Article Text

Abstract
Background Short birth intervals are a major risk factor for poor maternal and newborn outcomes. Utilisation of modern contraceptive methods during the postpartum period can reduce risky birth intervals but contraceptive coverage during this critical period remains low.
Methods We conducted a randomised controlled experiment to test whether vouchers for free contraception, provided with and without behavioural ‘nudges’, could increase modern contraceptive use in the postpartum period. 686 pregnant women attending antenatal care in two private maternity hospitals in Nairobi, Kenya, were enrolled in the study. The primary outcomes were the use of modern contraceptive methods at nearly 3 months and 6 months after expected delivery date (EDD). We tested the impact of a standard voucher that could be redeemed for free modern contraception, a deadline voucher that expired 2 months after delivery and both types of vouchers with and without a short message service (SMS) reminder, relative to a control group that received no voucher and no SMS reminder.
Results By nearly 6 months after EDD, we find that the combination of the standard voucher with an SMS reminder increased the probability of reporting utilisation of a modern contraceptive method by 25 percentage points (pp) (95% CI 6 pp to 44 pp) compared with the control group. Estimated impacts in other treatment arms were not statistically significantly different from the control group.
Conclusions Reducing financial barriers to postpartum contraception alone may not be enough to encourage take-up. Programmes targeting the postpartum period should consider addressing behavioural barriers to take-up.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key questions
What is already known?
Access to family planning is a critical element of delivering on Sustainable Development Goals.
Behavioural ‘nudges’ can influence health behaviours but more evidence is needed in the context of family planning.
What are the new findings?
Free contraception alone is not enough to increase take-up of modern contraception.
The combination of free contraception and a short message service (SMS) reminder increases take-up of contraception.
What do the new findings imply?
Programmes seeking to remove barriers to the take-up of postpartum contraception should consider addressing behavioural barriers.
Introduction
The utilisation of modern contraceptive methods to achieve desired birth spacing has the potential to reduce maternal and neonatal mortality and morbidity.1 2 Short birth intervals contribute to greater risk of adverse birth outcomes, preterm birth and neonatal morbidity.3–5 Investments in family planning are estimated to have the highest benefit–cost ratio for economic development among a suite of population and demography programmes.6
Family planning has received renewed policy interest with the Sustainable Development Goals specifically identifying universal access to family planning as a major priority. In response to evidence that family planning had been neglected as a health systems priority in sub-Saharan Africa,7 many countries invested significant resources in improving access to family planning as part of the Family Planning 2020 global partnership, with recent evidence illustrating significant progress in addressing unmet need in Kenya.8
Despite these advances, take-up of modern methods remains low during the critical postpartum period.9–11 In particular, poor households’ utilisation of modern contraceptives has consistently lagged behind national averages across most of sub-Saharan Africa.12 A study conducted among the slums of Nairobi found that 20% of second and higher order births occurred within 24 months of the previous birth and 9% occurred within 18 months.13 Another recent study found that a significant majority of women in Nairobi have not taken up modern contraception at the time of resuming sexual activity in the postpartum period, leaving them only partially protected from shortly spaced births.14
Efforts to improve access to postpartum family planning and ensure equity in the availability of modern contraception across socioeconomic groups have driven the design of interventions to reduce financial barriers to the take-up of contraception.15 Cost is a particularly important barrier to use of long-acting reversible contraception (LARC) methods such as implants and intrauterine devices (IUDs) and systems, which are 20 times as effective as other methods16 but typically require more out-of-pocket spending. However, reductions in financial barriers have not always led to expected increases in postpartum contraception. An evaluation of a voucher programme in Kenya offering subsidised long-acting family planning methods to poor households found that only 2% of households used the vouchers.17 Financial barriers may not be the only reason that new mothers desiring to postpone or avoid pregnancy do not take up modern contraception.18
The postpartum period poses unique challenges for mothers. They must balance the many demands of a new baby with other longer term priorities such as avoiding or delaying future pregnancies. Research in behavioural science suggests that the many cognitive demands of living in poverty may deplete mental resources for forward-looking activities,19 20 such as taking steps to avoid unwanted future pregnancies. The possibility of becoming pregnant may not be at the ‘top of mind’21 and the immediate costs of going to a clinic to access a modern contraceptive method may loom larger than the longer term benefits. Delivery strategies incorporating behavioural ‘nudges’18 into the delivery of postpartum family planning may be particularly important for households living under the cognitive load of poverty. Principles from behavioural science have increasingly been used to design policy innovations. However, there is very limited evidence on the impact of interventions informed by behavioural science to improve maternal and child health.22
We conducted a randomised controlled trial with a chain of private maternity clinics in the informal settlements of Nairobi to evaluate the impact of a free voucher for modern contraception and two behavioural ‘nudges’—a deadline for using the voucher and a short message service (SMS) reminder—on the take up of contraception in the postpartum period. Treatments were designed in collaboration with staff from the study clinic and conversations with patients. We focused our design on integrating behavioural insights into interventions (vouchers and SMS) that were likely to be policy relevant and scalable. Introducing a deadline to encourage earlier action has been found to increase the chance of taking action in education and consumer behaviour,23 while reminders have been shown to increase the likelihood of many health behaviours including appointment attendance and medication adherence.24 This project is among the first to test whether incorporating simple, low-cost nudges to traditional reproductive health voucher programme in low-income countries can increase their effectiveness by targeting behavioural barriers to utilisation at the same time as financial constraints.
Methods
Study setting and population
The study was conducted between April 2014 and December 2015 in two private maternity clinics in Nairobi’s informal settlements (Kiambu County). These densely populated areas are characterised by high poverty rates, poor access to water and sanitation and food insecurity.25 26 Total fertility rates for women in Nairobi’s urban poor regions are slightly higher than that of Nairobi (3.1 compared with 2.8) yet still lower than rural areas and the national average of 4.6.26 27
We recruited pregnant women attending antenatal care (ANC) at Jacaranda Health, a private-sector social enterprise providing maternal and newborn healthcare to poor urban women. At the start of the study, Jacaranda operated one maternity facility with a second facility opening in September 2014.
Intervention design, procedures and timeline
Women were eligible to participate in the study if they attended ANC services at Jacaranda, were between 18 years and 40 years old, had a gestational age of at least 7 months at the time of enrolment and could provide a valid phone number by which they could be reached in the postpartum period. Six hundred and eighty-six women attending ANC were consented and enrolled over that time period. Pregnant women were randomly assigned with equal probability to a ‘standard voucher arm’, a ‘deadline voucher’ arm or a control group. Both voucher arms received a voucher for free contraceptive methods to be redeemed at a Jacaranda Health facility, including condoms, injectables, implants, IUDs, combined and progestin-only oral contraceptives and counselling on effective use of the lactational amenorrhoea method (LAM). The value of the voucher ranged from US$0.92–US$6.45 depending on the method choice, with the largest value for the LARC methods of implants and IUDs. The ‘deadline voucher’ voucher expired 8 weeks after estimated date of delivery (EDD) and the ‘standard voucher’ expired 1 year after it was issued. A sample of each voucher is provided in online supplementary figure 1. The expiry date was made highly salient in the deadline voucher but not in the standard voucher. We used the EDD to determine the deadline date because the delivery date was unknown at the time of enrolment. Partway through the study, additional funding was received, which allowed us to expand the study (we refer to these periods as study phase 1 and phase 2). Around the same time, Jacaranda Health opened another maternity clinic, allowing for a larger potential sample size for the study. During the initial study period, we had observed unexpectedly low rates of redemptions of vouchers. Motivated in part by this observation, we designed an additional intervention to remind households of the opportunity to take up postpartum family planning. In November 2014, a cross-randomised additional treatment arm was added to the study design. Of the 686 total of women enrolled in the study, 339 were enrolled after November 2014 and, in addition to being randomly assigned with equal probability to one of three voucher arms, were also cross-randomised with equal probability into an arm that received a postpartum (5 weeks) SMS reminder or an arm receiving no SMS message, resulting in six treatment arms. Additional details about the study design and randomisation method are provided in the online supplementary appendix. Flow into experimental treatment arms is illustrated for each study phase in online supplementary figure 2a and bonline supplementary figure 2abonline supplementary material 1.
Supplemental material
All participants, including the control group, received counselling and educational materials on postpartum family planning, including information on appropriate methods for the postpartum period and a recommendation to initiate postpartum family planning 6 weeks after delivery. Because some women in the no-voucher group also got the SMS reminder and because some households share access to cell phones and may have wanted to maintain privacy around decisions about family planning, the SMS did not specifically refer to the voucher but instead read: ‘Don’t forget to review your family planning materials from Jacaranda Health’.
Data collection and outcomes
Participants were recruited in the waiting room of Jacaranda’s antenatal clinics. Eligible participants were consented into the study by providing their written consent. Participants completed a baseline survey at the antenatal clinic with questions about basic demographic characteristics and fertility preferences. Survey timing and outcome measures are defined with respect to the EDD rather than the actual delivery date in order to be consistent with the deadline and SMS intervention, which were scheduled with respect to EDD during pregnancy. Follow-up surveys were conducted by phone at 9, 12, 22, 36 and 52 weeks after EDD to assess timing of postpartum contraceptive take-up and method choice. Enumerators made multiple attempts to contact participants within a period of 3–4 weeks. Enumerators were trained to probe on the timing of contraceptive take-up if the participant did not remember the exact date with the enumerator providing assistance in estimating the date of contraceptive use. Everyone who participated in a phone survey was sent phone credit worth between US$0.46 and US$0.92 as an appreciation for participation. Data were also extracted on utilisation of care at Jacaranda from Jacaranda’s administrative database from the start of the study through June 2016 (ensuring at least 7 months of follow-up administrative data for all participants) including all information on visits to Jacaranda for family planning, any contraceptive methods received and any payments made for family planning. Finally, we kept programmatic data on the vouchers that were provided to study participants, whether vouchers were redeemed and information on when SMS reminders were sent. Additional details on data collection procedures are provided in the online supplementary technical appendix.
Our primary outcome was self-reported current use of a modern contraceptive method. Modern contraception was defined as including IUDs and intrauterine systems, implants, oral contraceptive pills, emergency contraceptive pills, condoms, injectables, patches, diaphragms/cervical caps, spermicides, vaginal rings, vaginal sponges and sterilisation. While the World Health Organization (WHO) includes LAM in their definition of modern contraceptive methods, LAM is sometimes distinguished from other modern methods28 as it can be effectively practised with no costs, facility visits or products. Evidence suggests that practice of LAM often lacks the reliability of other methods and many mothers who report practising LAM are not actually protected against pregnancy.29 The exclusion of LAM from our primary outcome of current use of modern contraception is consistent with our preregistered study outcome.
In order to understand the behavioural response to treatments, we also reported post hoc analysis on an outcome constructed from administrative data: take-up of a modern contraceptive method at Jacaranda. Self-reported survey data about take-up of contraception was preregistered as our primary outcome instead of using administrative data from the study facility because our treatments sought to increase the salience of desires around postpartum family planning, which may have led participants to seek family planning in whatever clinic was most convenient (not necessarily in the clinic where they received ANC).
We report on modern contraceptive use in the ‘short-term’ and ‘medium term’, which we define as 9 weeks and 22 weeks after EDD. These time points were chosen to be as close as possible to our first two waves of data collection in order to minimise recall bias. If we were unable to complete one of the surveys, we inferred use at that time-point from future surveys whenever possible. So, for example, for a respondent who did not complete a 9-week survey but did complete a 22-week survey, we constructed her use of modern contraception at 9 weeks based on whether she was using a method at the 22 week survey and her report about when that method use started. This method avoided losing data for inference but cannot account for discontinuation. Short-term modern contraceptive method use corresponds to a period shortly after the WHO recommendation of contraceptive take-up by 6 weeks and allowed us to observe the immediate effects of the SMS and deadline treatments. In order to understand how interventions influenced method choice, we consider a secondary post hoc analysis not included in our preregistered outcomes that examines whether study participants are using a LARC method (defined as use of an implant, intrauterine system or IUD).
Analytical approach
We estimate risk differences between treatment arms and the control group using ordinary least squares (OLS) with robust standard errors (SEs.) We use a linear model for ease of interpretation30 and estimate heteroscedasticity robust SEs to avoid bias.31 In our first model, we include a control for study phase and enrolment facility (stratification variables) in order to maximise power.32 In the fully adjusted model, we included the following additional covariates: maternal age (continuous), a binary variable indicating whether a mother was multiparous, a binary variable indicating some secondary education or higher, a binary variable indicating previous use of modern contraception, a binary variables indicating that the mother did not want future children and a binary variable indicating that her partner did not want future children, a binary variable for intention to use postpartum FP in the short-term, a continuous variable for the days between enrolment and the EDD, a continuous variable indicating travel cost to a study health facility, a binary variable indicating that the participant's residence was in the same sublocation as a study facility and a continuous variable indicating the date of study enrolment. We used case deletion for missing data and dummy-variable adjustment to account for missing covariates.33 In order to further explore patterns in our results, we construct a forest plot that compares the relationship between take-up of family planning and (1) our main interventions: receiving any SMS and receiving any voucher and (2) participant characteristics including education, self-reported intentions during ANC about take-up of postpartum family planning in the short-term. Coefficients were generated from OLS regressions of the variable of interest on the primary outcome of self-reported use of a modern method in the medium-term controlling for stratification variables (study phase and facility) with robust SEs.
Descriptive statistics on covariates were presented for the randomised sample and the sample followed to short-term and medium-term outcomes and p-values were reported for the test of differences in means between the randomised sample and the short-term and medium-term analysis samples. We report on two measures of treatment fidelity using programmatic data: whether the voucher that was randomly assigned was provided to the study participant and whether an SMS was sent within 1 week of the scheduled time (5 weeks after EDD). We also presented descriptive statistics on voucher redemptions, the monetary value of methods received using the voucher and the timing of voucher redemptions using programmatic data. We also presented descriptive statistics on method type, location, cost and timing for the first modern method initiated among the sample of participants ever reporting that they initiated a modern method in any of our surveys. We presented robustness checks in online supplementary tables, including separate estimates for the two study phases of data collection, estimation of our main results with LAM included in the definition of modern method use and estimation of our main results using multiple imputation for individuals with missing outcome data. In order to understand concordance between self-reported survey data and administrative data, we report comparisons of the rates of agreement between survey and administrative data for the primary outcomes among the short-term and medium-term analysis samples, including an analysis of the reported location where care was received among those reporting use of a modern method. We also present the distribution of methods obtained in each treatment arm for those self-reporting use of modern method in the medium term using a stacked bar graph.
Ethics
This study was approved by Institutional Review Boards at Harvard T. H. Chan School of Public Health and the Ethical and Scientific Review Committee of Amref Health Africa (AMREF) in Nairobi, Kenya. The study design was registered at socialscienceregistry.org with identification number AEARCTR-0000320.
Results
Of the 686 study participants enrolled in the study, we followed 78% of the sample (537 respondents) to collect data on the short-term outcomes with 17% of responses from the 9-week survey, 79% of responses from the 12-week survey and 3% of responses from the 22-week, 36-week or 52-week survey. We observe 61% of the sample to collect data on the medium-term outcomes (418 respondents), with 90% of outcomes constructed using the 22-week survey, and 10% of responses constructed using the 36-week or 52-week survey. The short-term and medium-term contraceptive use outcomes correspond to a mean of 63 days after actual delivery (95% CI 62 to 64) and 154 days after actual delivery (95% CI 153 to 155) among our study participants.
We present characteristics of the study sample in table 1. Sixty-seven per cent of participants report having used modern contraceptive methods in the past. Thirty per cent of respondents report not wanting any more children, while 21% reported that their male partners did not want more children. Thirty-two per cent of study participants reported during their pregnancy that they hoped to start using modern contraceptive methods by the short-term outcome time-point defined in our analysis. Women were an average of 42 days from their EDD at the time of enrolment. The average participant had travelled 30 min to arrive at the maternity clinic for care. Characteristics of the enrolment sample and the sample reached for the short-term and medium-term contraceptive use outcome were similar. We report descriptive statistics separated by treatment arm for the randomised sample (online supplementary table S3a), short-term sample (online supplementary table S3b) and medium-term sample (online supplementary table S3c). In online supplementary table S4, we present rates of follow-up surveys by treatment arm and phase. Rates of follow-up on primary outcomes tended to be slightly lower in the control arm, but characteristics of the follow-up samples were largely balanced across treatment arms.
Baseline characteristics of randomised and surveyed samples
We present information about treatment fidelity, redemption of study vouchers and take-up of postpartum contraception in table 2. The vast majority of participants received the treatment they were assigned to receive, with 98% of those assigned to receive a voucher receiving the correct voucher and 95% of those assigned to receive an SMS being sent an SMS within 1 week of the scheduled time. Twenty per cent of study participants assigned to receive a voucher for free contraception redeemed the voucher at study clinics. Among self-reported users of modern contraceptive methods who report currently using a LARC method by the short-term follow-up, 42% redeemed their voucher, while just 17% of users who chose a non-LARC method redeemed their voucher. The value of the average voucher redeemed was $4.26. The average value of the voucher redemption for LARC methods was $4.92 and for non-LARC methods was $2.59. Among all those who redeemed a voucher, the average number of days between EDD and redemption of the voucher was 71 days.
Descriptive statistics of contraceptive use
At first postpartum contraceptive initiation, the most common methods were implant (32%), injectables (27%) and contraceptive pills (27%). Thirty-seven per cent of participants reporting modern contraceptive use first initiated contraceptive methods at the private clinic where we enrolled study participants, while others accessed contraceptive methods at a public facility (27%), other private facility (21%) or ‘chemist’/pharmacy (15%). At first postpartum use of modern contraception, the average user paid US$1.50. The average time-period between EDD and initiating modern contraceptive use was 83 days for participants who initiated contraception during the study follow-up period.
The impact of the interventions on self-reported contraceptive take-up and timing from participant surveys was presented in table 3. In the control group, 32% of the sample was using modern contraceptive methods at the short-term time-point, and 58% of participants were using modern contraceptive methods at the medium-term time-point. None of the interventions had a statistically significant impact on the likelihood of using modern contraception in the short term. The estimated effects of standard voucher combined with SMS (12 percentage points (pp), 95% CI −5 pp to 30 pp) and deadline voucher combined with SMS (11 pp, 95% CI −9 pp to 31 pp) on short-term contraceptive use were large and positive, but the estimates are imprecise. By the medium-term time-point, the probability of using modern contraception for those who received a standard voucher with SMS was 25 pp higher than the control arm (95% CI 6 pp to 44 pp). The estimated impact of the SMS alone was also large, though the CI is imprecise (16 pp, 95% CI −6 pp to 38 pp). None of the other treatment arms were estimated to statistically significantly increase the likelihood of modern contraceptive use in the medium-term.
Ordinary least squares (OLS) model estimates of treatment effects on self-reported postpartum utilisation of modern contraception
We found that 13% of the control sample reported initiating LARC in the short-term time-point, while 27% of the control group reported initiating by the medium-term time-point (bottom rows of panels A and B of table 3). We did not see evidence of statistically significant impacts of any of the interventions in terms of short-term use of LARC. We found that the standard voucher combined with SMS increased the likelihood of taking up LARC in the medium term by 20 pp compared with the control group (95% CI 0 pp to 41 pp), though the estimated CI is imprecise. None of the other treatment arms statistically significantly increased the likelihood of modern contraceptive use, or LARC methods in the medium term.
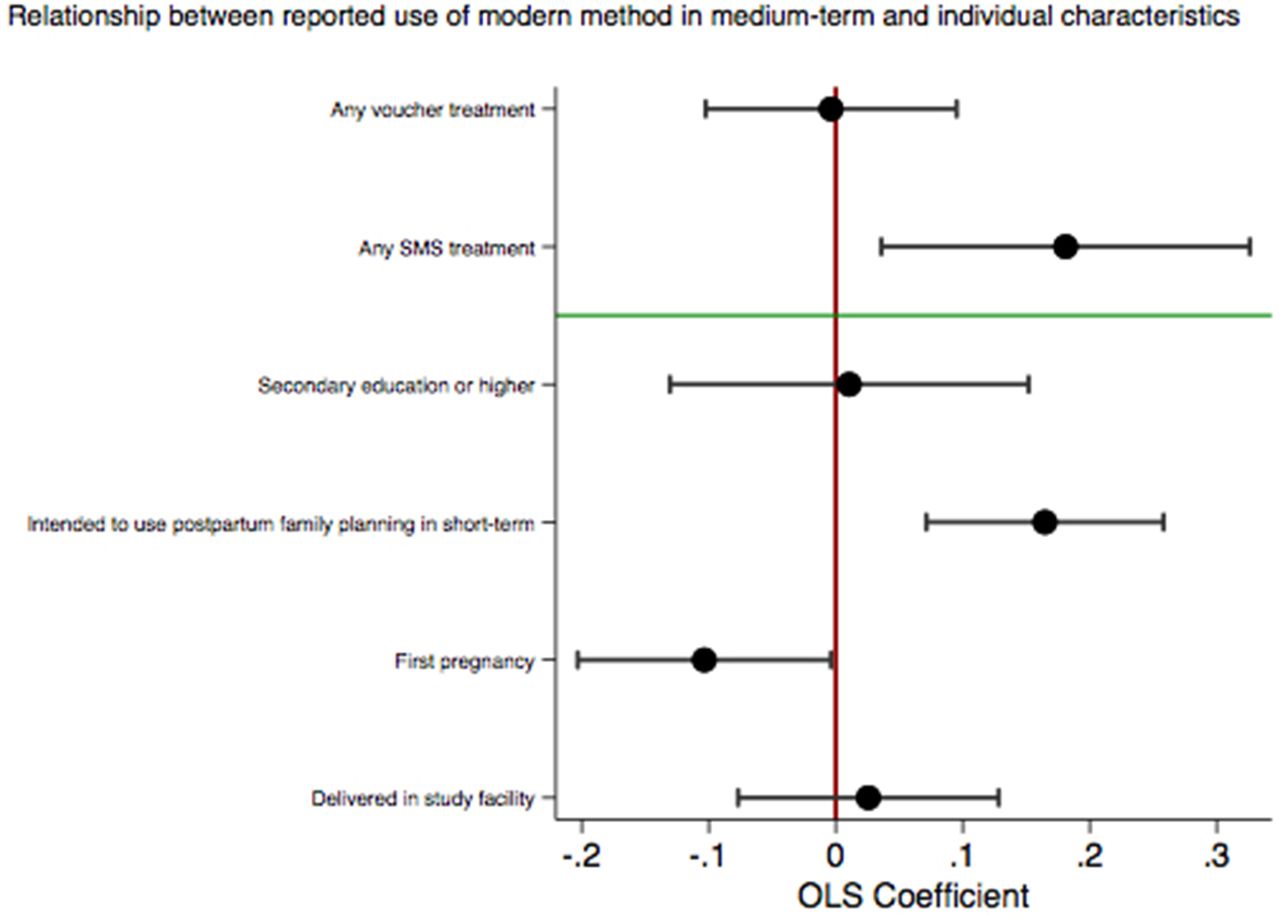
We see that across most models, estimated treatment effects for arms assigned to receive SMS were higher than those not receiving SMS. Figure 1 presents a forest plot demonstrating relationships between pooled treatments and individual characteristics and take-up of modern methods in the medium-term. We did not see evidence that those receiving vouchers were more likely to report using contraception in the medium term than those who did not. Individuals assigned to receive any SMS were 19 pp more likely to report using contraception in the medium term than those who did not (95% CI 4 pp to 33 pp). We found that individuals who report an intention to start family planning in the short term were 16 pp more likely to report using family planning in the medium term (95% CI 7 pp to 26 pp) and that individuals who were pregnant for the first time at baseline were 10 pp less likely to report contraceptive use (95% CI −20 pp to −0.3 pp). Participant’s education and delivery in a study facility were not associated with self-reported take-up of modern methods.

{kind=link}
Forest plot of pooled treatments and individual characteristics on self-reported medium-term contraceptive use. OLS, ordinary least squares; PP, percentage point.
We consider the impact of treatments on receiving a modern contraceptive method from the study clinic using data from administrative records in table 4. Thirteen per cent of study participants in the control group had received a modern method by the short-term follow-up window and 21% had received a modern method by the medium-term follow-up window. Though treatments combining vouchers with SMS tend to have higher estimated probabilities of receiving a modern method and the estimated impact is largest in the standard voucher with SMS arm, the CIs were imprecise and estimated impacts were not statistically significantly different from the control groups.
Ordinary least squares model estimates of treatment effects on postpartum receipt of modern contraception from study facility (administrative records)
We conducted sensitivity analyses in online supplementary table S5 (results with primary outcomes separated by phase), online supplementary table S6 (results with outcomes from administrative data separated by phase), online supplementary table S7 (results including LAM) and S8 (with multiple imputation for missing outcome). We observed similar patterns of results across these sensitivity analyses, though estimated effects using multiple imputation were quite imprecise. We present a comparison of self-reported and administrative data outcomes in online supplementary table S9. In online supplementary table S10, we reported descriptive statistics on the average take-up of specific methods across treatment arms.
Discussion
We found that that the combination of free contraception and an SMS reminder increased take-up of modern contraceptive methods in the postpartum period. There are a number of reasons why combining a voucher for free contraception with an SMS reminder may have increased take-up. It may be because the combination of the voucher and SMS addressed both cost and behavioural barriers to take-up. The likelihood of redeeming the voucher for free contraception was higher among participants who used a long-acting reversible method compared with other methods, suggesting that the voucher may have been especially helpful among women interested in using LARC. This could be because LARC methods typically come at higher out-of-pocket cost and are not always available in public facilities without trained providers.34 It could also be the case that, in addition to relaxing cost constraints, the voucher increased the salience of the need for postpartum family planning, in particular when combined with the reminder that draws attention to the voucher. Unfortunately, our data did not allow us to identify the precise mechanism by which the combination of vouchers and SMS reminders increased take-up.
In our study, the provision of a voucher for free contraception alone was not sufficient to increase take-up of modern methods. While the majority of our sample was using a modern method by the medium-term time-point, overall redemption rates of the voucher were low (20%), and the estimated impacts of treatments on acquiring contraception in the study clinics were small and statistically insignificant. The limited use of vouchers in our study is consistent with findings from other evaluations of voucher programme.17 This may be because women can receive contraception from a variety of locations, including private facilities, retail outlets and public facilities (where Kenya’s national policy is to provide postpartum contraception for free). Some women may decide to receive postpartum contraception in the facility where they delivered their baby or where they take their child for immunisation. Indeed, nearly two-thirds of those who ever report use of a modern method received their first postpartum modern method from a location other than the study facility where they enrolled during ANC.
We also found that those who received SMS reminders were more likely to take-up modern methods in the medium-term than those who did not. It is somewhat surprising that the SMS reminder seems to have had more influence in the medium term than it does in the short term (immediately after messages were sent). It may be that the SMS reminder increased the salience of desires around birth spacing and postpartum family planning but participants were not immediately able to act that the response was not immediate due to the need to confer with partners, develop a plan for visiting a facility or other factors.
Our evidence also suggests that not all behavioural nudges are effective in increasing postpartum contraceptive take-up. We find limited evidence that incorporating a deadline to use the voucher drives either early or eventual take-up of modern postpartum contraceptive methods. While our deadline was chosen to occur after the recommended initiation timing of postpartum contraception at 6 weeks by the WHO, it may nonetheless have been sent earlier than many women were ready to consider modern methods, particularly LARC methods. Reminders offer greater flexibility than a strict deadline,35 and this flexibility may be especially appropriate in the context of the many demands of the postpartum period.
Our experiment has important limitations. This was a pilot study with a modest sample size that was further limited by attrition. Attrition in this study was driven by the highly mobile nature of this urban population and the fact that we were attempting to contact women at a time when they were caring for a new baby. We demonstrated that demographic characteristics of the sample we were able to follow were not significantly different from the enrolled sample and that our findings were qualitatively similar when we use multiple imputation to infer missing outcome data. Another limitation of our study is that we relied on self-report of take-up and timing of postpartum contraceptive use for our primary outcome. As self-reports of contraceptive use are costly and onerous to verify, there is limited rigorous evidence of the validity of self-reported contraceptive use.36 In our study, we generally see consistency across self-report outcomes and outcomes from administrative data. We surveyed new mothers at high frequency in the postpartum period in order to avoid relying on long recall periods to reconstruct the timing of their use of postpartum family planning. While social desirability bias is a significant problem in many studies of contraceptive take-up that rely on self-reports,37 74% of participants in our study report at baseline that they plan to use family planning at some point in the postpartum period, suggesting high acceptability of postpartum contraception in this population.
Finally, our study sample draws only from women who have attended ANC in two private maternity facilities located in the informal settlements of Nairobi who have access to a cell phone. An estimated 84% of adults living in Nairobi own a cell phone, suggesting that we are unlikely to exclude a significant portion of our sample based on access to a cell phone within their household.38 Within our selected sample, we find similar but slightly higher rates of postpartum contraceptive use compared with a previous study in Nairobi’s informal settlements.39
International efforts to increase access to postpartum contraception have focused on designing voucher programmes that decrease or remove the cost of modern contraceptive methods to users. Evidence that a voucher for free contraception is not enough to increase take-up, but a free voucher combined with a simple reminder can significantly increase take-up of modern contraception has implications for the design of voucher and transfer programme. Voucher programmes should consider how to design financial supports in a way that accounts for potential behavioural frictions in the postpartum period.
There is relatively little prior evidence on the impact of reminders on contraceptive take-up in general and in the postpartum period in particular.40 Our study provides some of the first evidence from a randomised controlled trial to evaluate the impact of SMS reminders on contraceptive use. Our evidence fills an important gap in the literature on delivery strategies for promoting postpartum family planning in sub-Saharan Africa.41 Furthermore, we provide evidence on strategies to improve utilisation of postpartum contraception among a population of urban poor, helping to close the gap in knowledge, improving contraceptive take-up across socioeconomics groups42 and ensuring equity of access to modern contraception.
Conclusion
Despite significant health risks to mother and baby of closely spaced births and substantial desire to improve birth-spacing, take-up of modern contraceptive methods remains low in the postpartum period. We find that combining a behavioural nudge (an SMS reminder) with a voucher for free postpartum contraception increases the take-up of modern methods. Our study highlights the need for policy makers to consider multiple different kinds of barriers to the take-up of contraceptive methods in the postpartum period.
References
Footnotes
Handling editor Seye Abimbola
Contributors MM designed the study, secured funding for the study, designed data collection tools, performed data analysis, drafted the manuscript and edited the manuscript. CWR designed data collection tools, fielded the study, performed data analysis and reviewed the manuscript. AE and FM designed data collection tools, fielded the study and reviewed the manuscript. JC designed the study, secured funding for the study, designed data collection tools, contributed to data analysis, contributed to drafting and editing manuscript and reviewed the manuscript.
Funding We gratefully acknowledge funding from the William and Flora Hewlett Foundation (Grant number2014-9962). This project was also made possible through the generous support of the Saving Lives at Birth partners: the United States Agency for International Development (USAID), the Government of Norway, the Bill & Melinda Gates Foundation, Grand Challenges Canada, the U.K. Department for International Development (DFID), and the Korea International Cooperation Agency (KOICA). It was prepared by the authors and does not necessarily reflect the views of any funders.
Competing interests None declared.
Patient consent Not required.
Ethics approval This study was approved by Institutional Review Boards at Harvard T H Chan School of Public Health and the Ethical and Scientific Review Committee of Amref Health Africa (AMREF) in Nairobi, Kenya.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data from this manuscript are not available to share at this moment. Interested researchers should contact the corresponding author.