non-inferior, but not superior to the TAT regimen.14
Network meta-analysis
Demographic characteristics
A total of 7890 patients were included in the NMA. The mean age for the included patients ranged between 68 and 71 years, and about 22%–30% of participants were women. The detailed patients’ demographics and outcomes from the included studies were presented in table 1.
Patients’ demographics and outcomes from the included randomised controlled trials
ISTH major or CRNM bleeding
There were no significant differences between all DOACs when used in DAT regimens as well as when compared with TAT regimen, using VKA. Among all, DAT regimen containing apixaban was the preferred one, with a probability of 52%, followed by regimens containing dabigatran or rivaroxaban, with a probability of 18% and 17.9%, respectively (figure 2).

The network meta-analysis and the rankogram results for the International Society on Thrombosis and Haemostasis major or clinically relevant non-major bleeding. Estimates are presented in OR and 95% credible intervals. LD, low dose; P2Y12i, P2Y12 inhibitor; VKA, vitamin K antagonist.
All-cause mortality
The NMA showed no differences between all DAT regimens containing DOACs as well as between DAT and TAT regimens in regard to all-cause mortality. However, the ranking of DAT regimens showed that dabigatran regimen was the preferred agent, followed by apixaban regimen and rivaroxaban regimen with a probability of 28%, 21.5% and 20.8%, respectively (figure 3A, online supplemental figure 1).

The network meta-analysis results for (A) all-cause mortality and (B) stroke. Estimates are presented in OR and 95% credible intervals. LD, low dose; P2Y12i, P2Y12 inhibitor; VKA, vitamin K antagonist.
Stroke
Similar to all-cause mortality, the results of the NMA showed no significant difference between the DOACs when used in DAT regimen, and when compared with the TAT regimen, with VKA. Apixaban DAT regimen was ranked first, followed by regimens of edoxaban and rivaroxaban with a probability of 54%, 19.5% and 12.4%, respectively (figure 3B, online supplemental figure 2).
Myocardial infarction
There were no significant differences between all DOACs in the DAT regimens compared with each other or to the TAT regimen, with VKA. Rivaroxaban DAT regimen was the preferred regimen, followed by apixaban regimen and edoxaban regimen, with a probability of 34%, 22% and 18%, respectively (figure 4A, online supplemental figure 3).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
The network meta-analysis results for (A) myocardial infarction, and (B) stent thrombosis. Estimates are presented in OR and 95% credible intervals. LD, low dose; P2Y12i, P2Y12 inhibitor; VKA, vitamin K antagonist.
Stent thrombosis
The odds of stent thrombosis were similar across all DAT regimens with DOACs and TAT regimen, with rivaroxaban DAT regimen being the preferred regimen with a probability of 27% and followed by edoxaban regimen with a probability of 23% (figure 4B, online supplemental figure 4).
Discussion
For patients with AF who experienced ACS or underwent PCI, the selection of a regimen that is both effective in preventing stroke and stent thrombosis while minimising the risk of bleeding remains a challenge for prescribers. The main focus of this NMA was to estimate the efficacy and safety of different DOACs in DAT regimens compared with each other and to VKA in a TAT regimen for patients with AF who had undergone PCI, and to rank the DOACs in terms of difference in the efficacy and safety outcomes. We looked at five main end points, which were ISTH major or CRNM bleeding, all-cause mortality, stroke, MI and stent thrombosis.
Our results showed no significant difference between a DAT regimen with a DOAC compared with a TAT regimen with a VKA for all the specified outcomes. This demonstrates that the DAT regimen with DOACs is just as safe and effective as the TAT regimen with a VKA. However, apixaban regimen was the preferred option in reducing the risk of major or CRNM bleeding and stroke, dabigatran regimen was ranked as first option in the reduction of all-cause mortality, and rivaroxaban regimen was preferred in terms of reducing the risk of MI and stent thrombosis. Based on this ranking, VKA was ranked the lowest in comparison to all DOACs’ DAT regimens in terms of bleeding, all-cause mortality and MI. A previous NMA by Lopes et al presented similar results, but in their NMA, there was a significant difference between the DAT and the TAT regimens with a more favourable outcome in terms of safety for the regimen that includes a DOAC and a P2Y12 inhibitor.23
The 2016 European Society of Cardiology guidelines for the management of AF recommended to initiate the patients’ management on the triple therapy that includes an OAC with aspirin and clopidogrel in the 1st month of treatment after PCI, or to an extended period of 6 months in case of lower risk of bleeding; then, to continue with a dual therapy (OAC plus aspirin or clopidogrel) for 6–12 months and lifetime therapy on an OAC.8 Only aspirin and clopidogrel were recommended as antiplatelet therapy as opposed to third generation P2Y12 inhibitors due to the increased risk of bleeding and lack of evidence. If a DOAC is chosen for anticoagulation, then the lowest effective dose for stroke prevention should be used. However, a regimen of low-dose rivaroxaban plus clopidogrel and aspirin is not recommended for stroke prevention in AF.8 In the recent AHA/ACC/HRS 2019 guidelines for the management of AF in patients who had undergone PCI, the guidelines favoured the DAT over the TAT; for patients with an increased risk of stroke based on their CHA2DS2-VASc who should be initiated on triple therapy (OAC plus P2Y12 inhibitor plus aspirin), it is recommended to transition them to double therapy at the 4th–6th week of treatment.6 However, no recommendations were made in such population regarding the use of apixaban and edoxaban due to the lack of data on these agents at that time.
The results of this NMA align with the findings of previous studies that demonstrate the sufficiency of the DAT regimen for the prevention of stroke in patients with AF who experienced ACS or underwent PCI, with the added benefit of having a reduced risk of bleeding in those patients.9–14 There are some limitations to this NMA. The prominent variation in the design, the length of follow-up period and sample sizes between the included trials could have possibly contributed to the wide CI and the lack of significance in our analysis. Therefore, the findings should be used with caution until a large direct comparison studies among DOACs are conducted or findings from retrospective studies become available to support this evidence. Perhaps future studies could look more into patient-specific outcomes that could be based on differences in terms of sex, age group, presence of other comorbidities, genetic variations and other P2Y12 inhibitors.
Conclusion
The DAT regimens with DOACs are as safe and effective as the TAT regimen with VKA. Moreover, DOACs in DAT regimens had higher ranking probabilities as a best option in the selected outcomes over VKA in a TAT regimen. These ranking probabilities can be used to guide the selection among different DOACs agents based on patients’ conditions, until evidence from large and direct comparison studies become available.
Acknowledgments
The authors would like to extend their appreciation to King Saud University for funding this work through the Researcher Supporting Project (RSP-2020/77), King Saud University, Riyadh, Saudi Arabia.
References
Footnotes
Twitter @Dr_Almohammed
Contributors MSAY, MYA and ARA designed the study, conducted the analysis, produced the tables and figures, and participated in writing the manuscript. SMAR and AMA conducted the literature review, summarised the included trials and prepared the resulting figure. RMA and RAA extracted the data and contributed to writing the manuscript. OAA and OMA reviewed the extracted data for the analysis and the tables for the results and contributed to writing the manuscript. All authors read and approved the final manuscript.
Funding This work was supported by the Researcher Supporting Project number (RSP-2020/77), King Saud University, Riyadh, Saudi Arabia.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplemental information.