Palliative radiotherapy
BMJ 2018; 360 doi: https://doi.org/10.1136/bmj.k821 (Published 23 March 2018) Cite this as: BMJ 2018;360:k821
- Katie Spencer, MRC clinical fellow in clinical oncology1,
- Rhona Parrish, salaried general practitioner and hospice doctor2,
- Rachael Barton, consultant clinical oncologist3,
- Ann Henry, associate professor in clinical oncology1
- 1Leeds Institute of Cancer and Pathology, University of Leeds, Leeds LS2 9NL, UK
- 2Garforth Medical Centre, Garforth, Leeds LS25 1HB, UK
- 3Queen’s Centre for Oncology and Haematology, Castle Hill Hospital, Cottingham HU16 5JQ, UK
- Correspondence to: K Spencer katie.spencer1{at}nhs.net
What you need to know
Palliative radiotherapy offers effective symptom control for focal disease due to cancer
Increased analgesia, anti-emetics, and in some cases corticosteroids can help to reduce discomfort and side effects
Acute side effects of radiotherapy usually resolve within 4-6 weeks of completing treatment
Symptoms of cancer may deteriorate before improvement
For patients in the final weeks of life, the side effects and disruption of palliative radiotherapy may outweigh the benefits, and holistic palliative care may be more appropriate
Palliative radiotherapy offers a quick, inexpensive, and effective way of reducing many of the focal symptoms of advanced, incurable cancer, whether these arise from the primary tumour or from metastatic deposits. It can improve quality of life while being associated with limited treatment burden in terms of both hospital attendances and side effects.1 The average UK general practice oversees care for around 20 patients with terminal cancer each year with higher numbers seen in secondary care,23 while a Canadian survey of general practitioners found that 85% had provided care for patients with advanced cancer within the previous month.4 This article aims to update non-specialists on the benefits, practicalities, and side effects of palliative radiotherapy to ensure that patients are considered and referred for these treatments when appropriate.
Sources and selection criteria
In developing this article, we used multiple sources. For each of the sites treated, we carried out a search of the Cochrane database to identify systematic reviews. Search terms used included “palliative AND radiotherapy AND bone metastases,” “spinal cord compression AND radiotherapy,” and “palliative radiotherapy AND lung cancer.” Where no Cochrane reviews were identified, we used Medline searches to identify other relevant systematic reviews and individual studies. We also searched our existing collections of relevant references and consulted appropriate experts where relevant studies could not be identified. In all cases we used the highest level of evidence available to inform this review, with more recent studies cited where possible. All searches were carried out between September 2017 and January 2018.
How is radiotherapy delivered?
Radiotherapy is delivered with linear accelerators (fig 1) in specialised cancer centres generally located in large urban areas (see box 1). High energy x rays are targeted to the disease site, causing DNA damage and cell death. Curative radiotherapy is routinely delivered over multiple, small daily doses (fractions) to reduce the risk of long term, permanent side effects in adjacent normal tissues.5 Palliative treatments require lower total doses, with the focus shifting to symptom control while minimising treatment burden. This change underpins the routine delivery of palliative radiotherapy using much shorter courses of larger fraction size (hypo-fractionation).

Linear accelerator used to deliver radiotherapy
{kind=link}
Practicalities of palliative radiotherapy
Anatomically targeted treatment during which the patient lies still on a relatively hard-topped treatment couch for about 15 minutes. The procedure itself is not associated with pain, but some may find the treatment position uncomfortable. Increased pain relief ahead of treatment can help. Occasionally this discomfort outweighs the benefits
Patients must be able to provide informed consent. In emergency situations (such as spinal cord compression) a decision may be made in the patient’s best interests if the patient lacks capacity and has no available representative
Patients must be able to follow verbal commands from radiographers outside the treatment room; a lack of capacity may make it difficult or even unsafe to deliver treatment. Sedation and anaesthesia are not routinely used for palliative radiotherapy
Palliative treatments are usually delivered as a single dose or a short course (usually over 1-3 weeks)
A close fitting mask maybe needed to ensure a consistent treatment position for treatments to the head, neck or upper chest (fig 2). This is generally well tolerated, even by more anxious patients
Re-treatment may be possible for recurrent symptoms, but side effects may be greater
Referrals and management of treatment related side effects can be discussed with the local radiotherapy department

For radiotherapy to the head, neck, or upper chest, a close fitting mask maybe needed to ensure a consistent treatment position
{kind=link}
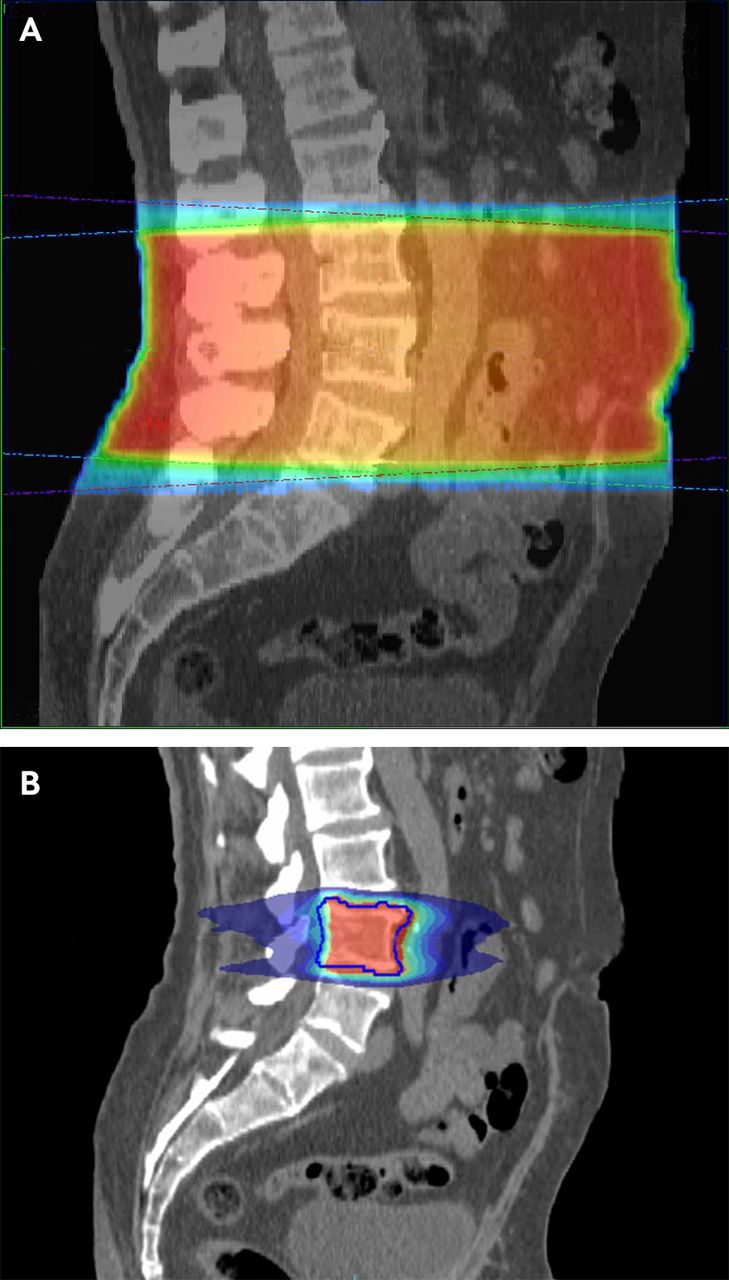
Increasingly, advanced techniques are used to offer more precise treatment delivery, allowing increased dose to the tumour while maintaining limited dose to surrounding tissues (stereotactic radiotherapy) (see fig 3).

Computed tomograms showing the difference in radiotherapy dose distribution between simple, conventional palliative radiotherapy (A), and targeted stereotactic radiotherapy (B). The latter treatment plan allows a dose of roughly three times greater biological effectiveness to the target with significantly lower dose to surrounding tissue
{kind=link}
What are the main barriers to referral for palliative radiotherapy?
Despite increasing numbers of radiotherapy treatment machines in the UK,6 national data highlight that radiotherapy use is lower than in Europe.78910 Internationally, multiple population based studies have shown that the chances of receiving palliative radiotherapy are dictated not only by clinical need but also by factors such as age, deprivation, and distance from treatment centre.1112 Questionnaire based studies suggest that a lack of understanding of the benefits of palliative radiotherapy among general practitioners and palliative care specialists may also be a barrier to referral.131415
What are the indications for using palliative radiotherapy?
A wide range of focal symptoms from advanced cancer can be treated with palliative radiotherapy as described below (and in table 1). Patients can undergo radiotherapy alongside palliative systemic anticancer treatments.
Benefits of palliative radiotherapy for varying indications (evidence referenced is the highest level identified)
Given that radiotherapy can only ever address focal disease, these treatments should supplement, not replace holistic palliative care. Assessment and support for all physical, psychological, and social needs, with strong communication between services, are necessary. Palliative radiotherapy rarely improves overall survival, which is reported to be a median of 5.2 months in one observational study.43 For patients with particularly limited prognosis, careful consideration of the appropriate level of intervention is essential; the potential benefits of treatment may be outweighed by expected side effects and treatment burden.
Pain due to bone metastases
Postmortem studies have detected bone metastases in up to 70% of patients with advanced cancer.44 Such metastases often cause localised pain and account for 35-40% of all palliative radiotherapy treatments.45 Pain may be constant or intermittent, can be neuropathic with a radiating dermatomal component and possible altered sensation, and often limits activities of daily living.46 Initial management combines analgesics and a holistic assessment of needs with interventions as required, such as home adaptations and walking aids.47 If, despite weak opioids, patients have persistent pain or side effects of medication, consider referral for radiotherapy.48 Metastases in long bones have a risk of pathological fracture. When this risk is assessed to be high, surgical stabilisation is often carried out before radiotherapy.495051
Palliative radiotherapy provides pain relief in a median of 2-3 weeks for 60% of patients (table 1).1617 Where pain recurs, retreatment can be considered after at least four weeks to allow response.52 Intravenous bisphosphonates offered equivalent pain relief to single fraction radiotherapy for metastatic prostate cancer in a single randomised controlled trial.19 This may be an alternative option for patients with prostate cancer naïve to bisphosphonates.
Symptoms due to locally advanced thoracic cancer
Lung cancer is the third commonest cancer in the UK and 28% of patients will present with locally advanced disease.5354 Thoracic symptoms include dyspnoea (50%), chest pain (28%), cough (40%), haemoptysis (10%), and dysphagia (7%).22 Some of these local symptoms can be successfully palliated in about two thirds of patients, although the success rate varies with symptoms. More information is provided in table 1.2021
Palliative radiotherapy to the mediastinum improved obstructive dysphagia from locally advanced oesophageal cancer in around two thirds of patients after a median of four weeks in a non-randomised phase I/II study.25 Given this delay in improvement and the risk of deterioration due to acute oesophagitis, patients with clinically significant dysphagia at baseline often undergo oesophageal stenting before radiotherapy.55 Radiotherapy improves durability of swallowing function after stenting.2627 However, for patients with very limited prognosis, stenting alone can provide rapid relief of dysphagia, and this group is unlikely to benefit from the addition of palliative radiotherapy.
Symptomatic radiation pneumonitis (occurring in <5%) can occur from six weeks to six months after treatment that includes the lungs.2021 Refer patients with cough and dyspnoea without another clear cause to the treating oncologist urgently for assessment and consideration of oral corticosteroids.
Pain and neurological compromise due to malignant spinal cord compression
Malignant spinal cord compression occurs when vertebral disease compresses the cord, either directly or as a result of vertebral collapse. More rarely, intraspinal or epidural metastases occur. Back pain is common, often occurring before neurological signs and symptoms, including sensory and motor disturbance and loss of sphincter control. Symptom progression varies, from neurological deterioration over hours to a gradual decline over weeks. Urgent magnetic resonance imaging (MRI) is required to confirm the diagnosis, and oral dexamethasone 16 mg once daily (with proton pump inhibitor) is routinely administered.5657 Subsequent assessments target expected prognosis in order to guide management decisions.5859
The median overall survival after a diagnosis of malignant spinal cord compression is 3-4 months.2960 When predicted prognosis is more than six months, neurosurgical decompression may be considered before radiotherapy on the basis of a single randomised study showing improved neurological outcomes.32 Unfortunately, most patients have a prognosis of less than six months. For these patients, urgent palliative radiotherapy (within 24 hours of MRI confirmation) aims to reduce pain and retain or improve neurological function.56 The best neurological outcomes are seen in those retaining some movement before treatment or with gradual onset of neurological symptoms.61 For patients with established paraplegia, less than 10% regain mobility; in the absence of pain, and if the prognosis is very limited, holistic palliative care and appropriate social or nursing support may be more appropriate.62
Acute side effects reflect the vertebral level treated, while late radiation induced spinal cord myelopathy is rarely seen with palliative doses (<1%).63
Symptoms due to brain metastases
Brain metastases occur in 20-40% of individuals with systemic cancer.34 Presentation can be with seizures, focal neurology, or symptoms of raised intracranial pressure (nausea, vomiting, and headaches). Prognostic indices help to tailor treatment to the individual patient.6465 For those with limited brain metastases and a life expectancy of more than six months, neurosurgery or stereotactic radiotherapy can be considered under discussion with the treating team, local neurosurgical or neuro-oncology teams, and patient.3666
For those with more extensive cerebral disease who retain a good performance status, whole brain radiotherapy can be offered, although no high quality randomised data exists to support this over corticosteroids alone.67 Indeed, a recent trial demonstrated no survival or quality of life benefit from whole brain radiotherapy over steroids alone in patients with brain metastases from non-small cell lung cancer.33 This has resulted in a reduction in the use of whole brain radiotherapy in this situation, but extrapolation to other cancer diagnoses is unlikely to be justified.
Symptoms due to advanced head and neck cancer
Patients with locally advanced head and neck cancer often present with a range of difficult to control symptoms including pain, dysphagia or odynophagia, airway compromise, bleeding, and cosmetically distressing tumour bulk.68 These often frail patients have complex needs and require multidisciplinary support including specialist nursing and medical care, support from allied health professionals, palliative care, and community support with strong communication between services.
Prospective studies report improvement in pain control and quality of life in about 50-60% of patients after palliative radiotherapy, with improved ability to eat solids in 33%.3738 Of note, in one UK series, 18% of patients required hospital admission during or immediately after treatment for nutrition, dehydration, and pain control.68
Symptoms due to advanced pelvic cancers
Locally advanced pelvic cancers can result in bleeding, discharge, bowel obstruction, urinary disturbance, and pelvic pain. Radiotherapy palliated bleeding in up to 90% of patients with advanced bladder, rectal, or gynaecological cancer and improved other symptoms for half to two thirds of patients.39404269 Acute side effects frequently occur, alongside temporary deterioration of existing symptoms. If abdominal discomfort or diarrhoea are severe or fail to resolve with simple measures, seek advice from the treating oncology team.
Bleeding, pain, and malodour due to skin cancers
Symptoms of bleeding, pain, and malodour due to advanced primary skin cancers responded to palliative radiotherapy in 61% of cases in a small observational study.70 Cutaneous disease—most commonly arising from breast cancer (metastases or primary), melanoma, and lung cancer71—can be treated similarly, although the evidence is extremely limited and there are no randomised comparisons with alternative approaches (such as surgical resection, electro-chemotherapy, photodynamic therapy, topical treatments).7273
What are the most common side effects of palliative radiotherapy?
The side effects of radiotherapy are dictated by which tissues receive a substantial dose. For example, conventional radiotherapy to lumbar spine vertebral metastases will usually involve irradiation of the bowels, resulting in side effects related to both the bone metastasis and bowels (see fig 3). Additionally, treatment is associated with fatigue in at least two thirds of patients, and this can affect quality of life, limiting participation in preferred activities.7475
Acute side effects of palliative radiotherapy usually resolve within 4-6 weeks of completing treatment. In routine practice, palliative prescribing of analgesia (including strong opiates) and antiemetics underpins the management of side effects. Randomised evidence is limited, and the recommendations for management of side effects (see table 2) are predominantly based on systematic reviews and guidelines.
Management of the acute side effects of palliative radiotherapy by organ or tissue
Long term side effects are uncommon in palliative radiotherapy, and management of these is led by the treating team with multidisciplinary involvement when required.106
What new treatments can we expect?
The radiotherapy dose delivered to a tumour is usually limited by likely side effects in surrounding tissues. Advanced techniques that offer treatments more closely matched to the tumour shape, delivered with computed tomography on the treatment couch immediately before radiotherapy, can more accurately target much higher radiotherapy doses to small focal disease sites. These more targeted stereotactic treatments are variously referred to as stereotactic body radiotherapy, stereotactic ablative body radiotherapy, and stereotactic radio-surgery. Figure 3 provides an example of the difference in radiotherapy dose distribution between the simple conventional palliative approach and these more complex treatments.
There is now the potential for these higher dose stereotactic treatments to be used to improve survival and quality of life in patients with metastatic disease. This is being investigated for “oligo-metastatic disease” (in which a patient has only a limited number of metastatic deposits, and the disease has not become widespread).115 For such patients, high dose stereotactic treatments can be used to ablate all macroscopic sites of disease, potentially resulting in superior overall survival. However, even the existence of the oligo-metastatic state remains controversial.110 A further possible role for these treatments is in more advanced disease, where a higher radiotherapy dose to a symptomatic metastasis might provide better and more durable symptom control while continuing to deliver treatment in a minimum number of fractions with limited toxicity to surrounding tissues.108109111 There are no randomised data to support either of these approaches currently. Their expected value remains controversial, and trials are now under way for a range of indications.107108109112113116
An additional area of palliative radiotherapy in which significant advances are now being made is in the use of radionuclides. These treatments deliver radioactive isotopes to tumour tissue, either through anatomically targeted delivery (such as via the hepatic artery in metastatic colorectal cancer) or through the use of radiolabelled molecules or monoclonal antibodies which are preferentially taken up by the tumour or its microenvironment.117 Historically, their use has been limited to some relatively rare tumours, but novel agents are increasingly demonstrating benefits in a range of more common conditions such as metastatic prostate cancer.114 With trials ongoing internationally, these treatments are likely to be used more extensively over the next few years.
A patient’s perspective
My late husband received palliative radiotherapy multiple times during his treatment for multiple myeloma. Early in the course of his disease, radiotherapy for back pain and spinal cord compression ensured that he was able to continue the gardening he had always enjoyed. Receiving treatment was never uncomfortable for him, but, as his general condition deteriorated towards the end of his life, he spent more time in hospital and the benefits of radiotherapy became less clear. He had a mask made for one of his treatments which covered his head and neck: he didn’t find this particularly uncomfortable and he was excited to show it to everyone. He even let his grandchildren play with it once treatment was completed.
Education into practice
Think about the last time you saw a patient with advanced cancer. How much did you consider localised disease as a possible cause of their symptoms?
Would you feel confident referring them to discuss palliative radiotherapy to help treat their symptoms?
What else might you do differently as a result of reading this article?
How patients were involved in the creation of this article
A patient representative (a relative of a previously treated patient) had the opportunity to review and comment on the draft manuscript. She did not feel any changes to the manuscript were needed but did share her experiences of her husband’s radiotherapy treatment.
Footnotes
Contributors: KS and AH conceived of the manuscript. KS wrote the initial draft manuscript and is guarantor. All authors contributed to manuscript revisions; defining the structure and content of the final draft. A patient representative and her family reviewed the draft manuscript and provided a carer’s perspective of the radiotherapy process. RP provided a generalist perspective. All authors approved the final draft.
Funding: While undertaking this work KS was funded by the Medical Research Council on a Clinical Research Training Fellowship (MR/N021339/1).
Competing interests: We have read and understood BMJ policy on declaration of interests and have no relevant interests to declare.
Provenance and peer review: Commissioned, based on an idea from the author; externally peer reviewed.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: http://creativecommons.org/licenses/by/4.0/.