Article Text

Abstract
Objectives The primary objective was to compare the efficacy of enteral potassium replacement (EPR) and intravenous potassium replacement (IVPR) as first-line therapy. Secondary objectives included comparison of adverse effects and number of doses required to resolve the episode of hypokalaemia.
Trial design The EIPS trial is designed as a randomised, equivalence trial between two treatment arms.
Study setting The study was conducted at the paediatric cardiac intensive care unit (PCICU) at Aga Khan University Hospital, Karachi.
Participants 41 patients (aged 1 month to 15 years) who were admitted to PCICU post cardiac surgery were recruited (23 IVPR arm and 18 EPR arm).
Intervention Intervention arms were block randomised on alternate weeks for IVPR and EPR.
Outcome measure Change in serum potassium levels in (mmol/L) and percentage change after each event of potassium replacement by the intravenous or enteral route.
Results Both groups (41 patients) had similar baseline characteristics. Mean age was 4.7 (SD±4) years while the most common surgical procedure was ventricular septal defect repair (12 patients, 29.3%). No mortality was observed in either arm. Four episodes of vomiting and one arrhythmia were seen in the EPR group. After adjusting for age, potassium level at the beginning of the episode, average urine output, inotropic score and diuretic dose, it was found that there was no statistically significant difference in change in potassium levels after EPR and IVPR: 0.86 mmol/L (±0.8) and 0.82 mmol/L (±0.7) respectively (p=0.86, 95% CI −0.08 to 1.10), or percentage change in potassium level after enteral and intravenous replacement: 26% (±30) and 24% (±20) (95% CI −3.42 to 4.03, p=0.87).
Conclusion EPR may be an equally efficacious alternative first-line therapy in treating hypokalaemia after surgery in selective patients with congenital heart disease.
Ethics and dissemination This study has been approved by Ethics Review Committee at AKU.
Trial registration number NCT02015962.
- hypokalemia
- potassium replacement
- pediatric post-surgical patients
- intravenous potassium replacement
- enteral potassium replacement.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
- hypokalemia
- potassium replacement
- pediatric post-surgical patients
- intravenous potassium replacement
- enteral potassium replacement.
Strengths and limitations of this study
EIPS is the first prospective randomised equivalence trial comparing the routes (enteral vs intravenous) for potassium replacement in paediatric patients in intensive care post cardiac surgery.
A retrospective review has previously shown comparable efficacy between the two routes.
Research from this trial will lead the way for further research in this field, possibly bringing about a change in the management of hypokalaemia in patients after surgery and subsequently lower complications and morbidity associated with intravenous potassium replacement.
EIPS is not a blinded study, which may lead to a procedure bias. Blinding could not be carried out in this trial owing to different routes of administration of the same supplementation (enteral vs intravenous) and different time intervals for checking serum levels in each arm (1 hour after intravenous replacement and 2 hour after enteral replacement).
Confounding factors, such as concomitant use of diuretics and inotropic agents during the episode, were identified and adjusted in the analysis.
Introduction
Hypokalaemia is a frequently encountered electrolyte abnormality in the daily clinical practice of the paediatric cardiac intensive care unit (PCICU). In the postoperative period, activation of the renin–angiotensin–aldosterone system, enhanced sympathetic tone and use of potassium-wasting diuretics for positive fluid balance have led to increased occurrence of severe hypokalaemia and its consequences.1 Hypokalaemia is a strong independent predictor of mortality in patients with heart failure.2–4 Potassium replacement remains the cornerstone therapy for hypokalaemia. There is mounting evidence that the serum potassium level should be maintained between 3.5 and 4.5 mmol/L5 or even higher in the setting of acute cardiac injury.6 7 Thus it is highly desirable to avoid hypokalaemia by close monitoring and subsequent potassium replacement.
Although intravenous potassium replacement (IVPR) in hypokalaemia is the preferred route in most intensive care settings, it is associated with known safety risks. IVPR can lead to arrhythmias, cardiac arrest and death if administered inappropriately.2 8 9 Given these risks, IVPR is considered a ‘high-alert medication’ by the Institute of Safe Medication practice.10 11 The need to maintain and frequently access a central line for administration of higher concentrations of potassium can lead to serious central line infections. Inability to use high-concentration potassium through peripheral lines may lead to administration of a larger volume of fluid for the delivery of the desired dose of potassium, thus disturbing the fluid balance in these patients. This may be detrimental in cardiac patients after surgery in whom a negative fluid balance is optimal. Given all the above mentioned issues with IVPR, enteral potassium replacement (EPR), with its equal or superior safety profile, may be a better alternative to IVPR. A retrospective review showed that the efficacy of EPR was comparable to IVPR in paediatric patients after surgery for congenital heart disease.9
We sought to explore this comparison between EPR and IVPR in a randomised equivalence trial to determine if EPR can be used as an alternative to IVPR.
This trial was registered at ClinicalTrials.gov (registration number: NCT02015962). This manuscript describes the results of the trial. Consort checklist of the trial is also included as supplementary file. Details of the trial protocol and design have been previously published.12
Objectives
The primary objective was to compare the equivalence of efficacy (measured as change in serum potassium levels in mmol/L and percentage change in level after potassium replacement) between EPR and IVPR as first-line therapy for the treatment of hypokalaemia. The secondary objectives were to compare the adverse effects (hyperkalaemia, diarrhoea, gastrointestinal bleeds, nausea and vomiting) after EPR and IVPR; to compare the number of doses required in achieving resolution of hypokalaemia (as described per protocol) for each episode; and to determine the efficacy of EPR versus IVPR for various degrees of severity of hypokalaemia, that is, mild, moderate or severe.
We hypothesise that EPR will be equally efficacious in the treatment of hypokalaemia as IVPR, as first-line therapy.
Trial design
Trial protocol and design have been published previously.12 Briefly, the EIPS trial was designed as a randomised, non-blinded, equivalence trial with two arms. Arm A (IVPR) received intravenous potassium replacement while Arm B (EPR) received enteral potassium replacement as a treatment for hypokalaemia. Intervention arms were block randomised in alternate weeks for IVPR and EPR for the sake of convenience and to minimise error in drug delivery.
Methods
Definitions used for the study
Hypokalaemia
Hypokalaemia was defined as serum potassium <4.4 mmol/L
Event and episode of hypokalaemia
Serum potassium <4.4 mmol/L was considered as hypokalaemia. This marked the beginning of an episode of hypokalaemia. Each potassium replacement was considered an event of hypokalaemia irrespective of whether hypokalaemia was completely resolved or not. The episode of hypokalaemia ended when the potassium level returned to the normal range as described above.
Study setting
The study was conducted in the paediatric cardiac intensive care unit (PCICU) at Aga Khan University Hospital, Karachi, Pakistan.
Eligibility criteria
Inclusion criteria
This trial included patients, aged 1 month to 15 years, undergoing surgical repair/palliation of a congenital heart lesion at Aga Khan University Hospital and admitted to the PCICU for postoperative management. Patients'/parents' willingness to participate in this study, serum potassium levels <4.4 mmol/L in the postoperative period, ability to tolerate oral or nasogastric administration of medication for EPR and presence of a central line for IVPR were also included in the eligibility criteria.
Exclusion criteria
We excluded patients with acute renal failure (creatinine clearance: ecCr <75%, urine output <0.3 mL/kg/hour×16 hours).13 Patients with paralytic ileus, necrotising enterocolitis, gastrointestinal bleeding, nausea, vomiting or diarrhoea were also excluded as they could not be given EPR. However, patients were not excluded if vomiting or diarrhoea developed after initial recruitment. Patients with critically low serum potassium <2.0 mmol and patients with symptomatic hypokalaemia were not recruited.
Consent procedure
Informed consent and assent was obtained by investigators from each patient (or parents) before cardiac surgery.
Study recruitment, procedure and monitoring
A detailed description of recruitment, study procedure and monitoring has been previously published.12 Patients were enrolled and potassium levels were checked routinely once they were moved to PCICU postoperatively. When the patients developed hypokalaemia, they received treatment according to the intervention arm and were followed until they had reached optimal potassium levels or moved from PCICU to a step-down unit. Repeat serum potassium levels were checked 1 hour after replacement in the IVPR group and 2 hours after replacement in the EPR group. Further monitoring of the serum electrolytes was determined by the patient’s clinical status.
In cases when the patient stayed in PCICU for longer than 1 week and block changed, patients continued to follow the route they were originally assigned. EPR patients who developed side effects (eg, vomiting, gastrointestinal upset) or critically low levels of potassium <2 mmol (exclusion criteria) were allowed to cross over and receive IVPR. An intention to treat analysis was performed to account for crossover patients.
During the pre-recruitment trial period, it was recognised that patients who were given enteral potassium supplementation could not tolerate the enteral formulation and ended up vomiting due to the sour taste of the formulation. Thus it was decided to administer enteral potassium through a nasogastric (NG) tube, placed intraoperatively, in mechanically ventilated patients. Once patients were extubated and started tolerating oral feeds, enteral potassium supplementation was administered with apple juice to improve the taste and palatability of the medicine. These measures were adopted throughout the trial to improve tolerance and compliance to EPR.
Study drugs, drug management
Drug-dosing protocol for potassium replacement is shown in table 1; details about the maximum concentration, dose in each arm and drug management can be reviewed in a previously published protocol.12
Potassium replacement dosing
Intravenous potassium chloride
The maximum dose was 3 mmol/kg/day. The dilution and infusion rate was 8 mmol/100 mL, 10 mmol/hour for a peripheral line; 15 mmol/100 mL, 15 mmol/hour for a central line.
Oral potassium chloride
The maximum dose was 240 mmol/24 hours. The maximum per dose was 60 mmol. The concentration was 13.33 mmol/5 mL.
Adverse events
The adverse effects of potassium supplementation that were monitored included hyperkalaemia (potassium levels >5 mmol/L), arrhythmias, diarrhoea, gastrointestinal bleeds and nausea and vomiting, during or within 2 hours of potassium replacement.
The adverse events were monitored and documented on an hourly basis by PCICU nursing staff and notified to on-call physicians and the principal investigator.
Sample size calculation
The sample size was calculated using an equivalence test of mean procedure, considering both interventions (EPR and IVPR) were of equal efficacy with an SD of 4%. The equivalence limit was assumed to be ±(15%), using a power of 90% and a level of significance of 5%; a total of 155 events were required in each arm to reject the null hypothesis which states that there is no difference in efficacy (change in serum potassium levels) of IVPR and EPR. The sample size was calculated using PASS software.
Statistical analysis
The primary objective of the study was to compare the efficacy of EPR and IVPR as a first-line therapy for the treatment of hypokalaemia. The end points (primary outcome) used were change in serum potassium levels in mmol/L and percentage change in serum potassium levels after each event of potassium replacement by both methods.
Data were analysed using two approaches: intention to treat (ITT) and actual treatment (AT) received analysis. ITT was considered the primary analysis. The mean (±SD) was calculated for continuous parametric variables while the median was used to describe continuous non-parametric variables. Categorical variables are presented as frequencies. To explore bivariate associations, the independent Student t and Mann-Whitney U tests were used for parametric and non-parametric continuous variables respectively, while χ2 was used for categorical variables. Change in potassium concentration over time was assessed by mixed effects regression modelling; this incorporated a random intercept trend. This analytic approach included all participants who had data available on at least one time point. A hierarchical model was developed that nests an event within an episode and patients through random intercept modelling to adjust for inter-individual and episode-related variation in change in potassium concentration. The analysis included linear time effect with main effect of treatment to examine whether the experimental condition (EPR) resulted in greater changes in potassium than the control (IVPR) over time. Age of participants, potassium concentration at beginning of episode, average urine output, diuretic dose and inotrope score were incorporated in the model as confounding factors and the results were reported as coefficients with 95% CIs. Data were analysed using STATA version 12 through xtmixed command. The model building command includes three steps. As a first step an unconditional model was tested with episode and event level random intercepts to examine the variation in outcomes at these levels. In the next step, a time variable was added with outcome as a fixed effect and random slope. A likelihood ratio (LR) test was used to confirm whether the variance of the slope is significantly different from zero. Time was treated as a fixed effect when the LR test failed to provide evidence for this null hypothesis. Finally, outcome adjusted for all potential covariates significant at a liberal p<0.2 in bivariate analysis were retained if significant at p<0.05. Fit of the models was assessed through Akaike information criteria (AIC) and Bayesian information criteria (BIC). Generally the smaller the statistical value, the better the model fits the data.
An interim analysis was performed after 155 events (cumulative in both arms) to ensure protocol compliance and to monitor adverse effects. Analysis did not reveal any major adverse effects and validated comparable efficacy between the two arms. Thus, no major changes were made to the protocol and the trial was continued to achieve the final sample size.
Data collection, storage and record keeping
The data abstraction form was used to abstract patient data for the study.
Data were collected by investigators (NR, QM, AR) throughout the duration of the study and were kept safe under lock and password protected e-files at all times.
Ethics committee and regulatory approval
This study was approved by the ERC and Clinical Trials Unit at Aga Khan University Hospital.
Results
Patients were recruited from December 2013 to May 2014. Initially 55 patients were approached. The first 10 patients were recruited and consented to participate in the pre-trial period; they were not included in the trial analysis. During the pre-trial period, the EPR and IVPR potassium protocol was introduced for the training of staff nurses. The next 45 patients were recruited for the trial. Of these, four were excluded as they did not meet the inclusion criteria (two participants were excluded as they developed critically low levels of potassium, while the other two participants did not develop an episode of hypokalaemia during their PCICU stay). Thus 41 patients fulfilled the inclusion criteria for the trial. There was no attrition from the patients recruited. The most common cardiac lesion in both the groups was found to be a ventricular septal defect (VSD) and the most common surgical procedure was VSD closure. None of the patients received continuous or modified ultrafiltration during or after surgery. After randomisation, 18 patients were recruited to the IVPR arm and 23 patients to the EPR arm. The mean age of patients was 4.8 (SD ±4) in the IVPR group and 4.6 (SD ±4.0) in the EPR group (table 2a).
Baseline characteristics of enrolled children in IVPR and EPR arms
Five patients from the EPR arm crossed over to the IVPR arm (figure 1) due to development of adverse events: four vomiting and one arrhythmia. The median length of PCICU stay was 2 (0.63–14) days and 1.95 (0.58–8) days (p=0.26) in the IVPR and EPR arms respectively. The median length of hospital stay for the IVPR arm was 7 (3–19) days while in the EPR arm it was 6 (4–18) days (p=0.83). A total of 97 episodes of hypokalaemia were recorded (48 and 49 in the IVPR and EPR arms respectively). From these episodes, a total of 460 events of hypokalaemia were recorded (234 and 226 in the IVPR and EPR arms respectively). There was no difference in episodes (IVPR 2.7, SD ±2.1; EPR 2.1, SD ±1.3) and events (number of doses) (IVPR 5.0, SD ±4.9; EPR 4.6, SD ±4.2) per child between the two arms (table 2b).
Episodes, events and mean percentage change in potassium concentration in the IVPR and EPR arms

Recruitment flow chart EIPS.
Mode of supplementation and response to therapy
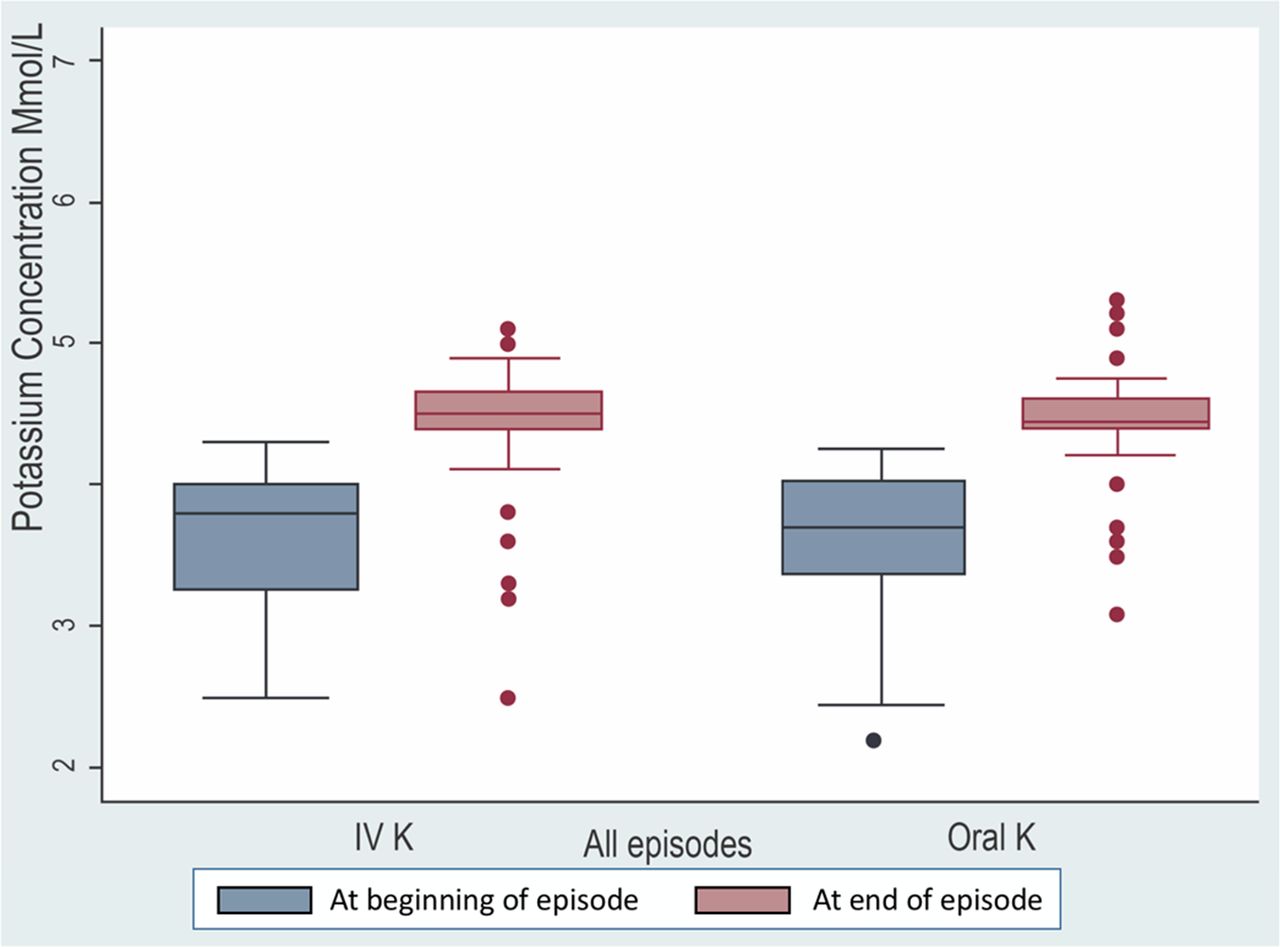
There was no difference between IVPR and EPR arms in the mean serum potassium levels at the beginning (3.67±0.42 vs 3.62±0.48, p=0.45 respectively) and at the end of the episode of hypokalaemia (4.47±0.62 vs 4.48±0.60, p=0.94 respectively) (figure 2).

{kind=link}
{kind=link}
Change in potassium concentration at the beginning and end of episode.
Univariate analysis showed no difference in response to therapy (number of doses required, absolute change (intravenous 0.82±0.7; 95% CI 0.62 to 1.01 vs oral 0.86±0.8; 95% CI 0.62 to 1.10; p=0.8) and percentage change (intravenous 24±20; 95% CI 18 to 30 vs oral 26±30; 95% CI 18 to 35; p=0.59) in potassium levels in both arms at the initial episode (table 2b). The overall difference of relative change in potassium concentration was −2.7% (95% CI −12.8% to 7.3%) with ITT analysis which was within the predetermined equivalence limit (±15%).
Actual treatment received analysis was also performed and findings were not significantly different from ITT analysis.
Using repeated measures analysis, after adjusting for the age of the patient, potassium concentration at the beginning of the episode, average urine output, inotropic score and diuretic dose, the change in absolute potassium level for each event of hypokalaemia was equal with no statistically significant difference between the two arms for ITT (β=0.01; 95% CI −0.08 to 0.10; p=0.86) and actual treatment analysis. Similar results were seen when analysis was performed using percentage change in potassium levels after supplementation for ITT (β=0.30; 95% CI −3.42 to 4.03, p=0.87) and actual treatment analysis (table 3, see online supplementary table 1, table 2, table 3).
Repeated measure analysis of change in serum potassium concentration in IVPR and EPR arms (ITT)
Linear mixed effect regression analysis was adjusted for episode level variations and controlled for covariates of age, potassium levels at the beginning of the episode, inotropic score, average urine output and average diuretic dose. The β coefficient is the standardised coefficient’ showing the degree of impact of intervention on the outcome.
Adverse events
No mortality occurred in either of the arms. A total of five adverse events were observed in the EPR arm while none were recorded in the IVPR arm. Out of these five cases, four were episodes of vomiting within 2 hours of enteral potassium replacement. A single atrial arrhythmia occurred in a 4.5 month old patient who underwent complete repair for tetralogy of Fallot. Abnormal rhythm was noticed an hour after enteral supplementation for treating mild hypokalaemia. Rhythm was evaluated to be a run of ectopic atrial tachycardia. This patient was also noted to have such episodes of tachycardia in the immediate postoperative period before the enteral supplementation was started. The rhythm improved after the patient was placed on oral amiodarone. No episodes of hyperkalaemia were appreciated.
Discussion
Our trial portrays comparable efficacy of both the modes of supplementation, intravenous and enteral, as first-line therapy for the correction of hypokalaemia in paediatric patients in the PCICU setting post cardiac surgery. Through this trial we were able to establish that enteral potassium supplementation is an equally efficacious and safe mode of potassium replacement as first-line therapy during hypokalaemia in selected patients with congenital heart disease in the immediate postoperative period.
Paediatric patients, after congenital heart disease repair, are particularly susceptible to hypokalaemia in the postoperative period due to administration of high doses of loop diuretics and inotropes.1 7 In the immediate postoperative period, the body does not conserve potassium efficiently, thus making potassium supplementation a requirement for many such paediatric patients after cardiac surgery.1 Potassium supplementation has a narrow therapeutic range and thus a guarded safety profile. Although serious adverse effects with either mode of supplementation are quite rare, inappropriate administration of potassium in these patients may lead to worsening of heart failure, cardiac arrest, hyperkalaemia, arrhythmias and death.2 8 9 Given all the above mentioned factors, efficient potassium replacement through a safe route holds pivotal importance in paediatric patients after cardiac surgery.
Comparable efficacy between enteral and intravenous potassium supplementation was initially demonstrated in a recent retrospective study.9 This retrospective study conducted by Moffet et al included 66 paediatric patients post congenital heart surgery who received 399 blouses of potassium (266 intravenous and 233 enteral). As a change of practice was advocated to encourage the use of enteral potassium supplementation before data collection for this retrospective study, the authors believe that the physician’s clinical experience and judgement may have skewed administration of enteral potassium to less critically ill patients. Also, limitations associated with a retrospective review reduced the generalisability of findings of this study. Taking the above-mentioned limitations into consideration, a prospective study with a predefined protocol and practices in place to reduce clinician to clinician variability is warranted.
Although equally efficacious in improving potassium levels, IVPR requires stringent monitoring by PCICU staff and the presence of a central line.9 Correcting potassium levels back to normal usually requires multiple replacements, making repeated access to the central line a necessity. This may lead to central line related infections.9 14 Also, transition to enteral supplementation from IVPR poses a challenge in some patients and central lines have to be kept in place longer than otherwise required for intravenous potassium supplementation.14 Another downside of using IVPR is that a large volume of fluid is required for the delivery of the desired dose of potassium with peripheral lines which is not preferable in postoperative cardiac patients in whom clinicians aim to achieve negative fluid balance. However, enteral supplementation with comparable efficacy offers many advantages. It is easier to transition paediatric patients after surgery for congenital heart disease directly to enteral supplementation and if required they can be discharged home on this supplementation. Moreover, use of enteral potassium supplementation can lead to significant reduction in fluid administration, which is of great advantage as hypokalaemia is frequently a consequence of administration of loop diuretics to treat fluid overload in these patients. Although, paediatric data regarding pharmacokinetics of enteral potassium supplementation are lacking, safety and efficacy of enteral supplementation of potassium in the adult population has been well established previously. One more potential advantage of administrating enteral potassium supplementation for treatment of hypokalaemia is its cost effectiveness.9 Along with being ten times more costly than EPR at our institution, IVPR also requires central line utilisation, increased nursing time and syringe pump utilisation that further adds to the overall cost of potassium supplementation. Adverse events seen in the enteral arm mainly comprised episodes of vomiting seen in some participants at the beginning of the trial. This can be attributed to the sour taste the of formulation or inappropriately fast administration through the NG tube. The former can be taken care of by feeding through the NG tube or mixing the enteral potassium formulation with fruit juices. Other than these few episodes of vomiting, participants in this trial tolerated enteral supplementation of potassium well. Given its equal efficacy, low adverse event profile and a potential benefit, EPR was shown to be an excellent alternative to IVPR as first-line therapy in our patient cohort.
Generalisability
EIPS included patients received in the PCICU after cardiac surgery. The mean age of participants was 4.7 years, with the youngest child being 1 month and the oldest child being 14 years. The predominant surgical procedure was VSD repair surgery. We believe that the results of our study can be generalised to these patient populations. However, there were only two patients with severely low potassium levels (see definition) and patients with critically low potassium, that is <2.0 mmol/L, who were excluded from the trial, thus the results from this trial should be generalised with caution in patients with severely and critically low potassium levels. Further investigation is warranted to determine the safety profile of enteral potassium in these patients. Also, EIPS is a single-centre randomised study, with alternate week patient randomization, leading to potential significant selection and allocation bias and limiting generalisability of the findings.
We used a more aggressive potassium replacement strategy, that is levels between 3.5 and 4.4 mmol/L, based on observations that higher potassium levels are required in cardiac patients.7 Though no episode of hyperkalaemia was noticed in our cohort, our study is not powered to comment on the safety of this strategy.
Limitations
EIPS is a single-centre, non-blinded equivalence study that may lead to observer bias. Blinding was not feasible in this trial owing to different routes of administration of the same supplementation (enteral vs intravenous) and different time interval for checking serum levels in each arm (1 hour after intravenous replacement and 2 hours after enteral replacement). Confounding factors, such as concomitant use of diuretics and inotropic agents during the episode, may have affected potassium metabolism. These factors were identified and were adjusted in the analysis.
An auto-analyser, located in PCICU, was used to measure point of care potassium levels in this trial. This might have been a potential limiting factor in our study. Central lab values, although being gold standard, could not be used as turnover time for each sample at our institution is about 4 hours. Central lab values were obtained only when a critically low or high value was seen on the auto-analyser testing. A strong correlation between two values had previously been established during daily practice at our PCICU.
Difference in severity of the patient’s condition (as depicted by difference in inotropic scores in the 2 arms) may also have confounded our results. This was accounted for at a statistical level by adjusting for inotropic scores in the multivariate modelling and did not seem to affect the results.
Some participants got moved out of PCICU before completion of an episode of hypokalaemia. Patients could not be followed once they moved out of PCICU to a step-down unit or floor as stringent monitoring for trial and point of care potassium levels was not available in floor settings. This does affect the generalisability of study. Routinely, patients who get moved to step-down units or floor receive oral potassium supplementation in our institution.
It is imperative to know that enteral potassium replacement may not be possible in some patients due to gastrointestinal intolerance.
Lastly, our trial was also underpowered to detect difference in frequency of adverse effects between both arms. This limits inference of equivalence between the two modes when it comes to their safety/adverse events profile.
Conclusion
We found similar effectiveness of EPR or IVPR, as first-line therapy, in treating hypokalaemia in paediatric patients after surgery for congenital heart disease. EPR may be an equally efficacious alternative to treat hypokalaemia, as first-line therapy, in these patients.
Supplementary Material
Supplementary dataReferences
Footnotes
Contributors NR, QM, MA, AH and BH contributed equally to the research idea, study design, protocol writing, initiation, data acquisition, analysis and manuscript writing. AR contributed in data acquiring, analysis of data and manuscript writing. BH was the senior author on this project involved in study idea genesis, design, data analysis and interpretation and manuscript writing. All authors have read and approved final manuscript.
Funding All authors declare no support from any organisation for submitted work, no financial relationships with any organisations that might have an interest in the submitted work in the previous 3 years and no other relationships or activities that could appear to have influenced the submitted work.
Competing interests None declared.
Patient consent Guardian consent obtained.
Ethics approval ERC AKU.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Additional data are available on request.