Article Text

Abstract
Background We have previously reported, in a systematic review of 181 studies, that restriction of antibiotic use in food-producing animals is associated with a reduction in antibiotic-resistant bacterial isolates. While informative, that report did not concretely specify whether different types of restriction are associated with differential effectiveness in reducing resistance. We undertook a sub-analysis of the systematic review to address this question.
Methods We created a classification scheme of different approaches to antibiotic restriction: (1) complete restriction; (2) single antibiotic-class restriction; (3) single antibiotic restriction; (4) all non-therapeutic use restriction; (5) growth promoter and prophylaxis restriction; (6) growth promoter restriction and (7) other/undetermined. All studies in the original systematic review that were amenable to meta-analysis were included into this substudy and coded by intervention type. Meta-analyses were conducted using random effects models, stratified by intervention type.
Results A total of 127 studies were included. The most frequently studied intervention type was complete restriction (n=51), followed by restriction of non-therapeutic (n=33) and growth promoter (n=19) indications. None examined growth promoter and prophylaxis restrictions together. Three and seven studies examined single antibiotic-class and single antibiotic restrictions, respectively; these two intervention types were not significantly associated with reductions in antibiotic resistance. Though complete restrictions were associated with a 15% reduction in antibiotic resistance, less prohibitive approaches also demonstrated reduction in antibiotic resistance of 9%–30%.
Conclusion Broad interventions that restrict global antibiotic use appear to be more effective in reducing antibiotic resistance compared with restrictions that narrowly target one specific antibiotic or antibiotic class. Importantly, interventions that allow for therapeutic antibiotic use appear similarly effective compared with those that restrict all uses of antibiotics, suggesting that complete bans are not necessary. These findings directly inform the creation of specific policies to restrict antibiotic use in food-producing animals.
- systematic review
- public health
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
Antimicrobial resistance (AMR) is a threat to public health, with the Tripartite Collaboration (WHO, the Food and Agriculture Organisation of the United Nations and the World Organisation for Animal Health) calling for a One Health approach to address this crisis.
A recent systematic review and meta-analysis suggested that, in general, interventions that restrict antibiotic use in food-producing animals are effective in reducing AMR in these animals and in certain subgroups of human population, though whether certain types of interventions are more effective than others remains unknown.
What are the new findings?
A wide spectrum of interventions, from limiting antibiotics for growth promoter or feed additive purposes only to limiting all uses of antibiotics (including for therapy), were associated with a 9%–30% absolute reduction in antibiotic resistance.
Interventions that restrict the use of only one antibiotic or antibiotic class were not significantly associated with a reduction in antibiotic resistance.
What do the new findings imply?
Highly targeted interventions that limit the use of only a single antibiotic or antibiotic class may have limited effectiveness in reducing antibiotic resistance.
Interventions that broadly target overall antibiotic use or that restrict the use of multiple antibiotic classes are recommended as these appear to be associated with reductions in antibiotic resistance, though a complete restriction of antibiotics does not appear to be necessary.
Introduction
Antimicrobial resistance (AMR) has been recognised as a threat to public health worldwide, being associated with increased morbidity, mortality and societal costs.1–4 It is estimated that by 2050, AMR will contribute to 10 million deaths per year, a 2%–3.5% reduction in gross domestic product, and cost $100 trillion US$ worldwide.5 Over-prescription and unnecessary non-prescription antibiotic use are the main contributors to increase AMR in humans.6 Widespread antibiotic use in agriculture and aquaculture also likely plays a role,7–9 especially as many of the antibiotics used in animals are the same, or are in the same class, as antibiotics used in humans.8 10–12 The WHO, the Food and Agriculture Organisation of the United Nations and the World Organisation for Animal Health, known as the Tripartite Collaboration, have called for a One Health approach, with recognition that animal, human and environmental health are linked, to address the problem of AMR.13
A systematic review conducted by our group showed that interventions that aimed to reduce antibiotic use in food-producing animals are associated with a reduction in AMR in these animals, as well as in certain subgroups of the human population (particularly those with direct contact with animals).14 These findings were critical in demonstrating that reducing antibiotic use in agriculture is an effective avenue by which to combat the growing problem of AMR worldwide. However, the studies included in the systematic review used many different approaches to reduce and/or to restrict antibiotic use. Our report did not address whether different types and extent of antibiotic restriction lead to different levels of reduction in antibiotic resistance. That is, though antibiotic restrictions appear, in a broad sense, to be effective in reducing resistance, it is unclear whether specific types of restrictions are more effective than others.
Antibiotics can be used in food-producing animals for therapeutic purposes (ie, to treat existing infectious disease), for disease control within a herd or flock, and for non-therapeutic purposes.15 This results in a wide spectrum of possible approaches to antibiotic restriction. The least restrictive approaches would include those that prohibit the use of only one antibiotic or antibiotic class, and those that restrict the use of antibiotics for specific non-therapeutic indications only such as for growth promotion. On the opposite end of the spectrum is the complete prohibition of the use of all antibiotics, for any indication. With the least restrictive approaches, there is risk of increased use of other antibiotics in the place of the restricted drug(s), thereby raising the question of whether such measures actually reduce AMR.16 17 On the other hand, while antibiotic-free strategies may be effective in reducing AMR, the inability to use antibiotics, even to treat diagnosed clinical infectious diseases, is detrimental for animal production and economics as well as to animal welfare.18 19
The development of national and international guidelines and policies requires greater detail about the effectiveness of different interventions so that specific recommendations can be made as to what type of antibiotic restrictions should be implemented. We were commissioned by the WHO to undertake a subanalysis of the original systematic review and meta-analysis to explore the associations between different interventions that restrict antibiotic use in food-producing animals and antibiotic resistance in these animals, to inform the WHO Guidelines on the use of antibiotics in food-producing animals.20 Our findings provide crucial insights into the type and extent of antibiotic restriction that optimises desired effects of reducing AMR.
Methods
The methods for the broader systematic review and meta-analysis, of which this is a substudy, have been described in detail in a prior publication.14 The systematic review and meta-analysis was conducted following a predetermined protocol and in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses reporting standards.21 Ethics approval was not required, as the study is based on a review of published literature.
Search strategy
The search strategy consisted of controlled vocabulary and keywords, under three themes: animal populations of interest (theme 1), resistance to antibiotics (theme 2)22 23 and interventions to restrict antibiotic use (theme 3). These three themes were combined with the Boolean operator ‘AND’. Electronic databases were searched in initially searched in July 2016, and again in January 2017. Databases included Agricola (1970–present), AGRIS (http://agris.fao.org), BIOSIS Previews (1980–present), CAB Abstracts (1910–present), MEDLINE (1946–present), EMBASE (1974–present), Global Index Medicus (http://www.globalhealthlibrary.net; non-MEDLINE indices included AIM (AFRO), LILACS (AMRO/PAHO), IMEMR (EMRO), IMSEAR (SEARO), WPRIM (WPRO), WHOLIS (KMS) and SciELO), ProQuest Dissertations and Science Citation Index (1899–present). No limits were placed based on publication date or language. An update to the search was conducted on 8 July 2019, focusing on the electronic databases MEDLINE, EMBASE, CAB Abstracts, and AGRIS.
Reference lists of included articles (published 2010 onward) were manually searched. Grey literature searching included websites of relevant health agencies, professional associations and other specialised databases. The WHO Guideline Development Group as well as experts in antimicrobial use and resistance, veterinary medicine and animal health policy were contacted to identify potential missed, ongoing or unpublished studies.
Abstract screening and full-text review
Two authors independently reviewed all identified titles and abstracts for eligibility. Only articles reporting original research that described an intervention aimed to reduce antibiotic use in animals and described antibiotic resistance in animals or humans were selected for full-text review. At the full-text review stage, articles were retained and ultimately included into this substudy if they were original research meeting the following inclusion criteria: (1) population studied included food-producing animals (within the classifications of avian, swine, bovine, caprine, camel, equine, rabbit, ovine, fish, bees, molluscs and crustaceans); (2) interventions restricted the use of antibiotics in food-producing animals; (3) presence of a comparator group without antibiotic use restrictions (historical comparators were considered eligible); (4) outcomes reported phenotypic antibiotic resistance in bacteria in food-producing animals and (5) sufficient data reported to calculate risk differences (RDs) in proportion of isolates with antibiotic resistance in the intervention versus the comparator group (to allow for meta-analysis).
Data extraction and assessment of individual study quality
Two authors (KT and NC) extracted data from each included study using a predesigned form. Data extracted included study design, country, animal characteristics, sampling characteristics, description of intervention, description of comparator, bacteria investigated, and prevalence of antibiotic resistance in intervention and comparator groups. The same authors independently assessed the methodological quality of each study based on pre-specified study quality indicators adapted from the Downs and Black checklist.24 The results of the quality assessment are described in a prior publication.14
Patient and public involvement
Due to the nature of the research question, which was defined by the WHO and which used data from our prior review of published literature, patients were not involved in this study.
Creation of an intervention classification scheme
The WHO commissioned this study to inform the development of Guidelines on this topic. The initial request for a classification scheme therefore originated from the WHO Advisory Group on Integrated Surveillance of Antimicrobial Resistance (WHO AGISAR) Guideline Development Group committee members. Because there is no widely accepted classification scheme to categorise interventions that restrict and/or reduce antibiotic use, we developed one from the ground-up, based on the types of interventions found in the literature. The preliminary categories that were developed were then presented to WHO AGISAR for input and feedback, and then iteratively refined.
We began by establishing standard terminology to be used in this classification scheme, as different jurisdictions may use terminology differently. For example, the definition for metaphylaxis provided by the US Department of Agriculture includes the prophylactic use of antibiotics in healthy animals to prevent disease (even when there are no clinically affected animals present),25 whereas the definition from the European Medicines Agency does not.26 Furthermore, some consider metaphylaxis to be a therapeutic indication of antibiotic use (ie, it is considered to be ‘group treatment’ of animals)26 while others note that antibiotic use is only therapeutic if administered in clinically infected animals.27 The latter definition would therefore consider metaphylaxis not to be therapy, but rather disease prevention. We consulted the veterinary experts on the study team along with the WHO Guideline Development Group for definitions for the terms ‘antibiotic growth promotor’, ‘metaphylaxis’, ‘prophylaxis’, ‘non-therapeutic antibiotic use’ and ‘therapeutic antibiotic use’. Consensus was reached for the definitions provided in table 1, which were then used in our classification scheme.
Definitions for terms used in the classification scheme for interventions
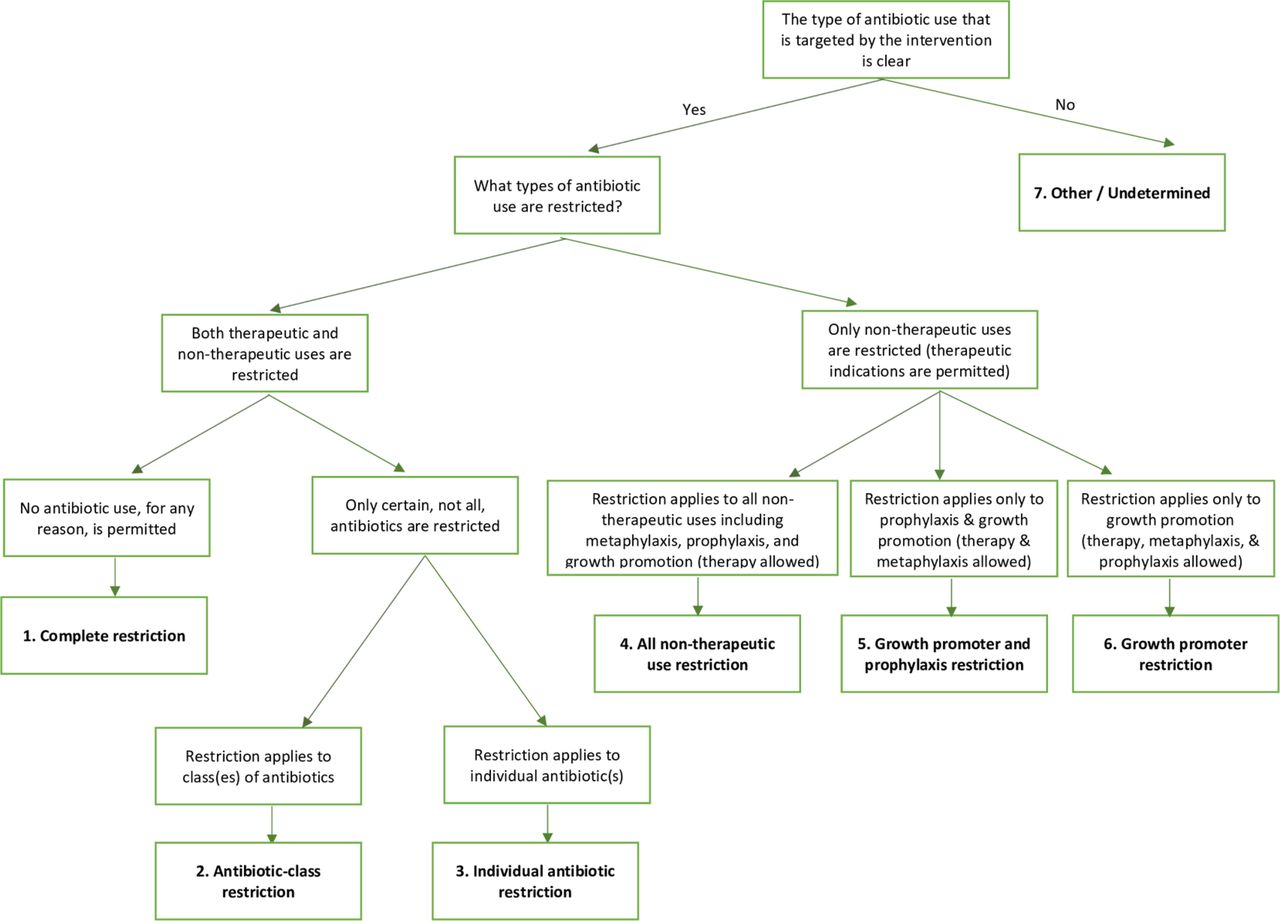
In total, we created seven categories of interventions (table 2): (1) complete restriction; (2) restriction of use of a single antibiotic class; (3) restriction of use of a single antibiotic; (4) all non-therapeutic use restriction; (5) growth promoter and prophylaxis restriction; (6) growth promoter restriction and (7) other/undetermined. Each intervention was assigned only one category. If a study included more than one intervention, then each intervention was classified separately based on the above approach. The ‘growth promoter restriction’ category did not require the restriction of all available antibiotic growth promoters. That is, interventions that restricted one or more growth promoters were eligible to be included in this category, even if there was residual use of other non-restricted growth promoters (eg, ionophores and flavophospholipols). The ‘other/undetermined’ category captures studies that did not specify the type of antibiotic use or indication that was targeted in the antibiotic restriction strategy. This includes studies, for example, that compare regions or farms using ‘more’ versus ‘less’ antibiotics with no indication of what is specifically targeted or described, or studies that assess the impact of reducing antibiotic use in a jurisdiction without delineating how this is achieved. An algorithm was created to ensure reproducibility in how interventions are classified into the different categories (figure 1).
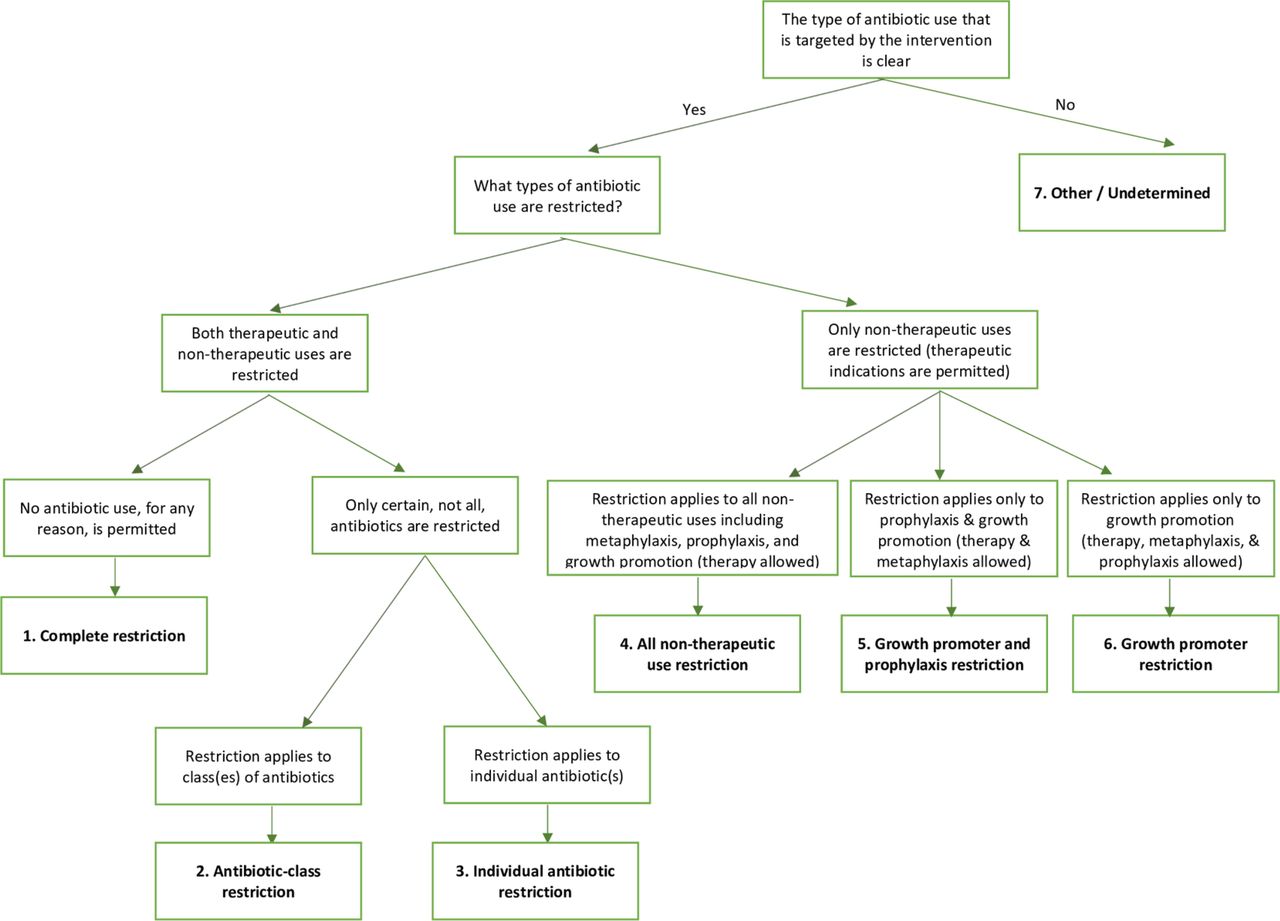
Algorithm for the classification of interventions to restrict antibiotic use in food-producing animals.
Classification of interventions that restrict antibiotic use in food-producing animals
We anticipated that some studies may use labels to define the intervention, without further description. Such labels might include ‘organic’ or ‘antibiotic-free’ production. We established a set of decision rules a priori. These included the following:
Interventions involving organic production in the USA were classified as ‘complete restriction’, as organic certification in the USA specifies that animals are raised without any exposure to antibiotics.28
Interventions involving organic production in Europe were classified as ‘all non-therapeutic use restriction’ as the European Commission on organic production specifies that animals are allowed limited antibiotics for therapeutic purposes.29 30
We referred to organic certification standards, if cited, for interventions involving organic production in countries outside of the USA and Europe.
Interventions where no such certifications exist (eg, ‘antibiotic-free’, ‘pasture’ or ‘free range’) were classified as ‘undetermined/other’ unless sufficient detail was provided for classification into any other category.
Outcome measure
Antibiotic resistance was considered a dichotomous outcome, as classified by the individual primary studies. Intermediate susceptibility was considered susceptible. Absolute RDs were calculated for each individual antibiotic in each study by subtracting the proportion of resistant isolates in the control group from the proportion in the intervention group.
Meta-analysis
All meta-analyses were stratified by intervention type. To allow for meaningful and adequately powered analysis within each intervention stratum, all included studies were pooled, regardless of the animal populations, sample types or bacterial species studied. A single effect estimate (absolute RD) was generated for each study by conducting within-study meta-analysis using random effects models.
Absolute RDs across all studies were then pooled using DerSimonian and Laird random-effects models. This method was chosen due to the known clinical heterogeneity across studies, with studies from different regions examining different animal populations, sample types and bacteria.31 A lower prevalence of antibiotic resistance in the intervention group compared with the control group would result in a negative pooled absolute RD. Recognising that RDs must be interpreted in the context of baseline prevalence of antibiotic resistance, we conducted additional meta-analysis, pooling the prevalence of antibiotic resistance in the comparator groups, stratified by intervention type, using random-effects models. Heterogeneity across studies was evaluated using the I2 statistic.32 33 Meta-regression was conducted, with each intervention type being a covariate. A joint test for all covariates was conducted, to test whether intervention type was associated with the size of the outcome effect (ie, antibiotic resistance).34
Role of the funding source
The WHO was involved in both the original systematic review and meta-analysis, as well as this substudy. They were involved in developing the research question, the study design and the study protocol. They had no involvement in data extraction or interpretation of findings. The authors have been given permission by the WHO to publish this article.
Results
Identification of studies
The initial search strategy identified 9008 citations from electronic databases. An additional 56 studies were identified by contacting experts, and another 82 by searching reference lists. After removal of duplicates, 5945 records underwent title and abstract review. Of these, 5559 records were not relevant to the research objective, and 386 full-text articles were reviewed. A total of 181 studies were included in the larger original systematic review. Of these, two were excluded as they examined AMR outcomes in humans but not animals, 17 were excluded as they reported presence of resistant genetic elements with no phenotypic resistance outcomes, and 48 were excluded as there were insufficient data to allow for meta-analysis. Therefore, 114 studies from the original systematic review were included in this substudy. In addition, an update to the search was conducted July 2019, at which time a total of 1208 new records were identified. After duplicates were removed, 703 underwent title and abstract review. Of these, 659 were excluded as were not relevant to the research objective, and 44 full-text articles were reviewed, of which 13 ultimately met criteria to be included into this study. In total, 127 studies were included into this systematic review and meta-analysis (figure 2).

{kind=link}
{kind=link}
PreferredReporting Items for Systematic Reviews and Meta-Analyses flow diagram of the study selection process.
Study characteristics
Of the 127 studies, 51 restricted all use of antibiotics (complete restriction),35–85 three restricted use of a single antibiotic class86–88 and seven restricted use of a single specific antibiotic.89–95 In all, 33 studies restricted use of antibiotics for all non-therapeutic purposes,48 96–127 and 19 restricted antibiotic growth promoters only.128–146 A total of 21 studies were classified into the ‘other/undetermined’ category.52 53 83 100 137 147–162 Of note, seven studies consisted of two different interventions and were therefore included into two separate categories.48 52 53 83 100 122 137
A summary of study characteristics is found in table 3. In total, 114 of the 127 studies were journal articles. There were eight dissertations and six meeting abstracts/conference proceedings. The majority had a cross-sectional design. Poultry (n=69) was the most commonly studied animal population, followed by swine (n=42) and dairy cattle (n=19). Antibiotic resistance was most commonly assessed in the bacterial group Enterobacteriaceae. In all, 65 studies were from North America and 53 were from Europe. Few study populations were from Asia (n=6), Africa (n=1), Australasia (n=2) and South America (n=1). Detailed study characteristics for individual studies can be found in a prior publication,14 as well as in online supplementary appendix 1 table S1.
Supplemental material
Summary of study characteristics
Meta-analysis by intervention category
All intervention types were associated with a significantly lower pooled risk of antibiotic resistance in the intervention group compared with the comparator group except for single antibiotic-class and single antibiotic restrictions (RD −0.02, 95% CI −0.10, 0.05 and RD −0.11, 95% CI −0.21, 0.01 respectively, see table 4). The pooled risk reduction of antibiotic resistance was greatest for growth promoter restrictions (RD −0.30, 95% CI −0.42 to -0.17). That is, for interventions that restricted the use of antibiotic growth promoters, there was a 30% reduction in the proportion of isolates that were antibiotic resistant in the intervention group compared with the comparator group. Similarly, there was a 10% and 15% reduction in the proportion of antibiotic-resistant isolates for interventions that restricted all non-therapeutic uses of antibiotics and interventions that completely restricted all (non-therapeutic and therapeutic) uses of antibiotics, respectively. The I2 for each intervention stratum ranged between 89.0% and 98.5%, suggesting the presence of considerable heterogeneity. The meta-regression joint p value was 0.046, suggesting that the type of intervention significantly affected the magnitude of reduction in antibiotic resistance.
Meta-analysis stratified by intervention category
Pooled proportions of antibiotic resistance in comparator groups
The pooled proportion of bacterial isolates with antibiotic resistance in comparator groups was lowest for studies that single antibiotic-class restrictions (pooled proportion 0.163, 95% CI 0.075 to 0.252, see table 4), and highest for studies examining interventions that restricted growth promoter use only (pooled proportion 0.492, 95% CI 0.261 to 0.723). The pooled proportions for complete restriction, all non-therapeutic use restriction and other/undetermined restriction were similar, between 0.32 and 0.34.
Discussion
Though our broader systematic review and meta-analysis was important in bringing to light the effectiveness of antibiotic use restrictions on decreasing antibiotic resistance in food-producing animals, what has remained unknown until now is how to best implement this broad principle into practice and policy. This subanalysis plays a critical role in providing answers that can guide antibiotic use strategies in food-producing animals.
We demonstrate that highly targeted interventions limiting the use of single antibiotics or a single class of antibiotics are unlikely to be effective in reducing overall AMR. One reason for this finding may be that the use of the restricted antibiotic(s) is simply replaced by other antibiotics, such that there is no overall reduction in antibiotic use. This phenomenon was seen in Denmark. After the ban on the antibiotic growth promoter avoparcin, there was increased use of other growth promoters, including tylosin and virginiamycin, in its place.131 Furthermore, there may be continued resistance to certain antibiotic classes even after selected classes have been banned or restricted because of co-selection. Because genes that encode resistance to different antibiotics may be linked (ie, carried on the same mobile genetic element), the continued use of just one of these antibiotics is sufficient to select for all of the linked resistance mechanisms to the different antibiotics.163 This phenomenon was described in pigs where macrolide and glycopeptide resistance genes were linked. In this case, the ban of avoparcin did not result in reduced glycopeptide resistance, due to continued macrolide use.164 165
Conversely, a complete ban on the use of all antibiotics in food-producing animals does not appear to be necessary. Though antibiotic-free practices were associated with a 15% reduction in antibiotic resistance, less prohibitive practices are associated with similar reductions. Given that complete restrictions do not appear superior in this regard, and with the added economic, production and ethical challenges of such practices, complete bans are not recommended. Beyond this, it is more difficult to ascertain whether certain less-restrictive types of interventions are superior to others.
At first glance, interventions that restrict antibiotic growth promoters appear to be most effective at reducing AMR in food-producing animals (RD −0.30, 95% CI −0.42 to 0.17). However, growth promoter bans are often the first types of restrictions implemented; other interventions such as those limiting other non-therapeutic uses of antibiotics or all uses of antibiotics tend to be later interventions that are implemented after growth promoter bans or after other efforts to reduce antibiotic use are already in place. The large effect of antibiotic growth promoter bans relative to those of other interventions may therefore be due to the different comparator groups across the different interventions. Lending support to this hypothesis is that growth promoter ban studies tended to be published earlier (median year of publication 2001, IQR 2000–2004) compared with studies examining all other types of interventions (median 2010, IQR 2006–2015). Further support is provided through stratified meta-analysis of baseline proportions of isolates demonstrating antibiotic resistance. As predicted, the pooled baseline proportion of antibiotic resistance for growth promoter ban studies was higher compared with non-therapeutic antibiotic restriction and complete restriction studies (49% vs 32%). The smaller effect size for non-therapeutic restriction studies may therefore be explained, at least in part, by the lower baseline risk of antibiotic resistance (resulting in smaller RDs even if relative effects of the intervention are as large as the ones seen with growth promoter ban studies) and/or the smaller incremental benefit to antibiotic restriction once strategies to ban growth promotion claims on medically important antibiotics are already in place. We therefore cannot conclude that restrictions that target antibiotic growth promoters alone are more effective in reducing AMR compared with restrictions that target non-therapeutic indications more broadly. On the other hand, we have demonstrated that antibiotic growth promoter bans are effective in reducing AMR and therefore recommend that these be implemented on a global scale.
There are limitations to this systematic review. First, the comparison among intervention types through stratified analysis is inferior to comparison through head-to-head randomised controlled trials. However, such head-to-head randomised comparisons of different antibiotic restriction strategies do not exist in the primary literature. Furthermore, our stratified analysis findings are powerful especially as the differences in outcome effect across intervention types are consistent with prior experience and are biologically plausible (particularly the finding that very narrow restrictions are ineffective in reducing AMR while broader restrictions are). Second, there is known clinical heterogeneity across studies, with different countries, livestock production sectors, animal groups and resistance to different bacterial species included. Despite this, our original systematic review and meta-analysis demonstrated consistency in findings across many different layers of stratification, suggesting the presence of an overall effect. Third, we were limited in our classification of interventions by the lack of detailed description of interventions within primary studies. Similarly, because the majority of studies did not provide any description of the implementation process, we were not able to assess how the quality of implementation may affect the effectiveness of interventions in reducing AMR. Our analysis suggests that well-implemented interventions that have national certification standards (eg, for organic production) may be more effective than interventions that have similar claims but no such standard (eg, ‘antibiotic-free’ products). The former was categorised as ‘complete restriction’ (if undertaken in the USA), which was associated with a 15% reduction in antibiotic resistance, while the latter was classified in the ‘other/undetermined’ category, which was associated with a 9% reduction. A more in-depth analysis, though, could not be completed without more information and description about implementation of each intervention in the primary studies. Lastly, the vast majority of studies originated from either North America or Europe. Generalisability of these findings to other jurisdictions may be limited, particularly in low-income countries where there may be limited access to veterinarians, less investment in biosecurity166 and different antimicrobial use patterns.
Though we previously found that interventions that restrict antibiotic use in food-producing animals in general are effective in reducing AMR,14 the practical applications were limited due to the broad nature of the research question and analyses. It has been unclear until now which specific interventions should or should not be recommended to achieve the goal of reducing AMR. This substudy provides insight to these policy-relevant questions. We show that broad interventions that restrict the use of a full spectrum of antibiotic classes are needed. We also show, however, that complete bans on all antibiotic use are not necessary, as judicious use of antibiotics (such as for the treatment of clinical disease in affected animals) does not appear to hinder efforts to reduce AMR. These findings have directly informed WHO Guidelines on use of medically important antimicrobials in food-producing animals,20 and are directly relevant to public health policy globally.
Acknowledgments
This study was commissioned and paid for by the WHO. Copyright in the original work on which this article is based belongs to the WHO. The authors have been given permission to publish this article.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.↵
- 103.↵
- 104.↵
- 105.↵
- 106.↵
- 107.↵
- 108.↵
- 109.↵
- 110.↵
- 111.↵
- 112.↵
- 113.↵
- 114.↵
- 115.↵
- 116.↵
- 117.↵
- 118.↵
- 119.↵
- 120.↵
- 121.↵
- 122.↵
- 123.↵
- 124.↵
- 125.↵
- 126.↵
- 127.↵
- 128.↵
- 129.↵
- 130.↵
- 131.↵
- 132.↵
- 133.↵
- 134.↵
- 135.↵
- 136.↵
- 137.↵
- 138.↵
- 139.↵
- 140.↵
- 141.↵
- 142.↵
- 143.↵
- 144.↵
- 145.↵
- 146.↵
- 147.↵
- 148.↵
- 149.↵
- 150.↵
- 151.↵
- 152.↵
- 153.↵
- 154.↵
- 155.↵
- 156.↵
- 157.↵
- 158.↵
- 159.↵
- 160.↵
- 161.↵
- 162.↵
- 163.↵
- 164.↵
- 165.↵
- 166.↵
- 167.
Footnotes
Handling editor Peter MacGarr Rabinowitz
Contributors Each of the 12 authors meets the authorship requirements as established by the International Committee of Medical Journal Editors in the Uniform Requirements for Manuscripts Submitted to Biomedical Journals. All authors were involved in the design and development of the study. HG created the search strategy and conducted the literature search in electronic databases. DN conducted the grey literature search. KT and NC screened all studies for inclusion into the systematic review and performed all study quality assessments. SC, PR and HB provided input on studies where consensus could not be reached. KT, NC, DN, AP and NS performed data extraction. All authors contributed to data interpretation and data analysis. KT drafted the manuscript and all authors revised it critically for content. All authors have read and approved the manuscript. KT accepts full responsibility for the work and conduct of the study, had access to the data and controlled the decision to publish. The corresponding author (KT) attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Funding This study was funded by World Health Organization.
Disclaimer The authors alone are responsible for the views expressed in this publication and do not necessarily represent the views, decisions, or policies of the World Health Organization.
Competing interests JK has an unrestricted grant as a principal investigator from Pfizer Canada to conduct an epidemiological study of invasive pneumococcal disease in humans, including impact of pneumococcal vaccines, and has a contract with GSK Canada as a local co-investigator a clinical trial of a maternal pertussis vaccine; no other relationships or activities that could appear to have influenced the submitted work. All other authors report no other relationships or activities that could appear to have influenced the submitted work.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.