Effect of high throughput RHD typing of fetal DNA in maternal plasma on use of anti-RhD immunoglobulin in RhD negative pregnant women: prospective feasibility study
BMJ 2008; 336 doi: https://doi.org/10.1136/bmj.39518.463206.25 (Published 10 April 2008) Cite this as: BMJ 2008;336:816
- Kirstin Finning, clinical scientist1,
- Pete Martin, clinical scientist1,
- Joanna Summers, biomedical scientist1,
- Edwin Massey, consultant haematologist1,
- Geoff Poole, head of red cell immunohaematology2,
- Geoff Daniels, head of molecular diagnostics1
- 1International Blood Group Reference Laboratory, NHS Blood and Transplant, Bristol BS10 5ND
- 2NHS Blood and Transplant, Bristol
- Correspondence to: G Daniels geoff.daniels{at}nbs.nhs.uk
- Accepted 25 February 2008
Abstract
Objectives To assess the feasibility of applying a high throughput method, with an automated robotic technique, for predicting fetal RhD phenotype from fetal DNA in the plasma of RhD negative pregnant women to avoid unnecessary treatment with anti-RhD immunoglobulin.
Design Prospective comparison of fetal RHD genotype determined from fetal DNA in maternal plasma with the serologically determined fetal RhD phenotype from cord blood.
Setting Antenatal clinics and antenatal testing laboratories in the Midlands and north of England and an international blood group reference laboratory.
Participants Pregnant women of known gestation identified as RhD negative by an antenatal testing laboratory. Samples from 1997 women were taken at or before the 28 week antenatal visit.
Main outcome measures Detection rate of fetal RhD from maternal plasma, error rate, false positive rate, and the odds of being affected given a positive result.
Results Serologically determined RhD phenotypes were obtained from 1869 cord blood samples. In 95.7% (n=1788) the correct fetal RhD phenotype was predicted by the genotyping tests. In 3.4% (n=64) results were either unobtainable or inconclusive. A false positive result was obtained in 0.8% (14 samples), probably because of unexpressed or weakly expressed fetal RHD genes. In only three samples (0.2%) were false negative results obtained. If these results had been applied as a guide to treatment, only 2% of the women would have received anti-RhD unnecessarily, compared with 38% without the genotyping.
Conclusions High throughput RHD genotyping of fetuses in all RhD negative women is feasible and would substantially reduce unnecessary administration of anti-RhD immunoglobulin to RhD negative pregnant women with an RhD negative fetus.
Introduction
Alloimmunisation against the RhD (RH1) red cell surface antigen is the commonest cause of haemolytic disease of the fetus and newborn, which, before the introduction of anti-D prophylaxis after delivery in the 1960s accounted for the death of one baby in 2200.1 2 Over the next 40 years the effect of the anti-RhD prophylaxis programme and improved neonatal care reduced the incidence to one death in 21 000.3
In 2002 the National Institute for Health and Clinical Excellence (NICE) in the United Kingdom undertook an assessment of the cost effectiveness of routine antenatal anti-RhD prophylaxis with anti-RhD immunoglobulin.3 Previously anti-RhD immunoglobulin had been administered antenatally only when events occurred that would be associated with a feto-maternal haemorrhage. NICE recommended that all RhD negative pregnant women should be offered anti-RhD immunoglobulin at 28 and 34 weeks’ gestation.3 In a predominantly white population, however, about 38% of these women would be carrying an RhD negative fetus4 and would receive the treatment unnecessarily. Consequently, NICE also “endorsed studies into the feasibility of mass testing antenatally for fetal blood group by analysis of fetal DNA in maternal plasma.”3 The benefits of this testing would be twofold. Firstly, there would be a substantial reduction in the use of anti-RhD immunoglobulin, an expensive blood product in short supply. Secondly, women with an RhD negative fetus would be spared unnecessary exposure to this pooled human blood product with its associated discomfort and perceived risk from viral or prion contamination. This risk is exemplified by the infection of hundreds of women with hepatitis C virus transmitted by anti-RhD immunoglobulin in Ireland in 1977-8.5
Anti-RhD immunoglobulin is produced by the pooling and fractionation of plasma from large numbers of donors who themselves are RhD negative and have been exposed to RhD positive red cells to stimulate the production of RhD antibodies. Although the future of anti-RhD immunoglobulin might involve monoclonal or recombinant products, thus eliminating the risks associated with human blood products, there is still no indication that these are to be introduced in the foreseeable future and costs would probably increase if recombinant products were used.6
The antigens of the Rh blood group system are located on two proteins encoded by two homologous genes, RHD and RHCE.4 The most immunogenic of the Rh antigens, RhD, is encoded by RHD. About 15% of white people are RhD negative and are usually homozygous for a deletion of RHD, whereas RhD positive people have either one or two copies of RHD.7 Tests for predicting RhD phenotype from DNA involve the amplification of one or more regions of RHD to determine whether the gene is present. Numerous variants of RHD exist: in some, all or part of RHD is present but no RhD antigen is expressed; in others, part of RHD is absent but a variant form of RhD antigen is present.4 8 RHD variants are relatively rare in white people, but an inactive RHD gene, called RHDΨ, is present in 66% of RhD negative black Africans.9 RHDΨ contains a 37 base pair duplication plus a nonsense mutation and must be taken into account in any method for RHD genotyping.
Since 1995 the International Blood Group Reference Laboratory of the English National Blood Service has been providing a fetal RHD genotyping service for RhD alloimmunised women whose fetuses might be at risk of haemolytic disease of the fetus and newborn.10 11 In 1997 Lo et al showed that about 3-6% of cell-free DNA in the plasma of pregnant women is of fetal origin and can be used for predicting RhD fetal phenotype in RhD negative women.12 13 In 2001 the laboratory introduced fetal RHD genotyping from fetal DNA in maternal plasma to their molecular diagnostics service. Maternal plasma has now almost replaced fetal cells, obtained by amniocentesis or chorionic villus sampling, as the source of fetal DNA, hence eliminating the need for invasive sampling procedures.11 The method currently used routinely for fetal RHD genotyping is labour intensive and expensive and therefore not suitable for the mass screening of all RhD negative women. Recent developments in technology and the introduction of automated robotic techniques have brought down costs and increased the potential for higher throughput.
We validated a high throughput RHD fetal genotyping technique by comparing the results obtained with the RhD serological phenotype obtained from cord blood taken at delivery.
Methods
Blood samples
Anticoagulated blood samples were chosen for fetal genotyping from any RhD negative pregnant women attending antenatal clinics that use the Birmingham and Sheffield centres of the National Blood Service for routine ABO and RhD blood grouping and antibody screening. This did not involve taking additional blood samples to those collected for routine testing. The blood samples were collected at the women’s 28 week visit to the antenatal clinic. Ethnicity was 55% white, 8% Asian, 1.5% black, 0.5% Caribbean black, 1% mixed, 1% other, and 33% unknown or not given. We selected at least 1500 individuals on the basis of 80% power to detect an error rate of 2%.
Robotic isolation of DNA from maternal plasma
Bar coded blood tubes containing 4-6 ml of anticoagulated blood were centrifuged for 10 minutes and the tubes were then transferred directly to the sample rack of the MDx BioRobot (Qiagen, Hilden, Germany) without disturbing the buffy coat. DNA was robotically extracted from 0.56 ml of maternal plasma and eluted into nuclease-free water in a 96 well plate. This procedure took about three hours, with a capacity of 88 blood samples per run. The extracted DNA was used for real time quantitative polymerase chain reaction immediately or stored at −30°C until testing was performed.
Real time quantitative polymerase chain reaction to detect the presence of RHD
The MDx BioRobot was used as a liquid handling robot to dispense a mix of Universal PCR MasterMix (Applied Biosystems, Foster City, CA, USA) and primers and probes for exons 5 and 7 of the RHD gene (as a multiplex) or the CCR5 gene (see table A on bmj.com) into a 384 well polymerase chain reaction plate. DNA (5 μl) from each maternal sample was dispensed into three wells containing reaction mix for the RHD gene and into a single well containing reaction mix for CCR5. Control wells for the RHD assay containing RhD positive DNA, RhD negative DNA, RHDΨ positive DNA, and no DNA were also dispensed. Real time quantitative polymerase chain reactions were performed on the ABI Prism 7900HT (Applied Biosystems) to detect the presence of fetal RHD gene sequences and to quantify total (maternal and fetal) DNA in the plasma. These tests were interpreted without knowledge of the RhD phenotype, which was subsequently determined on red cells from the cord blood sample. The procedure took about three hours with a capacity of DNA from 88 blood samples per run.
Interpretation of real time polymerase chain reaction results
The RHD exon 7 assay amplified both RHD and RHDΨ, whereas the exon 5 assay amplified RHD only. A cycle threshold value of less than 42 was interpreted as a positive signal. An algorithm was created to predict fetal RhD phenotype and to recommend whether anti-RhD should be offered or withheld, depending on the number of positive signals obtained for both RHD exons 5 and 7. Confirmation of successful DNA extraction and an estimation of the amount of total DNA in the sample were provided by the single amplification of CCR5 (not fetal specific).
Statistical analysis
We used GraphPad Prism 5 software package (GraphPad Software, San Diego, CA) to analyse the results. We used Fisher’s exact test (two tailed) to determine the sensitivity and specificity of the test and the Mann-Whitney rank sum test to compare the effect of total DNA concentration on the accuracy of the prediction of fetal RhD status and whether to recommend giving anti-RhD immunoglobulin. We regarded a two tailed probability value (P value) of <0.05 as significant.
Serological RhD testing on cord bloods
The accredited testing laboratories in the National Blood Service and in hospital trusts performed RhD typing on cord blood samples using routine serological methods. At that time they did not know the genotype as determined from the fetal DNA.
Results
Paired analyses
RHD genotyping was performed on DNA from 1997 pregnant women, with a mean gestational age of 27.9 weeks (median 28 weeks, range 8-38 weeks). Most (92%) samples were tested at 26-32 weeks’ gestation. Cord blood RhD phenotypes were available from 1869 deliveries; 128 fetal phenotypes were not available for paired analysis because 124 cord samples were untraceable and there were four fetal deaths. When twins were delivered (n=13), the expected genotype from maternal plasma was RHD positive if at least one of the babies was RhD positive.
Prediction of fetal RhD phenotype from DNA
In 95.7% of cases the fetal RhD status predicted from the genotype was the same as the serologically determined phenotype from cord blood: 1118 (59.8%) were RhD positive and 670 (35.9%) were RhD negative (table)⇓. There were 14 false positive results (0.8%), in which an RHD gene was detected but the phenotype determined serologically from cord blood was RhD negative. Cord blood samples were not available for DNA extraction so we were unable to test for the presence of variants of RHD associated with non-expression or weak expression of the RhD antigen, the most likely and expected causes of these apparently incorrect results. Only three samples (0.16%) gave “false negative” results. Eight samples (0.4%) gave “variant RHD” results, which were exon 7 positive but exon 5 negative. This pattern would be expected if the fetus had inherited RHDΨ or, less commonly, the variant RHDVI gene. Four of these eight fetuses were subsequently shown to be serologically RhD negative and might have had these variant genes, and the remaining four were RhD positive.
Results of testing 1869 DNA samples from plasma of RhD negative pregnant women for fetal RHD and comparison with serologically determined phenotype of her baby’s cord sample*
Inconclusive fetal genotyping results were obtained from 56 samples (3%), of which 31 were from fetuses that were RhD positive and 25 were from fetuses that were RhD negative. One inconclusive result arose from a failure to extract DNA from the plasma. Thirty samples gave insufficient positive and negative replicates and so we categorised them as inconclusive. Twenty five of the inconclusive results (1.3%) arose from the presence of a suspected maternal RHD gene and in these cases the fetal phenotype was not predicted. Further tests on DNA derived from the women’s buffy coats revealed that three women were normal RhD negative, indicating an excessively large amount of fetal DNA in their plasma. Ten women had RHDΨ, one had RHDVI, and one had a single point mutation in RHD (722C>T, Thr241Ile), apparently preventing full expression of the RhD protein. The remaining 10 women all had at least an RHD exon 7, but further analysis of their RH genes was not performed.
Accuracy of test to determine requirement for anti-RhD administration
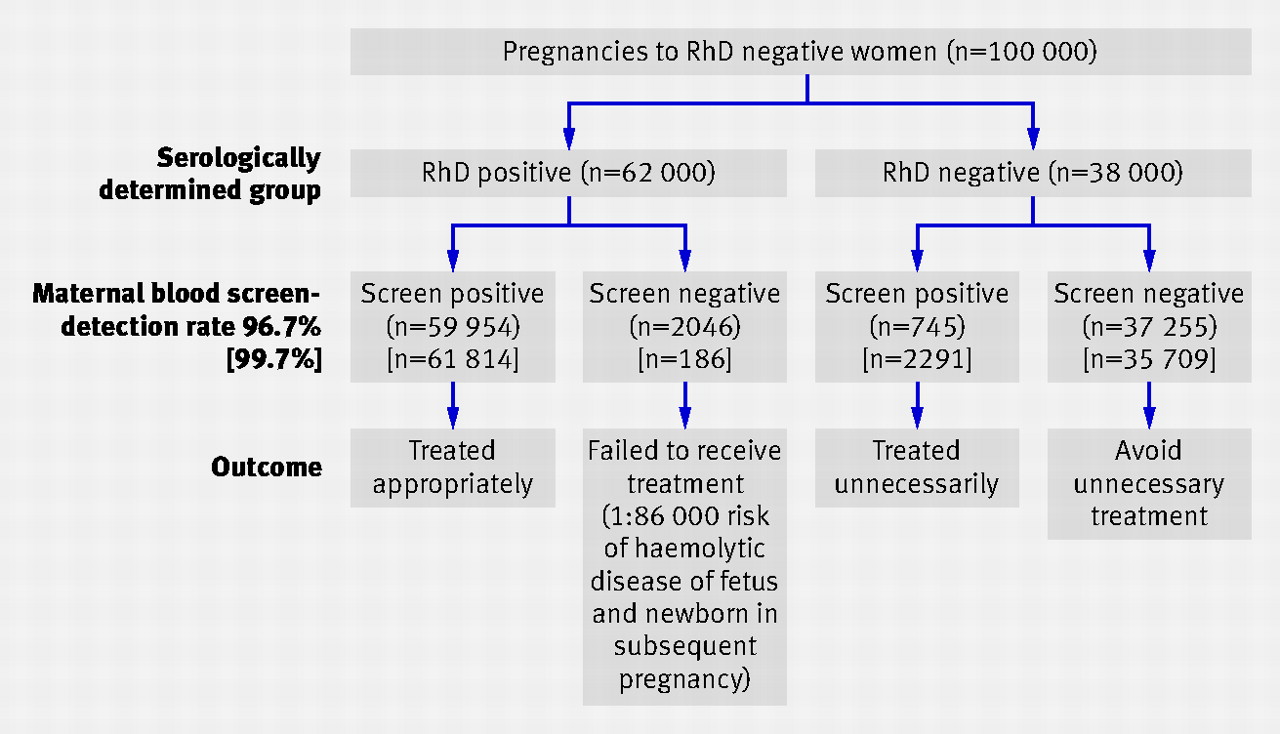
We compared two alternative models for determining the accuracy of the maternal plasma test. The fetus was categorised as “screen positive” if either the predicted phenotype from DNA was RhD positive, or the predicted phenotype from DNA was RhD positive, RHD variant, or inconclusive. With the first model, the detection rate was 96.7%, the false positive rate was 1.96%, and the odds of being RhD positive given a positive result were 80:1. By the second method, the detection rate was 99.7%, the false positive rate was 6.0%, and the odds of being RhD positive given a positive result were 27:1. The second, more cautious, definition of “screen positive” is therefore more beneficial because more RhD positive fetuses are detected for an acceptable increase in the false positive rate (figure)⇓. If this model was applied to all RhD negative pregnant women in England and Wales, it would prevent a considerable number of women with RhD positive fetuses being omitted from treatment (figure).⇓ If it had been used to decide which women in this trial should receive prophylaxis, 64% would have received anti-RhD (of whom 96.4% had RhD positive babies). Of the women in the trial, 62% gave birth to RhD positive babies and therefore only 2% of women would have received anti-RhD unnecessarily, compared with 38% without genotyping.

Hypothetical flow diagrams of fetal RHD screening from maternal blood, with positive screen result classes as predicted phenotype from DNA of RhD positive only or with predicted phenotype from DNA of RhD positive, RHD variant, and inconclusive results
{kind=link}
Discrepant results
We analysed the effect of DNA concentration in maternal plasma on the ability to determine fetal RHD genotype. We compared the amount of DNA in the three maternal plasma samples that gave false negative results and in the 31 inconclusive samples (where maternal RHD was not present) with the amount of DNA in maternal plasma samples when the fetus was correctly predicted to be RhD positive. The mean total DNA concentration was found to be significantly higher in the false negative and inconclusive samples (P<0.001), which might explain the failure to amplify fetal DNA in these cases. Many samples that gave false negative or inconclusive results were more than 14 days old and had excessively high levels of maternal DNA, probably as a result of the breakdown of maternal leucocytes. Under usual clinical laboratory criteria these samples would not have been accepted for testing and repeat samples would have been requested.
Discussion
We have developed a high throughput technology for determining fetal RHD genotype from cell free fetal DNA in the plasma of RhD negative pregnant women. We tested almost 2000 samples from RhD negative women and compared the results with RhD phenotypes obtained by serological testing of red cells from the corresponding cord blood samples. There was concurrence between genotype and phenotype in 95.7% of the tests. In 0.8% of the tests the genotype falsely predicted an RhD positive phenotype and in 0.16% of the tests the genotype falsely predicted an RhD negative phenotype. In the remaining 3.4% of the tests the genotyping results were inconclusive.
Benefits of fetal RhD testing
In accordance with current NICE guidelines,3 all RhD negative women in the UK should be offered routine antenatal anti-RhD prophylaxis of at least 500 IU of anti-RhD immunoglobulin at 28 and 34 weeks’ gestation or a single dose of 1500 IU at 28 weeks’ gestation. About 38% of white RhD negative women carry an RhD negative fetus and receive anti-RhD immunoglobulin unnecessarily.4 Lack of a safe and reliable technique for routine fetal RHD genotyping with sufficiently high throughput has meant that to protect all RhD negative women, those with an RhD negative fetus also receive prophylaxis.
Our results show that fetuses of RhD negative women could be RHD genotyped with an acceptable level of accuracy. Application of the testing protocol before 28 weeks’ gestation, while still leading to anti-RhD administration in 2% of mothers with RhD negative fetuses, would avoid unnecessary treatment in about 36% of RhD negative women and avert the associated discomfort, inconvenience, and risk of exposure to pooled donor blood products that such injections entail. In theory, RhD negative women would be saved an additional visit to the midwife for a second dose at 34 weeks’ gestation, though routine care might require such a visit. Potential sensitising events, such as abdominal trauma or vaginal bleeding, occurring after 28 weeks’ gestation would not require additional treatment with anti-RhD immunoglobulin in the 36% of cases shown to have an RhD negative fetus. In addition, should these tests prove completely reliable, the routine RhD serological testing of cord blood samples from neonates of RhD negative mothers could be eliminated.
Relevance of false positive results
The incidence of an RHD positive genotype associated with an RhD negative phenotype (0.8%) is consistent with the prevalence of RHD genetic variants associated with lack of phenotypic expression of an RhD antigen found in other studies.14 15 Such “false positives” would, however, be of limited importance. Only a few mothers would continue to receive anti-RhD immunoglobulin unnecessarily with RHD genotyping compared with the large numbers currently treated in the absence of fetal genotyping. In fact, the red cells of some of these fetuses probably express small quantities of RhD antigen, not detected by routine serological testing, and so administration of anti-RhD could be considered appropriate.
Relevance of false negative results
A false negative result could be more important because withholding treatment from women carrying an RhD positive fetus would be associated with potential alloimmunisation and morbidity or mortality from haemolytic disease of the fetus and newborn in subsequent pregnancies. The risk of alloimmunisation occurring when anti-RhD prophylaxis is given only after delivery is about 1% compared with 0.3% if antenatal prophylaxis is also given.3 The overall risk of antenatal alloimmunisation depends on the likelihood of a subsequent pregnancy (62%) and that the baby will be RhD positive (71.5%, assuming no change of partner). Based on the observed detection rate in this trial of 99.7%, the risk of future pregnancies being affected by haemolytic disease of the fetus and newborn that would have been prevented by giving all RhD negative women anti-D at 28 and 34 weeks’ gestation is 1:86 000 RhD negative women. About 5% of sensitisations result in fetal or neonatal death and another 5% of infants might experience mild to severe developmental problems, therefore a false negative result would lead to about one additional case of fetal or neonatal loss or of developmental problems occurring per 860 000 RhD negative pregnant women. This modest apparent increase in risk might, however, be offset by an increased uptake of prophylaxis among mothers who have been correctly identified as carrying an RhD positive fetus.
In our study only three samples gave an apparently false RhD negative result. Some of the samples tested in this trial, including these three, were delayed in transport, which could reduce accuracy of the results. Strict implementation of a policy of testing only samples that were less than seven days old would increase the logistical problems of transportation over large geographic areas but would reduce the risk of false negative results.
Variant RHD genes
Categorisation of a fetus predicted to carry a variant RHD gene as “screen positive” might be an overcautious approach as these are probably fetuses with either an inactive RHDΨ gene or with an RHDVI gene, which produces a weak variant D antigen, and neither is likely to cause alloimmunisation of the mother. If this method were introduced for routine testing, further validation of the test might result in such variants being treated as RhD negative and antenatal immunoglobulin therapy being withheld.
When the mother is predicted to carry an RHD gene, a cautious approach should be applied. In this study, 72% of women suspected of having RHD genes gave birth to RhD positive babies and treating such inconclusive cases as “screen positive” would seem to be the most appropriate approach.
Application of the technology
No diagnostic test has 100% sensitivity and specificity, including the serological testing that was used as the reference for determining the accuracy of the molecular tests in this study. The earlier in pregnancy that fetal DNA is tested the greater the risk that it will not be detected because cell-free fetal DNA concentrations rise as pregnancy progresses.16 Most of our tests were performed on blood taken at the 28 week visit, during which the first dose of anti-RhD immunoglobulin is usually given. For the fetal RhD testing to be completed and the results fed back to the antenatal clinics before this visit, blood samples would need to be taken at 26 weeks’ gestation. It is unlikely that this would make a significant difference to the accuracy of the testing. In the trial, 183 samples were from women at 26 weeks’ gestation or earlier and tests on these resulted in no false negative results. Alternatively, if the policy on routine antenatal prophylaxis were modestly changed to a single dose of anti-RhD immunoglobulin given at 30 weeks’ gestation, then testing at 28 weeks would be suitable. Commencement of treatment at 30 rather than 28 weeks has previously been considered as an option in the UK,17 18 and since 1998 the practice in Holland has been to give 1000 IU of anti-RhD at 30 weeks’ gestation.19
Other trials
A similar fully automated trial has been performed in Amsterdam, in which 2359 samples taken at 30 weeks’ gestation were tested for RHD exon 7 after robotic isolation of DNA from maternal plasma and real time quantitative polymerase chain reaction technology.20 In 1257 of the cases in which molecular results could be compared with serological results, researchers obtained three false negative results and five false positive results, giving a diagnostic accuracy of 99.4%.
Future studies
Clearly there could be benefits from taking maternal blood samples for fetal RHD genotyping at earlier stages of the pregnancy than 28 weeks’ gestation to coincide with existing planned antenatal visits. Consequently, we are about to start feasibility trials on testing maternal blood samples obtained during the first visit to the antenatal clinic, normally at 8-16 weeks’ gestation, and at the visit for the anomaly scan at 20 weeks.
Conclusions
High throughput RHD genotyping performed on free fetal DNA in maternal plasma at about 28 weeks’ gestation reliably predicts fetal RhD phenotype with an acceptably low rate of false negative results. The introduction of fetal genotyping followed by the withholding of antenatal anti-RhD prophylaxis from mothers with an RhD negative fetus would result in about 36%of women being saved from unnecessary exposure to human blood products, inconvenience, and discomfort.
What is already known on this topic
Fetal RhD phenotype can be predicted from fetal DNA in the plasma of RhD negative pregnant women
About 38% of RhD negative pregnant women have an RhD negative fetus and might receive unnecessary antenatal anti-RhD immunoglobulin
What this study adds
An automated high throughput method developed for determining fetal RhD phenotype from fetal DNA in the plasma of RhD negative pregnant women is accurate
Screening of fetal RHD in all RhD negative pregnant women is feasible
Footnotes
We thank the many pregnant women who took part in this study. We are also grateful to Ian Skidmore, Craig Wilkes, Richard Mason, and other managers and staff in the red cell immunohaematology laboratories of the National Blood Service, the staff of the hospital trusts in the Birmingham, Sheffield, and Oxford regions, and Helen Williams, Maggie Pailing, and Sue Cotton of the National Blood Service Hospital liaison team for their advice. Michael Spratt, research statistician of the University of Bristol, provided valuable statistical input into the design of the study, and Ian Franklin, Ann Gooch, and Frank Boulton assisted with the manuscript.
Contributors: All authors participated in the study design, study implementation, and interpretation of the results. GD is guarantor.
Funding: KF, PM, JS, and GD were supported by the UK Department of Health. Some funding for consumables was provided by the European Union through the Special Non-Invasive Advances in Fetal and Neonatal Evaluation (SAFE) Network of Excellence.
Competing interests: None declared.
Ethical approval: Central office for research ethics committees in the UK.
Provenance and peer review: Not commissioned; externally peer reviewed.