Article Text

Abstract
US adults visit eye care providers more often than primary healthcare providers, placing these doctors in a prime position to help identify and manage patients with prediabetes and diabetes. Currently, diabetes is identified in eye clinics in an advanced stage, only after visible signs of diabetic retinopathy. Recent ophthalmic research has identified multiple subclinical and clinical changes that occur in the anterior segment of the eye with metabolic disease. The corneal epithelium exhibits increased defects and poor healing, including an increased risk of neurotrophic keratitis. Increased thickness and stiffness of the cornea artificially alters intraocular pressure. There is damage to the endothelial cells and changes to the bacterial species on the ocular surface, both of which can increase risk of complications with surgery. Decreased corneal sensitivity due to a loss of nerve density predispose patients with metabolic disease to further neurotrophic complications. Patients with diabetes have increased Meibomian gland dysfunction, blepharitis and reduced tear production, resulting in increased rates of dry eye disease and discomfort. Early detection of metabolic disease may allow eye care providers to be more proactive in recommending referral and intervention in order to reduce the risk of blindness and other diabetes-related morbidity. Continued research is needed to better understand the time course of changes to the anterior segment and what can be done to better detect and diagnose patients with prediabetes or undiagnosed diabetes and provide improved care for these patients.
- cornea
- type 2 diabetes
- clinical care
- prediabetes
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Obesity, prediabetes and diabetes are growing exponentially—worldwide, and especially in the USA.1 The effect of diabetes on the retina has been well classified, but there is growing research on the profound effects of metabolic disease on the front of the eye. In the USA, adults visit eye care providers more often than primary healthcare providers, placing eye doctors in a prime position to lead the care and research in this area.2 Unfortunately, diabetes is often first diagnosed in eye clinics in an advanced stage, only after visible signs of diabetic retinopathy appear. Standardized, non-invasive, early detection tests in an eye care setting could help to reduce the risk for disease onset and/or progression. The purpose of this paper is to summarize the current state of knowledge on the clinical outcomes of obesity, prediabetes and diabetes on the ocular surface, and explore new research which may someday be applied to help identify and better refer patients with undiagnosed prediabetes and diabetes.
Clinical and subclinical changes to the ocular surface
New research has identified multiple clinical and subclinical changes that occur in the anterior segment of the eye with dysregulation of insulin and glucose. These alteration can lead to poor or fluctuating vision, increased risk of inflammation and subclinical complications with contact lens wear or ocular surgery and pain and discomfort. The following section reviews changes to the cornea, conjunctiva, eyelids and tear system and are summarized in table 1.
Ocular surface changes associated with obesity, prediabetes and diabetes
Cornea
The human cornea is a five-layer structure, comprising an endothelial layer, Descemet’s membrane, stroma, basement membrane and epithelium. The cornea is about 540–560 µm thick centrally, and increases by about 100 µm in the periphery. Central thickness increases by about 10–30 µm in patients with type 1 or type 2 diabetes, including well-controlled patients with diabetes with hemoglobin A1c (A1c) <7.3 Duration of diabetes is correlated with increasing corneal thickness.4–7 It has been hypothesized that the increase in thickness may be due to increased glucose levels in the tissue and the formation and accumulation of advanced glycation end products (AGEs).5 7–9 Two small population-based studies found no correlation between obesity and corneal thickness10 11; however, one study reported significant associations between corneal thickness and body weight, body mass index (BMI), fasting plasma glucose (FPG) and 2 hours plasma glucose (PG).12 An increase in corneal thickness associated with obesity and prediabetic blood glucose levels are in line with the model of obesity and diabetes being a continuum of metabolic disease.12
The corneal endothelium is a single layer of uniform hexagonal squamous cells. The corneal endothelium regulates water and solute transport, including glucose, between the aqueous humor and cornea in order to maintain corneal transparency and thickness. Hyperglycemia can cause direct oxidative damage and reduce the activity of Na+/K+-ATPase activity.8 Corneal endothelial cell density is reduced by about 100–400 cells/mm2 in patients with both types 1 and 2 diabetes compared with age-matched controls.4 5 8 13 14 The decrease in density leads to changes in cell shape (pleomorphism) and size (polymegathism).4 8 13 14 Duration of diabetes disease is well correlated with endothelial cell density loss, polymegathism and pleomorphism.5 13
The cornea naturally auto-fluoresces at a wavelength of about 515–630 nm when excited with 415–490 nm light due to endogenous fluorophores.15 16 Corneal auto-fluorescence increases in type 1 and 2 diabetes, likely due to the increase in AGEs.16 Corneal auto-fluorescence has been correlated with duration of disease, severity of diabetic retinopathy and A1c levels and has been suggested to be a good non-invasive indicator of the metabolic state of the cornea.16 17
The corneal stroma accounts for the majority of the corneal thickness (~90%) and thus its physical and biomechanical properties. Hyperglycemia and associated accumulation of AGEs lead to crosslinking of the stroma which increases the corneal stiffness.9 Patients with type 1 and type 2 diabetes have been shown to have increased corneal hysteresis, or viscosity, of the cornea as measured by resistance to deformation by air puff.6 7 18 Corneal hysteresis is also associated with the duration of disease and A1c levels.7 18 Increased corneal thickness and stiffness in patients with diabetes can lead to an overestimation of intraocular pressure (IOP),7 19 which may lead to a misdiagnosis of glaucoma.
The cornea is the most densely innervated tissue in the body, with about 7000 nociceptors/mm2 at its center.20 Corneal nerves derive from the nasociliary branch of the ophthalmic division of the trigeminal nerve (cranial nerve V), enter through the anterior stroma as small unmyelinated nerve fibers and then branch upward to penetrate basement membrane layer, form the subbasal nerve plexus and terminate in the epithelium.20 Corneal nerves regulate wound healing and modify the lacrimal response, and are critical to ocular surface integrity.21 Corneal subbasal nerves can be imaged non-invasively with in vivo confocal microscopy. Corneal subbasal nerve fiber length, density and branching are reduced with type 1 and 2 diabetes (figure 1).22–25 The decrease in corneal nerve fiber length and density has been well correlated with diabetic peripheral neuropathy24 25 and autonomic neuropathy.26 Due to the nerve and other ocular surface damage, up to 70% of patients with diabetes have some form of keratitis ranging from superficial punctate keratitis to recurrent corneal erosions and neurotrophic ulcer27–29 (figure 2). Corneal nerve fiber length was predictive of a diagnosis of peripheral neuropathy in patients with diabetes, with a cut-off point of 12 mm/mm2.30 Importantly, corneal nerve health was shown to improve with improved glucose control for patients with either type 1 or type 2 diabetes.31 32
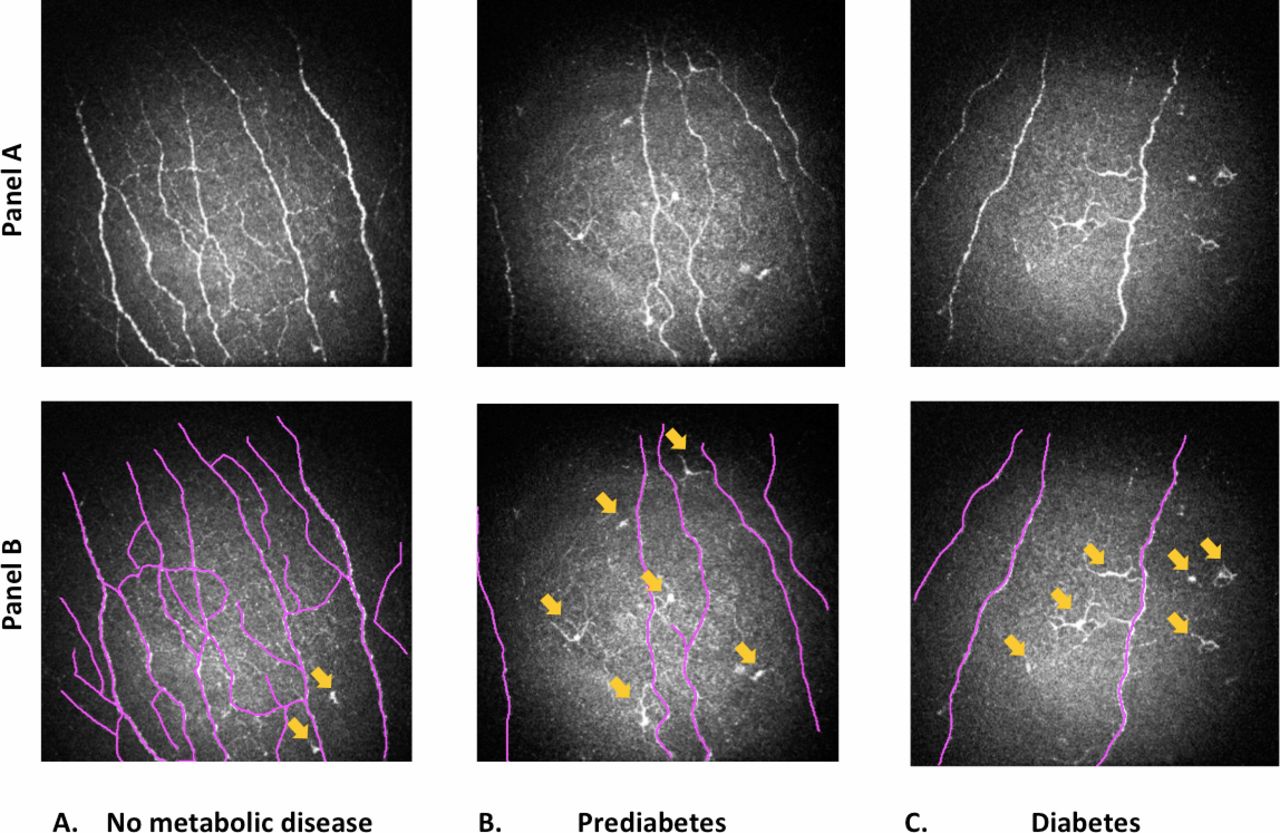
In vivo corneal confocal images (400×400 µm2) demonstrating patients with (A) no metabolic disease, (B) prediabetes and (C) type 2 diabetes (panel A) at the central cornea. Corneal subbasal sensory nerves are highlighted in purple in panel B with calculated densities of 3964 µm, 1691 µm and 1012 µm per 400×400 µm2 in patients with no metabolic disease (A), prediabetes (B) and diabetes (C), respectively (Richdale and Harrison, unpublished data). Yellow arrows indicate corneal epithelial dendritic cells and show a higher density in patients with prediabetes and diabetes (6 cells/frame) compared with those with no metabolic disease (2 cells/frame). All subjects were 54–59 years of age with no history of contact lens wear. Photo credit: Labs of Kathryn Richdale, OD, PhD and Wendy Harrison, OD, PhD, College of Optometry, University of Houston, Texas, USA.
{kind=link}
{kind=link}
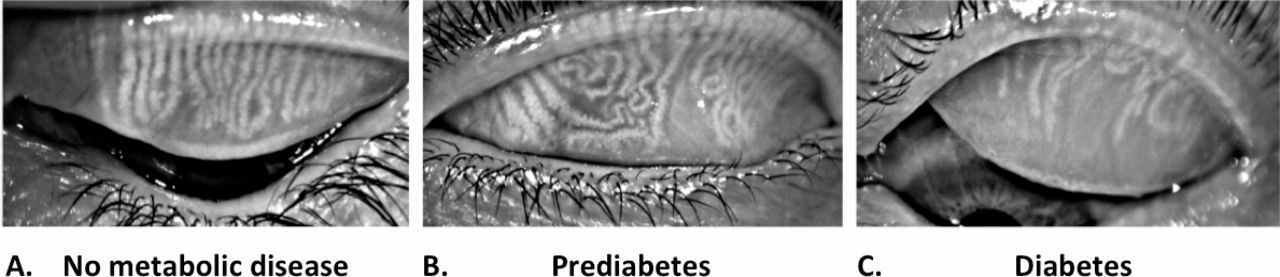
Images demonstrating patients with Meibomian gland dropout using the keratograph in patients with (A) no metabolic disease, (B) prediabetes and (C) type 2 diabetes (Richdale and Harrison, unpublished data). All subjects are 51–59 years of age with mild-to-moderate dry eye symptoms and did not wear contact lenses. Photo credit: Labs of Kathryn Richdale, OD, PhD and Wendy Harrison, OD, PhD, College of Optometry, University of Houston, Texas, USA.
Corneal sensitivity to mechanical pressure, temperature and chemicals stimuli is a measure of corneal nerve function.33 More than 50% of the patients with diabetes show reduced sensitivity as a result of damage to corneal sensory nerve.34 All three types of sensitivity are reduced in patients with long-term type 1 and type 2 diabetes.23 35 Decreases in mechanical sensitivity measured by non-contact esthesiometer were noted shortly after diagnosis of type 2 diabetes, but were somewhat delayed for those with type 1 diabetes, which also mimics patterns seen in peripheral neuropathy.35
Corneal epithelial dendritic cells are antigen-presenting cells located in and around the corneal subbasal epithelial layer and initiate the immune response to infectious or inflammatory agents.23 36 Dendritic cells are critical for proper corneal epithelial wound healing.37 These cells can be identified by their morphology in vivo with confocal microscopy (figure 1). There is an increase in central dendritic cell density in patients with type 1 and 2 diabetes compared with healthy controls.22 38 Dendritic cell density has also been found to be inversely related to corneal nerve fiber density,22 38 indicating that there may be a neuro-immune interaction in the development of the neurotrophic keratitis.
The corneal epithelium is about 50 µm thick with layers of squamous, intermediate (wing) and basal cells, which are attached to the underlying basement membrane by hemidesmosomes. In vivo confocal microscopy has been used to measure the density of intermediate and basal epithelial cells in diabetes. The epithelial cell density is reduced in patients with type 1 and type 2 diabetes, with each year of diabetes corresponding to a decrease of about 10–25 cells/mm2.39 40 The corneal basement membrane also becomes thicker and less regular, and junctions between cells are weakened in diabetes.28 41 There are direct and indirect effects of changes in glucose and insulin on the structure and metabolism of the corneal epithelium.42 In brief, hyperglycemia alters the expression of growth factors and mediators secreted by corneal epithelial cells, leading to a cyclic disruption in cell growth, migration and integrity.42 Early research suggested that the corneal epithelium does not require insulin for uptake of glucose43; however, recent research using human telomerized corneal epithelial cells in culture suggests that insulin plays a key role in mediating epithelial cell metabolism and homeostasis.44
Although the early effects of obesity or prediabetes on corneal health have not been well explored, given the continuum of diseases seen in other aspects of the body, it is likely that the structure and function of the entire cornea is altered before the diagnosis of diabetes. Further research is needed to fully understand the potential effects of early disease states on corneal health. One major gap pertains to the possible ability of interventions that reverse glucose dysregulation, in either people with prediabetes or obesity, to improve corneal nerve health and adverse immune response, which could lead to improved corneal wound healing and reduce the risk of further damage. Some lifestyle strategies, such as increased physical activity and diet, can rapidly reduce glucose levels and postprandial insulin before and independent of weight changes. Thus, it will also be important to understand the time course of disease development for corneal health. The progression from impaired glucose tolerance or fasting hyperglycemia on through diagnosed diabetes may indicate that some of the ocular pathology occurs sooner in the spectrum of disease than the classical clinical symptoms or retinal signs at the diagnosis of diabetes. And because of this, it follows that there is a need to know if there is also a rapid attenuation or reversal in the anatomy and physiology in the eye, as there might be for adaptations in the peripheral vasculature.
Tear film, conjunctiva, eyelid and Meibomian glands
The ocular surface produces lipid, aqueous and mucin, to make up the tear film, which is then spread by the eyelids and serves to protect and maintain the health of the ocular surface. The aqueous layer is primarily produced by the lacrimal and accessory glands. Mucins are secreted by the conjunctival goblet cells and corneal epithelial cells. Lipids are secreted from the Meibomian glands, which are located in the eyelids.
The International Dry Eye Workshop (DEWS) II report classified diabetes as a risk factor for aqueous-deficient dry eye disease, although it may also have an evaporative component.45 46 Patients with type 1 and 2 diabetes have been shown to have a faster tear break up time, decreased tear production and volume, higher tear osmolarity and greater rates of Meibomian gland dysfunction (figure 2).24 47–50 The ocular surface is further compromised in patients with more severe and longer duration of diabetes disease, including those with higher A1c values, or retinopathy or peripheral neuropathy.24 51 Patients with obesity (average BMI 38.2±5.8), most of whom would also have been classified as having prediabetes (FPG 108.2±14.1), also showed increased conjunctival metaplasia and goblet cell loss compared with healthy controls.52 Via a retrospective medical record review, patients with diabetes were more likely to have a diagnosis of blepharitis (type unspecified) compared with controls.53 The etiology and pathogenesis of reduced tear function in patients with diabetes is likely due to both microvascular and neuropathic changes in lacrimal and Meibomian glands, in addition to reduction in reflex tearing due to decreased corneal sensitivity and nerve dysfunction.45 54
Patients with type 1 and 2 diabetes may also have more conjunctival hyperemia, due to a dilation of the large conjunctival vessels.55 56 At the same time, the smaller capillary vessels have been found to decrease in diameter in patients with diabetes.55 The increase in conjunctival microvasculopathy was identified even prior to the onset of clinical retinopathy.56 Further testing is needed to understand the relationship between conjunctival and retinal microvasculopathy but, due to the non-invasive nature of the testing, conjunctival microvascular testing could be a useful screening tool for early diabetic retinal disease.56
A detailed review of tear components modified by diabetes and other diseases has been published elsewhere and is beyond the scope of this paper.57 But, in brief, many tear inflammatory mediators and neuropeptide (eg, substance P) are altered in diabetes but there are no significant changes in the main tear proteins, including lactoferrin, albumin, lipocalin, lysozyme and secretary IgA.58 59 Tear glucose levels also are higher in patients with type 1 or 2 diabetes under both fasting and fed conditions compared with healthy controls.60–62 Tear glucose levels are about 10 times lower but well correlated with blood glucose levels, after allowing approximately 20–25 min for equilibration.60 61 63 Average tear glucose concentration of patients without diabetes range from about 0.05 to 0.5 mM (0.89–8.9 mg/dL), and 0.5 to 5 mM (9.0–89.3 mg/dL) for patients with diabetes.60 63 Unfortunately, there is no known report of tear glucose levels for patients with prediabetes. Insulin is critical to maintaining the health of the cornea, lacrimal glands and Meibomian glands.42 54 64 However, there is only one study which reported insulin levels in human tears. Rocha et al found that insulin levels in stimulated tears of patients without diabetes were approximately 0.20 ng/mL (69 pmol/L) under fasting conditions and increased to 0.60 ng/mL (103 pmol/L) after a meal.65 Insulin levels in tears of patients with diabetes, prediabetes or obesity have not been reported. In general, insulin-like growth factor binding protein 3 (IGPBP3) binds to insulin-like growth factor-1 in order to activate the cell apoptosis and antiproliferation.39 66 Since the expression of IGPBP3 was found to be greatly increased in patients with type 2 diabetes, compared with controls and was negatively correlated with corneal nerve fiber length, it has been proposed that IGPBP3 plays an important role in corneal epithelial and nerve health in type 2 diabetes.39 66 There was a similar, although not statistically significant trend for patients with type 1 diabetes.66
The predominant microbial species identified on the healthy ocular surface are Corynebacterium, Staphylococcus, Streptococcus, Acinetobacter and Pseudomonas.67 High glucose levels in the tears and increased ocular surface inflammation with diabetes support increased microbial growth.68 Using traditional culture techniques, greater frequency of Escherichia coli, Klebsiella pneumoniae and enterococci have been identified on the ocular surface of patients with diabetes compared with healthy controls.69–71 Higher positive culture rates and greater bacterial diversity were associated with increasing severity and duration of diabetes disease, respectively.70 72 Using 16 s rRNA analysis, patients with type 2 diabetes were found to have greater bacterial diversity and increased abundance of Acinetobacter, Pseudomonas, Burkholderia, Sphingomonas and Ralstonia compared with healthy controls.68 73 Patients with type 1 and type 2 diabetes have been shown to have an increased risk of acute bacterial conjunctivitis.53 74 Further research in larger and more diverse populations is needed to fully understand the effects of these diseases on the ocular surface microbiome and risk for ocular inflammation.
Eye care for patients with diabetes and at-risk populations
The American Optometric Association and the American Academy of Ophthalmology recommend that patients with diabetes receive a comprehensive eye exam at diagnosis of type 2 diabetes or 5 years after diagnoses of type 1 diabetes, and then annually thereafter.75 76 Patients with diabetic retinopathy should be seen more frequently.75 76 There are no specific guidelines for patients with prediabetes or obesity. Therefore, one of the pressing needs for more research is to define the time course of the ocular pathological changes prior to diabetes diagnosis. As discussed in the previous section, identifying potential metabolic disease changes earlier may allow for treatment and possible reversal of pathological processes which could have a significant impact on ocular and overall systemic health and quality of life.
According to US optometry and ophthalmology guidelines, care of the patient with diabetes is focused on diagnosing and managing retinal complications.75 76 Currently, the recommendations for anterior segment complications associated with diabetes are to monitor and manage as usual and customary as there are no disease-specific treatments.76 Epithelial defects and dry eye disease can be managed with ophthalmic lubricants, punctal plugs, prescription topical or oral medications, autologous serum, amniotic membranes or lid closure.46 Bandage or scleral contact lenses may be used with caution due to increased risk of infections. Non-steroidal anti-inflammatory drugs should be avoided in these patients due to the possibility of corneal perforation.20 Some experimental treatments have begun to be evaluated in early human case reports and trials. Despite a lack of understanding of the normal levels of insulin in non-diabetic and diabetic tears, it has been shown that the use of topical insulin improved time to wound healing, compared with standard treatment of antibiotic and steroid, following corneal debridement during vitreoretinal surgery in patients with diabetes.77 78 Thymosin beta4 (β4) has multiple regenerative properties and has been used to heal pressure and venous stasis ulcers and improve dry eye signs and symptoms.79 80 Thymosin β4 has also been suggested to promote wound healing in a case series of patients with diabetes.81 82
There is only one Food and Drug Administration-approved treatment for neurotrophic keratitis, the most severe type of keratitis caused by corneal nerve damage, Oxervate (cenegermin). Oxervate is a recombinant human nerve growth factor, was found to improve neurotrophic keratitis in 70% of patients compared with placebo (28%).83 However, it is a costly treatment and may not be accessible to all patients. Current research is also exploring the potential use of aldose reductase inhibitors, opioid growth factors, hepatocyte growth factors and other topical therapies for neurotrophic keratitis.20 84 Unfortunately, the standard of care for patients with anterior segment complications of diabetes is still mainly palliative, based on symptoms, and uses therapies researched mostly on patients without diabetes.
The effects of contact lens wear and diabetes have been carefully reviewed by O’Donnell and Efron and Bussan and Robertson.85 86 Patients with diabetes who wear soft contact lenses had about 130 cells/mm2 fewer endothelial cells than patients with diabetes who do not wear lenses,4 which is a 4%–5% greater loss of endothelial cells for patients with diabetes compared with healthy adults. Patients with diabetes who do not wear contact lenses had about 370 endothelial cells/mm2 less than healthy non-contact lens wearers.4 This suggests that patients with diabetes who wear soft contact lenses long-term may suffer further endothelial compromise than either factor alone.4 87 Rigid gas permeable contact lenses offer improved oxygen transmission and reduced risk of infections thus should potentially offer patients with diabetes improved outcomes. However, there is limited research beyond clinical observations of the potential complications of rigid contact lens wear in patients with diabetes.85 86 The current US ophthalmic guidelines do not preclude contact lens wear for patients with diabetes. Nevertheless, eye doctors are encouraged to educate patients with diabetes on the increased risk of complications and more frequent follow-up is recommended due to poorer wound healing, reduced corneal nerve function, decreased endothelial cell density and changes in the ocular microbiome,4 75 which may lead to contact lens indicated corneal infiltrative events.
Patients with diabetes may be at increased risk of complications during and after ocular surgery. Patients with diabetes suffer about 4%–6% greater endothelial cell loss after cataract surgery, with greater cell loss being reported in patients with longer duration of disease.14 88 89 Fortunately, the additional cell density loss did not seem to affect visual acuity.88 89 Patients with diabetes have higher rates of incomplete wound healing after laser-assisted keratomileusis (LASIK).90 Due to unstable refractive error associated with hyperglycemia, patients with uncontrolled diabetes have worse refractive outcomes.91–93 Halkiadakis et al reported no significant difference in clinical outcomes for patients with diabetes with good glycemic control undergoing LASIK.94 The American Academy of Ophthalmology considers uncontrolled diabetes an absolute contraindication, but well-controlled diabetes a relative contraindication for refractive surgery.91 Further research is needed to fully understand the effects of metabolic disease on postsurgical pain and wound healing.
The Eye Bank Association of America does not require indicating diabetes as a possible contributing factor to donor death, and historical data suggest that donor corneas from patients with reported diabetes is not a risk factor for penetrating keratoplasty failure.95 However, a recent study found that donor corneas from patients with obesity and diabetes were more likely to lead to graft failure in Descemet Membrane Endothelial Keratoplasty surgery.96 97 Thus, continued research is needed to fully understand the risks for patients who are recipients of corneas from donors with metabolic disease.
Summary of limitations in research and clinical care
Research in diabetes in the eye has historically been focused on the retina. More recently, researchers have begun to explore the effects of type 1 and 2 diabetes on the anterior segment of the eye and revealed significant structural and functional alterations, including dry eye disease, even early in the disease process. Population-based studies would be required to confirm the effect of diabetes on dry eye. Corneal subbasal nerves are readily imaged with in vivo confocal microscopy and able to reveal early neuropathy and regeneration with treatment. Corneal auto-fluorescence and tear protein and neuropeptide levels may be other non-invasive methods to screen and monitor disease severity and evaluate efficacy of treatments. Unfortunately, ocular surface diabetes research continues to lag behind systemic research as there is still a limited understanding of the course of the disease from obesity and prediabetes up through later stages of the disease when retinal damage is visible. With earlier detection and education of ocular pathological events, patients may be more motivated to take action to improve overall health and prevent loss of vision, which is considered by patients as more devastating than loss of a limb, memory, hearing or speech.98
Current anterior segment care is palliative and does nothing to stop or reverse the damage induced by diabetes. There are no guidelines for eye care for patients with obesity or prediabetes. While only severe diseases such as neurotrophic or bacterial keratitis have the potential to cause permanent visual loss, other changes to the cornea, conjunctiva, lids and tear function can lead to chronic discomfort, pain and fluctuations in vision which can have a significant impact on patients’ quality of life. More research is needed to understand if any current or novel treatments could halt or reverse the effects of metabolic disease on the eye.
Given the staggering numbers of undiagnosed patients with prediabetes and diabetes in the USA, better early screening test are needed. The ideal screening tests would be low cost, non-invasive and have high sensitivity and specificity. While the American Diabetes Association (ADA) recommends A1c testing for all patients over the age of 45 years and for overweight adults of any age, many of the most at-risk patients are not seeking preventative primary care and thus remain undiagnosed. Although we may be years away from eye tests that are incorporated into ADA recommendations for eye doctors to use routinely, recent ophthalmic research has begun to identify promising tests to elucidate multiple subclinical and clinical changes associated with diabetes in the anterior segment of the eye, including readily detectable changes in corneal thickness, stiffness and nerve density. Incorporating these tests into routine eye care could allow eye doctors to better understand the course of the disease process. Other changes such as corneal auto-fluorescence, conjunctival microvasculature and tear components are not currently feasible to conduct during routine eye care but could 1 day become biomarkers with the development of better clinical tools to accurately detect and monitor changes. This has been the case in other areas such as the InflammaDry (Quidel, San Diego, California, USA) for testing matrix metallopeptidase-9 levels in patients with dry eye. Continued research is needed to determine which clinical parameters and cut-off points could help practitioners improve the specificity and sensitivity of screening tools like the ADA risk questionnaire to identify patients at greatest risk. Therefore, this review is intended to provide clinicians and researchers with information about early anterior segment changes that may, someday, further help the detection of diabetes for patients in eye clinics. Most of the studies to date have included only patients with established diabetes already under treatment. Thus, it is not clear which of the anterior segment biomarkers might best be associated with early diabetes disease and could be further developed to improve screening and detection of patients with prediabetes or early undiagnosed diabetes. Continued research and analysis of anterior segment changes in patients with prediabetes and diabetes could ultimately help eye care providers identify and make more appropriate referrals long before the onset of diabetic retinopathy. Longitudinal studies of patients from the stage of obesity, or prediabetes, or the initial diagnosis of diabetes, would allow researchers to understand the mechanism underlying the impact of hyperglycemia and insulinemia on the ocular surface tissues.
In summary, given the epidemic rates of obesity, prediabetes and diabetes in the USA, there is a strong need for continued research to understand the anterior segment complication of metabolic disease and improve both diagnosis and treatment options for patients.
Acknowledgments
The authors would like to thank the students from Richdale’s and Harrison’s lab, University of Houston, College of Optometry shared the photos for this review paper.
References
Footnotes
Contributors All authors have contributions to the conception of the review, including drafting the work or revising it critically for important intellectual content. All authors have given final approval of the reversion published.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available.