Article Text

Abstract
Objectives Cultural differences between the USA and France led us to examine the feasibility, acceptability and preliminary efficacy data on craving, quality of life and psychological flexibility of the add-on Mindfulness-Based Relapse Prevention (MBRP) programme in alcohol use disorder (AUD) in France.
Design We conducted a prospective observational study with a 6-month follow-up.
Setting The study was performed in a naturalistic setting with adult outpatients from an addiction department.
Participants We included all patients with a current AUD who participated in the MBRP programme (n=52). There was no non-inclusion criterion.
Interventions The intervention was an 8-week MBRP programme, combining elements of traditional relapse prevention cognitive behavioural therapy and mindfulness meditation training. This was an eight-session closed-group programme.
Primary and secondary outcome measures Primary outcomes were the number of attended treatment sessions, home practice frequency and dropout rate. Secondary outcomes were changes in craving, quality of life, psychological flexibility, drinking outcomes, depression, anxiety and mindfulness levels.
Results The average number of completed sessions was 6.6 (SD: 1.9). Most participants introduced mindfulness meditation into their everyday lives: 69% and 49% of included patients maintained formal practice at 3 and 6 months, respectively, and 80% and 64% maintained informal practice at 3 and 6 months, respectively. Most participants used mindfulness techniques to face high-risk situations (56% at 6 months). Participants reported a significant reduction in craving, days of alcohol use, depression and anxiety and an increase in mindfulness and psychological flexibility at 6 months.
Conclusions The MBRP programme showed good acceptability and feasibility. MBRP seemed to improve craving, mindfulness and psychological flexibility. Comparative studies are needed to evaluate the programme’s efficacy in AUD.
Trial registration number 2200863 v 0.
- mindfulness
- alcohol use disorder acceptability
- relapse prevention
- MBRP
- craving
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This study was conducted in a naturalistic ecological setting to provide a clinically relevant view of the feasibility and acceptability of a mindfulness-based relapse prevention programme for alcohol use disorder.
We collected preliminary efficacy data on drinking and non-drinking outcomes such as craving, psychological flexibility and quality of life.
There was no control condition.
The sample size and missing data led to weakened statistical power.
Introduction
Alcohol use disorder (AUD) contributes significantly to the global burden of diseases and is marked by relapse.1–3 Cognitive behavioural therapies (CBTs) assume that patients have irrational thoughts that contribute to the maintenance of the problem behaviour. CBTs aim to modify the cognitive and behavioural processes that maintain the disorder by leading patients to question their irrational thoughts, replacing them with rational thoughts and thus not generating the ‘problem behaviour’. In a more behavioural approach, patients are repeatedly exposed to the situations that usually lead to the problem behaviour and are offered the opportunity to recognise that the corresponding thought was irrational. There is evidence supporting the efficacy of CBTs in the treatment of addictions.4 However, some patients are resistant to CBTs and its effectiveness decreases in the long term.4 The limits of CBTs can be explained by the presence of underlying processes linked to self-control, such as persistent suppressive coping strategies. Emotional suppression, or the tendency to respond to negative emotional states with alcohol consumption, is common in patients with AUD5 and can lead to automated behaviours which are difficult to inhibit. Paradoxically, the attempt to suppress negative emotions promotes their emergence.6 Complementary strategies to promote acceptance of emotional states could be useful to overcome such automatic reactions.7–9 This could explain why, despite adequate care, craving often persists,10 11 which has been identified as an important predictor of relapse in addictions.12 Specific addictive processes could be the target of complementary interventions to CBTs for relapse prevention: psychological functioning (indirectly) and craving (directly).
Mindfulness
Mindfulness has been defined by Jon Kabat-Zinn as an ‘awareness that arises through paying attention, on purpose, in the present moment, non-judgementally’.13 Mindfulness involves being aware of the present experience, including inner and external events, in a non-reactive way and without judgement.14 Mindfulness practice is increasingly being introduced in clinical therapies.15 16 Some programmes combine conventional CBT elements and mindfulness training, such as the Mindfulness-Based Stress Reduction programme16 and Mindfulness-Based Cognitive Therapy.17 These mindfulness-based therapies showed promising results in the treatment of psychiatric disorders such as depression and anxiety.18 19 Unlike conventional CBTs, mindfulness-based therapies do not aim to change thoughts or emotions, but to change one’s relationship to them. In other words, rather than modifying mental activity to avoid the emergence of a behaviour, mindfulness involves taking a step aside and observing mental production, without judgement and without the need to react automatically to it. This ability could enhance self-control and covers a wide range of applications, regardless of the situation or the cognition. Experiential avoidance is a coping style with the objective of avoiding or suppressing private experience such as emotions and cognitions.20 Patients with substance use disorder (SUD) seem to commonly use this avoidant coping style,21 which has been shown to be associated with the severity of SUD and craving.22 From this perspective, substance use expectancies could be the suppression of a negative inner experience.22 However, efforts to suppress emotion and thoughts could paradoxically increase their intrusion.23 Learning how to accept and not react to uncomfortable internal events could improve the management of negative emotions and thus be particularly useful in the treatment of SUD.
Bowen et al 24 developed a programme specifically for use in relapse prevention in patients with SUD. The Mindfulness-Based Relapse Prevention (MBRP) programme integrates mindfulness training and CBT components inspired from Marlatt’s manual to prevent relapse.25 In the 8-week MBRP programme, patients are invited to generate a craving sensation by visualising a trigger situation and dealing with discomfort related to craving through meditative techniques, that is, observation, experiencing and acceptance without reacting. These techniques aim to improve tolerance to discomfort.
Mindfulness meditation is less widespread in France than it is in the USA. Mindfulness is a mind–body approach: Mind, body and spirit are three interconnected concepts.26 Yet, spirituality has a very different imprint in different countries. According to the Temperament and Character Inventory,27 the ‘self-transcendence’ dimension, which reflects levels of spirituality, is higher in the USA than in France.28 This could explain the differences in the dissemination of mindfulness between France and the USA. It could also lead to limits on the transferability of American results to other countries with lower levels of spirituality, such as France. These results show that it is essential to assess the acceptability of this type of intervention according to the cultural contexts in which it is provided. However, studies in the cancer field showed that a new dimension of nature-oriented spirituality, different from religiosity, is emerging in European countries as well and could be an operating coping style. This new dimension could be perceived as being close to the concept of mindfulness, as one of the questions in a Swedish study explored whether walking or engaging ‘in any activity outdoors gives you a spiritual sense’.29 Patients with SUD seem to have a significantly lower level of trait mindfulness in comparison to that of healthy controls.30 Mindfulness-based interventions have shown promising results in the treatment of addiction in the USA.31 The MBRP programme has shown efficacy in comparison to treatment as usual, based on the Alcoholics/Narcotics Anonymous 12 steps programme, with group meetings one to two times a week32 and a conventional CBT relapse prevention programme in SUD in the USA (n=286).33 However, patients received compensation for completing the questionnaires and a participation bonus. It appears that compensation makes participation more attractive for economically disadvantaged people. Therefore, compensation can have an impact on the clinical representativeness of the sample.34 Furthermore, as remuneration makes participation in the study more attractive, it can have an impact on the information given by the patient about the selection criteria in order to avoid exclusion from the study35 but also on the retention rate, and affect the acceptability assessment.
Only one study has been conducted in France in AUD,36 showing improvements in mindfulness levels, impulsivity and anxiety after the MBRP programme, but with no control group (n=26). No information on the feasibility or acceptability of the programme was available, and therefore additional data on these aspects of mindfulness-based interventions in AUD in France are needed.
In the present study, we aimed to assess the feasibility and acceptability of the MBRP programme in AUD in an ecological setting. We also aimed to report the preliminary efficacy data of this programme, with a special focus on non-drinking outcomes, particularly craving, mindfulness levels, psychological flexibility and quality of life. Non-drinking outcomes are clinically relevant and complementary to consumption criteria, particularly in the context of the recent expansion of therapeutic objectives in AUD to include drinking reduction alongside abstinence.37 Person-centred approaches imply very different drinking-objectives depending on the patient. It was noted that variables that do not directly measure consumption could be a more representative indicator of the effectiveness of treatment for patients and healthcare providers, including quality of life.38–40 In addition, factors such as depressive disorders, anxiety and craving are known to have an influence on relapse,41–43 and their measurement therefore seems relevant in this context. Mindfulness could lead to the development of psychological resources such as psychological flexibility and mindfulness levels. Psychological flexibility has been described as the ability to fully live in the present moment, including the thoughts and emotions it contains, without trying to change it, and, according to the situation, persisting or changing behaviour in the pursuit of objectives.44 Psychological flexibility is considered the opposite of experiential avoidance: the tendency to try to change the frequency or intensity of internal negative events such as cognitions, emotions or sensations, which appears to be associated with substance and alcohol craving.22 Increasing the level of psychological flexibility could be particularly beneficial for addictions, as it increases the ability to accept negative emotions or other unpleasant sensations, such as craving, and moves the patient away from the dysfunctional avoidant coping style. The parallel assessment of these resources and drinking outcomes could allow a better understanding of the underlying mechanisms of action of mindfulness-based strategies in AUD and to what extent the direct impact of mindfulness training on resources such as mindfulness levels or psychological flexibility, could have an indirect impact on alcohol consumption, through the use of more adaptive and non-suppressive coping strategies. Moreover, quality of life has been identified as an important variable in assessing treatment outcomes in patients with AUD from their perspective45–47 and appears to be a good predictor for treatment success.37 Our hypothesis was that the MBRP programme could significantly reduce craving and improve mindfulness levels, psychological flexibility and quality of life in AUD by comparing significance of change from baseline to 3 months and 6 months, in a naturalistic clinical setting. Moreover, we hypothesise that this group will demonstrate good feasibility with good participation in the sessions and good acceptability with implementation of home practice and a low dropout rate.
Methods
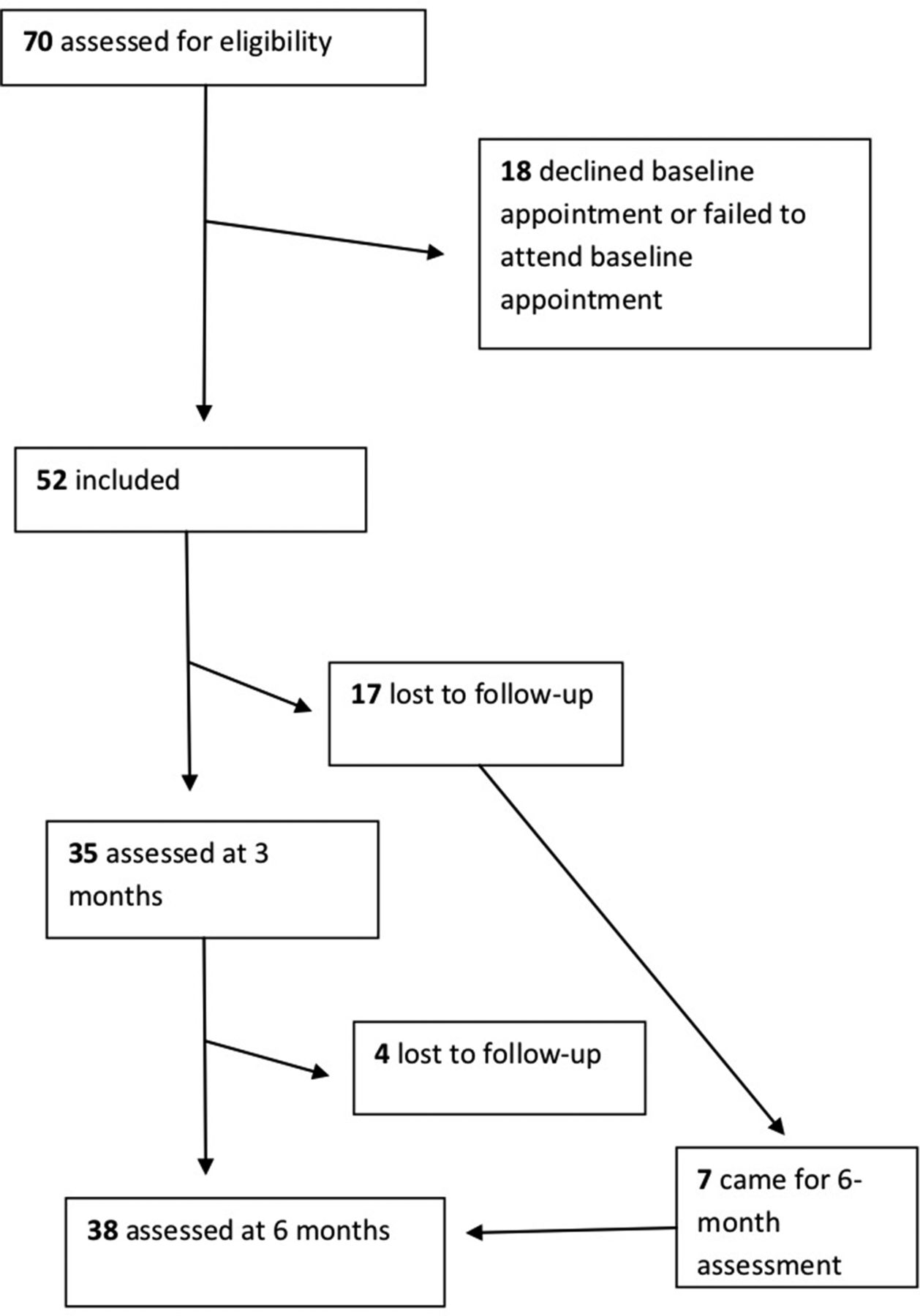
We conducted a prospective ecological observational study without a control condition to assess the feasibility, acceptability and benefits of an MBRP programme as a treatment for AUD (see figure 1).

Flowchart
Study population
Participants were recruited in the addiction facility of the Paul Brousse Hospital of Villejuif (France). We included all patients with a current AUD who participated in the MBRP programme. There was no non-inclusion criterion. Patients were informed and agreed that the data, part of the medical register, could be used for research.
Ethics
For this observational non-interventional study, we followed reference methodology M-003. The MR-003 is the legal framework for routine care research in France. It implies that patients did not object to participate after having been individually informed. In accordance with the legislation, all patients of the facility were systematically informed that their medical data could be used for research purposes. All patients agreed orally to have their data used for research. This observational study using collected in routine data could not be preregistered. However, hypotheses were stated before the statistical analysis. We sent a notice to all included patients containing information about the present study and reminding them of their right of refusal to have their data used for this research. No patient has withdrawn his agreement after receiving this notice. This study was declared to and authorised by the French national committee for informatics and liberty ‘CNIL’.
MBRP programme
The mindfulness-based intervention followed the MBRP programme designed by Bowen and colleagues.24 It was an 8-week group programme with one 2-hour session per week, specific to addiction but non-specific to any substance or behaviour. It combined mindfulness meditation exercises with components from Marlatt’s relapse prevention CBT programme.48 The main objectives of this programme were to increase the level of mindfulness and to teach the patient not to react automatically to cravings. The first three sessions of the programme targeted awareness and presence. The first session focused on the autopilot mode and relapse, the second focused on awareness of triggers and craving, and the third promoted mindfulness in daily life. Sessions ‘four’, ‘five’ and ‘six’ targeted mindfulness and relapse prevention. Specifically, the objective of the fourth session was to foster mindfulness in high-risk situations, the fifth session was to teach acceptance and skilful action, and the sixth session was to learn to consider thoughts as thoughts only, not as reflections of reality. The purpose of the last two sessions was to extend what was learnt to daily life, through work on self-care, lifestyle balance, social support and continuing practice. At each session, the exercises were selected to be easily used in autonomous settings, such as the Stop/Observe/Breathe/Expand awareness/Respond mindfully exercise, a short 3 min exercise that aims to manage high-risk situations by inhibiting automatic behavioural responses.24
Measures
At baseline, 3 months and 6 months, we collected data from the medical register by using the following measures:
The Alcohol Time Line Follow Back (TLFB)49 is a drinking assessment method that obtains estimates of daily drinking. It has been evaluated with clinical and non-clinical populations. People provide retrospective estimates of their daily drinking by using a calendar over a specified time period, in this case 1 month from the interview date. Memory aids can be used to improve recall (eg, calendar; key dates serve as anchors for reporting drinking; standard drink conversion). The Alcohol TLFB has good psychometric characteristics with different drinker groups. This method is used when precise estimates of drinking are necessary.
The Alcohol Quality of Life Scale (AQoLS)50 is a 34-item patient-reported outcome that measures health-related quality of life specific to patients with an AUD, developed from the patient’s perspective. The AQoLs shows good internal consistency (Cronbach’s alpha: 0.96).
The Craving Experience Questionnaire (Frequency) (CEQ-F)51 is a self-assessment tool that evaluates the frequency of cravings over the last week. It is divided into three more dimensions that evaluate the intensity (CEQ-F intensity) and intrusiveness (CEQ-F intrusion) of craving and images (CEQ-F imagery) associated with craving. This questionnaire showed good psychometric properties among patients with AUD (Cronbach’s alpha: 0.94).
The Acceptance and Action Questionnaire (AAQ-II)52 is a 10-item self-assessment tool that reports experiential avoidance and psychological inflexibility. The French version was validated53 and psychometric properties have been documented among a clinical sample of patients with an SUD.52 This tool has good internal consistency (Cronbach’s alpha: 0.75).
The Five Facets Mindfulness Questionnaire (FFMQ)54 is a 39-item questionnaire that measures mindfulness levels on five factors: observing, describing, acting with awareness, non-judging of inner experience and non-reactivity to inner experience. The FFMQ scale was validated in AUD.55 It shows good internal consistency with a Cronbach’s alpha of 0.88 for the total score and ranging from 0.76 to 0.89 for the five factors.
The Impulsive Behaviour Scale (UPPS-P) short version56 is a 20-item self-reported scale. It assesses impulsivity in five different facets: urgency, positive urgency, lack of perseverance, lack of premeditation and sensation seeking. The short French version of the UPPS-P presented good psychometric properties in SUD with Cronbach’s alphas ranging from 0.70 to 0.84 for the five facets.57
The Beck Depression Inventory (BDI 21)58 is a 21-item self-questionnaire that assesses the presence and severity of depressive symptoms. The BDI scale also showed good psychometric properties in SUD (Cronbach’s alpha: 0.92).59
The Beck Anxiety Inventory (BAI)60 is a 21-item self-questionnaire that assesses anxiety. This tool was designed specifically for a clinical population in the field of psychiatry, and its developers paid particular attention to its ability to discriminate between anxiety and depression. The French version of this scale showed good psychometric properties (Cronbach’s alpha: 0.85).61 This inventory has been validated in a clinical sample.62
We collected sociodemographic data and other health resources to evaluate the intensity of treatment aside from the MBRP programme. We collected the frequency of the formal and informal practice of meditation after the end of the programme. Formal practice included an intentional commitment of time, for example, sitting meditations or body scans. Informal practice was defined as bringing an intentional awareness to a routine daily activity. It could take place during daily life activities, including, for instance, showering or washing dishes. We also collected data on the use of mindfulness exercises in high-risk situations.
We choose to evaluate at 3 months and not immediately after the end of the course because the majority of the evaluations we used were based on the last 4 weeks. The same applies to the drinking outcomes (TLFB). It seemed more relevant to evaluate the condition of our patients over the 4 weeks following the end of the programme rather than over the last 4 weeks of the programme. This seems all the more relevant when it comes to the evaluation of the introduction of a home practice.
Feasibility and acceptability
Simons and Kursawe63 defined feasibility as ‘the proportion of patients who were offered treatment who completed and the number of sessions attended’. We used attendance to treatment sessions as a proxy for feasibility. Turrini et al, assessed acceptability as follows: ‘the number of patients leaving the study early for any reason, were recorded as a measure of treatment acceptability’.64 Sekhon et al defined acceptability as ‘multi-faceted construct that reflects the extent to which people delivering or receiving a healthcare intervention consider it to be appropriate’ and including, ‘perceived effectiveness.’ 65 Furthermore they indicated that ‘If an intervention is considered acceptable, patients are more likely to adhere to treatment recommendations and to benefit from improved clinical outcomes.’ Thus, we used both dropout rate and home practice as proxies for acceptability, considering that implementation of home practice indicated that mindfulness had been implanted in the patient’s daily life, implying a perceived effectiveness of the method.
Statistical analyses
We performed descriptive analyses. At 3 months, data were missing for 33% of patients and at 6 months for 27% of them. We handled missing data by using a median imputation. The missing data were mainly related to missed evaluation appointments or incomplete questionnaires. We conducted Wilcoxon tests to compare the mean changes between baseline, 3 months and 6 months.66 We calculated Spearman’s rank correlation coefficient on baseline between mindfulness and craving frequency, craving triggers, anxiety, depression and quality of life. Analyses were conducted by using R V.3.3.
Patient and public involvement
The research question and outcome measures emerged from clinical observation and informal patient feedback. Patients were not directly involved in the design, recruitment or conduct of the study. Patients were informed that the collected data could be used for research purposes and had access to the results on request.
Results
Baseline characteristics
We included 52 patients between October 2016 and April 2017. Table 1 presents patients’ characteristics at baseline. Sixteen patients were abstinent, and 24 had at least one heavy drinking day (HDD) during the last 30 days. On average, patients drank 63.3 alcohol units over the last 30 days (SD=89.8). All 52 patients had regular medical appointments with an addiction specialist. Most (60%) benefited from individual psychotherapy, 8% participated in other group interventions proposed in the facility and 12% had regular appointments with a nurse from the facility. Of 52 patients, eight consumed cannabis daily and 28 used tobacco. All participants were diagnosed with AUD by a clinician when they started treatment in the addiction unit. At the time of participation in the MBRP programme they were not all at the same stage of care, but they all presented criteria for AUD in the last 12 months, and a functioning affected by AUD as judged by the clinician, even some had recently became abstinent or had recently reduced drinking. This point explains the heterogeneity in the number of HDD at baseline.
Baseline characteristics
Acceptability and feasibility of the programme
The average number of completed sessions was 6.6 (SD: 1.9). Most participants maintained mindfulness meditation in everyday life after the end of the programme. At 3 months, 69% of participants maintained formal practice and 80% maintained informal practice. At 6 months, 49% of participants maintained formal practice and 64% maintained informal practice. Most participants also used mindfulness techniques learnt in the programme to face high-risk situations (57% at 3 months and 56% at 6 months). At 6 months, 27% of patients were dropouts, we thus note that 73% of the participants remained in the study until 6 months after the programme.
Baseline correlations between mindfulness level and drinking and non-drinking outcomes
We showed a significant negative correlation between mindfulness level and all three drinking outcomes, namely, number of HDDs, number of days of consumption and total alcohol consumption in the last month (r=−0.3,–0.2 and −0.3, respectively, and p=0.005, 0.009 and 0.006, respectively). Correlation analyses showed a significant negative correlation between the level of mindfulness and the impact of alcohol on quality of life (r=−0.3, p=0.001): The higher the mindfulness level, the lower the negative impact of alcohol on quality of life. A positive correlation between home practice and the level of mindfulness (r=0.2, p=0.009) could also be identified. Furthermore, we found a significant negative association between mindfulness level and anxiety (r=−0.3, p=0.001), depression (r=−0.5, p<0.001) and frequency of craving in the last week (r=−0.1, p=0.03).
Preliminary efficacy data
The evolution of drinking characteristics, mindfulness, craving, anxiety and depression are reported in table 2.
Evolution of drinking characteristics, mindfulness, craving, anxiety and depression
Drinking outcomes
We found a significant reduction in the number of HDDs from baseline to 3 months (p=0.025). Significance was not reached at 6 months. We also found a significant reduction in the number of drinking days at 6 months (p=0.002). However, we could not find any difference in total alcohol consumption.
Psychological flexibility, mindfulness and quality of life
We found a significant reduction in the impact of alcohol use on quality of life (AQoLS) at 3 months (p=0.048). Significance was not reached at 6 months. We also noted a significant increase in the total mindfulness level from baseline to 3 months (p=0.019) and to 6 months (p<0.001) (FFMQ). We found significant changes in the following factors of mindfulness at 3 and 6 months: observation (3 months: p=0.003; 6 months: p=0.011), description (3 months: p=0.007; 6 months: p<0.001) and non-reactivity (3 months p=<0.001; 6 months: p<0.001).
We also observed an increase in psychological flexibility and acceptance (AAQ-II) at 6 months (p<0.001).
Craving
We found a significant reduction in the frequency of intense cravings over the last week at 3 months (p=0.019) and in the total score and all three dimensions of craving frequency in the last week at 6 months: total score (p=0.001), intensity (p=0.002), intrusion (p=0.010) and imagery (p=0.002) (see figure 2).

{kind=link}
{kind=link}
Evolution of craving frequency subscales. CEQ-F, Craving Experience Questionnaire (frequency over the last week).
Anxiety and depression
We found a significant reduction of depression scores (BDI) at 6 months (p<0.001) and a significant reduction of anxiety (BAI) at 3 months (p=0.028) and 6 months (p=0.036).
Within group effect size
At 3 months we found medium effect sizes for the number of HDD, the total alcohol consumption, anxiety and mindfulness and small effect sizes for the number of days of alcohol use, quality of life, depression, psychological flexibility and craving frequency. At 6 months effect sizes were large for depression, mindfulness, craving frequency and psychological flexibility (see table 2).
Discussion
This study presents feasibility and acceptability data and first benefits of drinking and non-drinking outcomes of the MBRP programme in patients with an AUD in care in a naturalistic clinical setting at 3 and 6 months. We found that most participants introduced mindfulness meditation into everyday life and most used mindfulness techniques to face high-risk situations. We showed a significant reduction in depression and an increase in mindfulness levels and psychological flexibility at 6 months. At 3 and 6 months, we found a reduction in anxiety. We showed a significant reduction in the number of HDDs and the impact of alcohol use on quality of life at 3 months and of craving frequency at 6 months. We also found interesting negative correlations between mindfulness and the impact of alcohol use on quality of life, craving frequency, anxiety and depression.
From the perspective of offering a relapse prevention strategy, we chose a naturalistic recruitment with no non-inclusion criteria, and patients had at baseline a wide range of drinking characteristics. This is an ecological study and participants did not receive any compensation or remuneration for participating in the programme, which offers a complementary perspective to that allowed by previous studies, particularly clinical trials that used poor ecological environments.33 67 We also focused on non-drinking outcomes, which allowed us to assess the evolution of patients, regardless of their drinking goals and baseline drinking status.37 Documenting a broad panel of non-drinking outcomes allowed us to evaluate the patient as a whole, including his or her own subjectivity.
Craving
We found a significant reduction in the frequency of intense craving over the past week at 6 months. This result could suggest that mindfulness training could have a direct action on craving and could reduce craving intensity. However, it should be noted that no causal link could be drawn through this observational study. This result is consistent with existing studies documenting the positive impact of mindfulness on craving.68 Resisting craving could be seen as trying to suppress it. Suppressive strategies seem to be efficacious in anxious patients in addiction.69 However, emotion suppression is well known as a dysfunctional coping style.6 Some authors suggested that reducing maladaptive coping such as suppression could be a priority for the treatment of several mental conditions. Thus, the efficacy of suppressive strategies has been debated in addiction.70 Neuroimaging studies showed that craving and resisting craving often activates the same brain networks.9 Trying to resist the urge could then lead to an extension of craving intensity.71 Similarly, trying to suppress a thought makes one think of that thought, which is precisely why it makes it impossible to remove.23 Another option to be set free from a thought or emotion is to accept it.23 Mindfulness is a non-suppressive strategy. The MBRP programme focused particularly on craving, more precisely, on the acceptance of craving. The main objective of this programme was to teach participants to accept the discomfort of craving and to realise that with or without consumption, craving tended to decrease. One of the key elements of the MBRP programme was the repeated imaginational exposure to craving in order to make participants realise that they do not necessarily have to react automatically to the associated discomfort, eventually by drinking. This could lead to a habituation process that could explain the reduction of intense craving frequency in this study.
Psychological flexibility and mindfulness
These results are consistent with improvement in psychological flexibility (AAQ-II), which revealed a better ability to accept inner experience, such as emotion, instead of trying to suppress it. Moreover, mindfulness-based therapies are classified as state training interventions.72 73 State training aims to develop a brain state by practising through mindfulness meditation, which could influence the functioning of self-control networks, which then fosters executive functions including inhibitory control.72 74 In contrast to CBT, mindfulness-based interventions do not target the inhibition of one particular behaviour but lead participants to develop a brain state that enables them not to react automatically to discomfort, such as that experienced when craving. Improvements in mindfulness and psychological flexibility could allow one to hypothesise that mindfulness-based interventions have a direct action on these two psychological resources and that part of the action on craving and drinking outcomes could be indirect. More precisely, mindfulness-based interventions could modify the brain state and thereby modify the activity of brain networks. In the context of treatment for patients with AUD, improvement in the ‘non-reactivity’ dimension of mindfulness, which is the ability to allow thoughts and feelings to come and go, without getting absorbed or carried away by them, could reflect improvements in self-control.
Quality of life
We found a significant change in quality of life at 3 months. These results did not, however, remain significant at 6 months. Mindfulness training also appeared to have beneficial effects on quality of life in other research fields in the past.75–77 Our mitigated results could be because the impact of alcohol on the quality of life of our sample was already relatively low at baseline (23 of 102), which mechanically reduces the margin for change.
Negative affect
We found a decrease in anxiety and depression and an association between mindfulness levels and anxiety and depression; these results are consistent with the scientific literature,78 which suggested that mindfulness could be negatively associated with negative mood. Several studies showed that negative mood could predict treatment outcomes in SUD and that patients with depression and anxiety could show higher rates of relapse with this disorder.5 41 79–81 Thus, fostering mindfulness levels could therefore protect participants from relapse. Furthermore, Roos and colleagues found that the MBRP programme showed a large effect on substance use outcomes among patients with severe substance use, depression and anxiety symptoms.82 Here again, mindfulness could have a direct effect on emotion regulation and an indirect effect on drinking outcomes through better emotion regulation.
Drinking outcomes
Change in HDDs was significant at 3 but not 6 months. However, change in number of drinking days was significant at 6 months. It could be hypothesised that the programme increased self-control as a direct effect of mindfulness practice, resulting in a decrease of HDD at the postintervention assessment on the third month. Change in lifestyle balance, resulting in less drinking days, could take more time and be an indirect effect of the programme, visible from the sixth month. The loss of significance of HDD at 6 months could be related to a greater dispersion of data, that is, larger SD, which could traduce a loss of efficacy on self-control in some participants may be due to a decrease in mindfulness practice over time.
Some studies revealed that mindfulness levels at baseline could predict treatment outcomes in SUD.83 Our results showed a significant correlation between mindfulness levels and drinking characteristics. The fact that mindfulness levels were negatively correlated to the impact of alcohol use on quality of life, depression, anxiety, craving frequency and drinking outcomes suggests that mindfulness could improve the overall level of psychological functioning through direct and indirect mechanisms. Further studies should be carried out to explore a causal link between these variables.
Limitations
This study has several limitations. It is an observational study with no control group; it does not allow to assess the efficacy of the programme but only to report on changes in an observational way. Comparative studies are needed to document the efficacy of this programme in AUD. We used widely used proxies to assess feasibility and acceptability, but it could have been interesting to complete these data by qualitative interviews. Furthermore, the sample size and the missing data lead to weakened statistical power that could explain why some of the demonstrated improvements could not reach significance. Another limitation related to ecological design is that all participants attended regular medical appointments and that 60% of participants also received psychotherapy. Patients were not involved in the design of the study. A mediation study is needed to understand the direct and indirect mechanisms of mindfulness-based interventions in AUD. Finally, it would have been interesting to assess spirituality in our sample as a possible marker of response. It has been shown that mindfulness trait and spirituality levels are associated and that both increased after participation in a mindfulness-based programme.84 Other results suggested that people who meditate regularly have a higher level of openness to experience than those who do not.85 It would be interesting to know if this kind of personality trait (eg, openness/spirituality) is a precondition for meditation and if these traits predict treatment adherence or outcomes
Conclusions
This ecological study offers evidence for the MBRP programme to be a feasible add-on treatment in AUD in France. Most of the patients completed the programme and used the learnt mindfulness techniques to cope with craving. Patients seemed to adhere to the programme and introduced the mindfulness practice into their lives. The MBRP in addition to standard care appeared to result in less frequent craving, increased mindfulness levels and improvements in psychological flexibility. Given that mindfulness training teaches acceptance of uncomfortable inner experiences such as craving or negative mood instead of their suppression, MBRP could reduce automatic reactions and increase self-control. These results allow us to consider that mindfulness-based interventions could work both directly and indirectly through improvement in psychological resources such as psychological flexibility and emotion regulation. A mediation study could help to clarify the direct and indirect mechanisms of action. Comparative studies are needed to investigate the efficacy of the programme
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
Footnotes
Contributors CvH and AL participated to the protocol writing, conduction of study, statistical analysis, results interpretation and manuscript writing. LR and YK participated to the protocol writing, statistical analysis, results interpretation and manuscript writing. MD, H-JA and AB participated to conduction of study, results interpretation and manuscript writing.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Disclaimer All authors have seen and approved the final version of the manuscript being submitted. They warrant that the article is the authors' original work, has not received prior publication and is not under consideration for publication elsewhere.
Competing interests H-JA has received sponsorship to attend scientific meetings, speaker honoraria and consultancy fees from Bioprojet, D&A Pharma, Ethypharm, Lundbeck, Merck-Serono, Mundipharma, Novartis and Pfizer. LR has received sponsorship to participate in scientific reaserch funded by PMU and FDJ through a convention with the University Paris Ouest Nanterre la Défense. AB has received sponsorship to attend scientific meetings, speaker honoraria and consultancy fees from Bristol-Myers-Squibb, Lundbeck, Merck-Serono and Mylan and is member of the invidor board. AL has received sponsorship to attend scientific meetings, speaker honoraria and consultancy fees from Lundbeck and Indivior.
Ethics approval This study was declared to the French national committee for informatics and liberty “CNIL” (number 2200863 v 0).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The proposed research includes data from 52 subjects. The dataset includes self-reported demographic and behavioral data from interviews and self-assessment, part of the medical register and collected in routine care. We could share disidentified data and only with the authorisation of the CNIL (National Commission for Information Technology and Rights).
Patient consent for publication Not required.