Article Text

Statistics from Altmetric.com
Description
A 66-year-old Afro-Caribbean woman presented with a 1-day history of sharp left flank pain. This was associated with nausea and diarrhoea, without fever or urinary symptoms. Her medical history includes type 2 diabetes mellitus on insulin therapy but with suboptimal control (haemoglobin A1c 80 mmol/mol or 0.23 g/dL glucose levels) and related complications including chronic kidney disease, retinopathy, peripheral neuropathy, hypertension, sickle cell trait, obesity and osteoarthritis. Blood investigations demonstrated leucocytosis (white cell count 12.7×109/L) and deranged renal function (creatinine 150 µmol/L; baseline 110 µmol/L). Urine dipstick test was positive for nitrites, ketones and glucose and urine culture isolated mixed growth of bacteria with Candida.
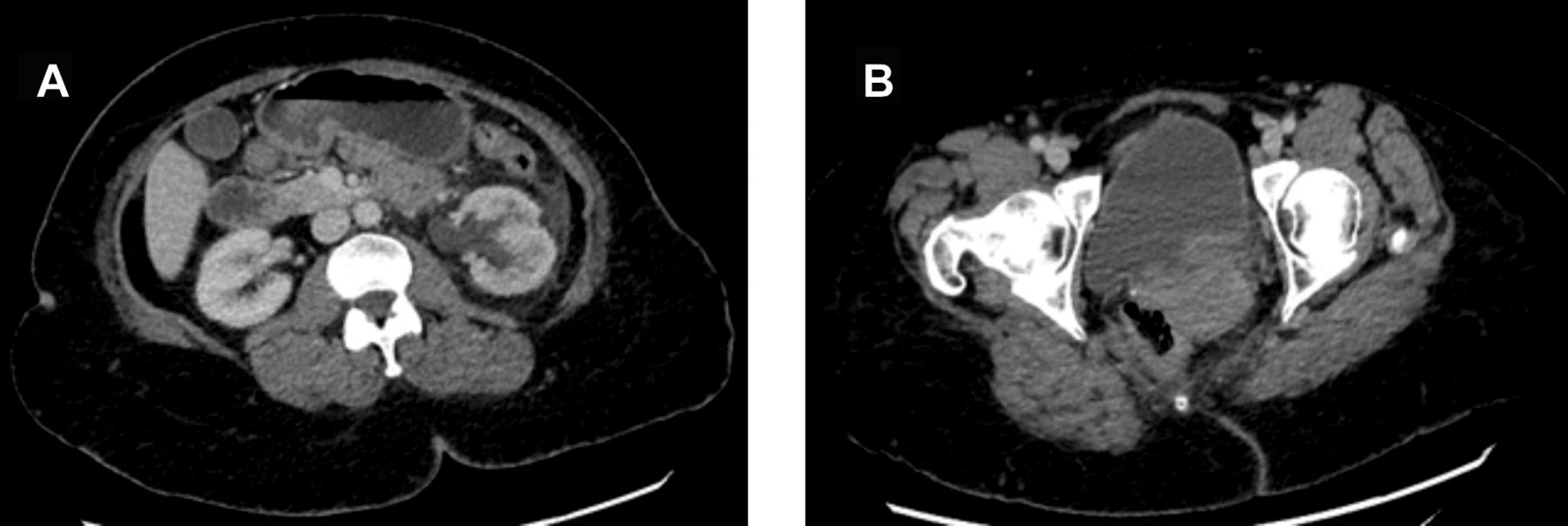
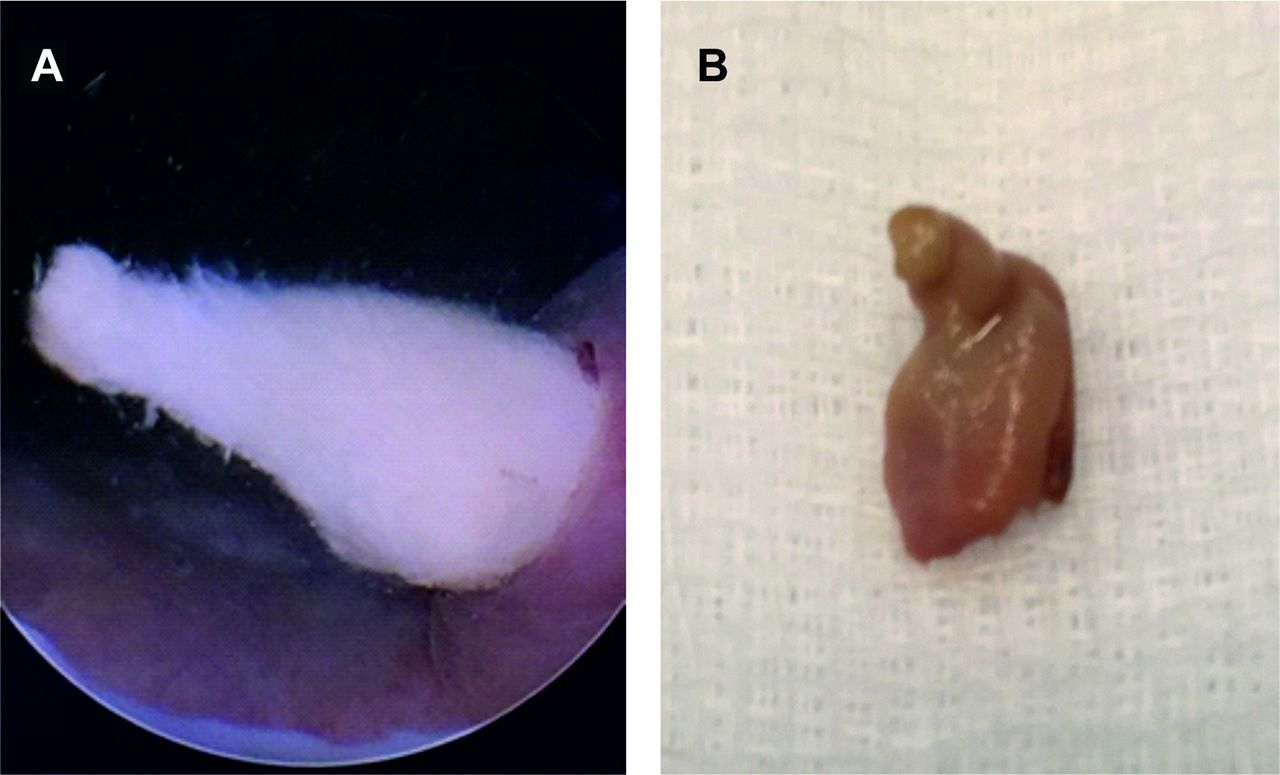
A CT abdomen/pelvis, initially planned on the working diagnosis of acute diverticulitis, revealed a mild left-sided hydroureteronephrosis associated with perinephric inflammatory stranding. Left posterolateral bladder wall thickening and left distal ureteric enhancement were also highlighted (figures 1 and 2). The patient was commenced on intravenous co-amoxiclav for the treatment of urosepsis. Though she remained afebrile, on the following day her blood investigations significantly worsened (white cell count 19.7×109/L, C reactive protein 429 mg/L and creatinine 429 µmol/L) and emergency diagnostic cystoscopy and insertion of a left ureteric stent was planned. The bladder appeared normal but a lump of necrotic soft-tissue could be seen protruding from the left ureteric orifice (figure 3), in keeping with a sloughed renal papilla wedged at the vesicoureteric junction. This was removed intact with biopsy forceps and a 6 French/22 cm ureteric stent was inserted (figure 4). Postoperatively, the patient’s symptoms rapidly improved and her blood tests including renal function returned to baseline. She was discharged on oral antibiotic therapy and had successful stent removal 2 weeks later. Histological analysis confirmed an infarcted renal papilla with focal necroinflammatory bacterial colonisation of the residual medullary collecting ducts (figure 5). In the following months, the patient remained well with stable renal function and a renogram demonstrated adequate renal drainage with no obstruction. She was referred to the Endocrine Team for optimisation of her diabetic control.

Transverse views of CT abdomen/pelvis scan (with intravenous contrast). The CT revealed mild left-sided hydroureteronephrosis with extensive perinephric stranding with no other cause for these findings (A). There is also possible posterior bladder wall thickening near the ureteric orifice and left distal ureteric enhancement can be seen (B). This was concerning for a possible focal bladder or distal ureteric lesion. A urographic phase was not performed, therefore, specific sloughed papilla findings are difficult to comment on.

Coronal views (A and B) of CT abdomen/pelvis scan (with intravenous contrast) demonstrating the infected and obstructed left collecting system and dilatation of the intramural ureter. The parenchyma of the left kidney is normal and no urinary tract calculi can be seen.
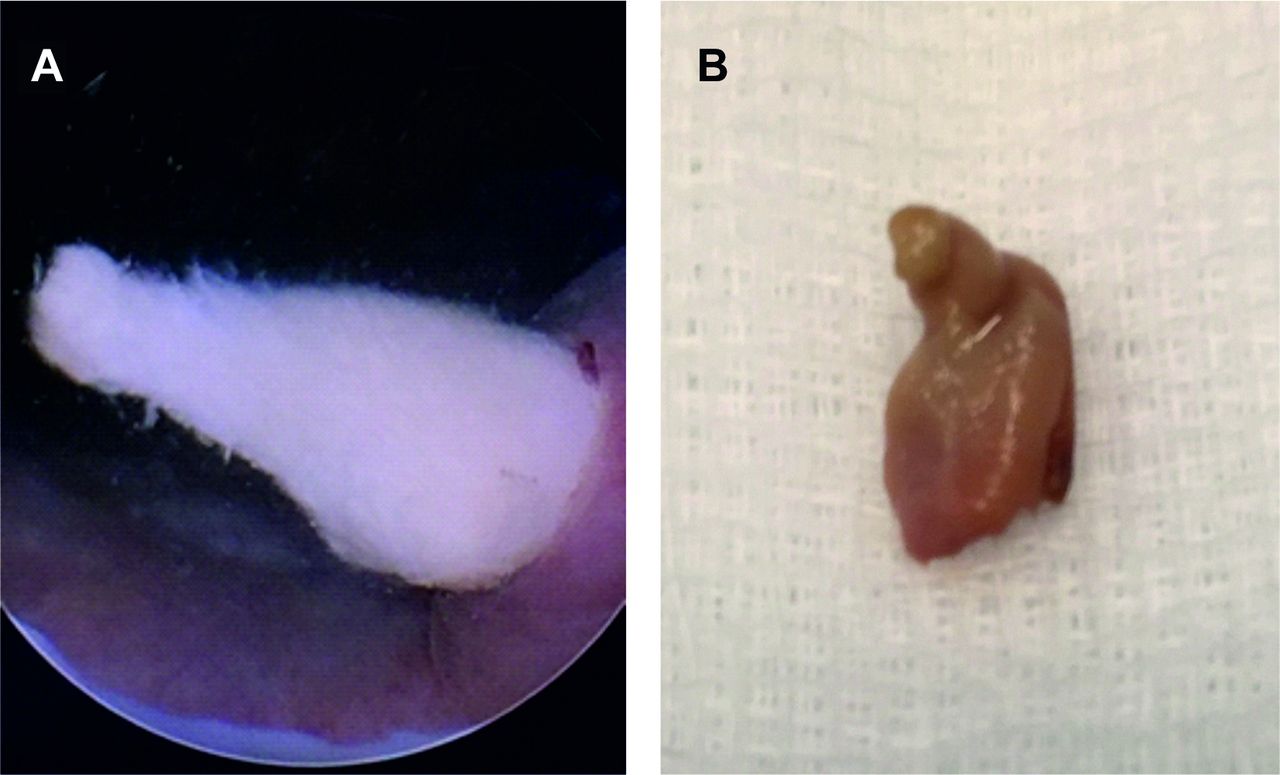
Cystoscopic view (A) of sloughed renal papilla that was seen protruding from the left distal ureteric orifice, which was subsequently removed (B) (firm yellow tissue measuring 9×6×4 mm).

Following removal of the sloughed renal papilla, a ureteric stent (6 French/22 cm) was inserted for relief of the obstruction.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Biopsy taken from the left kidney (A and B) showing necrotic and infarcted tissue (no nuclei are apparent) with ‘ghost’ outlines of renal papillae elements. No malignancy identified (H&E stain, 40x).
Renal papillary necrosis is often associated with sickle cell disease, diabetes, long-term use of analgesics or renal tuberculosis. Passage of sloughed papilla into the ureter may cause renal colic, acute kidney injury or obstruction with or without urosepsis. Radiological findings of papillary sloughing include lobster claw or signet ring appearance of papillary calcifications,1 hydronephrosis or filling defects in the renal pelvis or ureter.2 As in our case, significant sloughing of the papilla can lead to necrotic material causing ureteric obstruction. In the event of intervening sepsis start broad-spectrum antibiotics and insert a ureteric stent for relief of the obstruction. Kamath et al3 reported the successful removal of sloughed papilla in a hydronephrotic transplant kidney using a percutaneous approach. Papillary necrosis and the subsequent migration of a sloughed papilla into the ureter represents an uncommon cause of hydroureteronephrosis but should be considered as a potential diagnosis in patients who present with renal colic, urosepsis or upper urinary tract obstruction, especially when recognised risk factors are present and when imaging fails to identify more common causes such as urolithiasis or neoplasia.
Patient’s perspective
I have been living with diabetes for over 20 years and now I am taking insulin. I was admitted into hospital with abdominal pain with diarrhoea. The doctors first thought this may be related to diverticulitis. However, my kidney function tests became very abnormal. The surprising thing at the time was that I did not have any urinary symptoms. I had the camera test and I felt so much better immediately afterwards and my kidney function tests returned back to normal within a few days. I recovered well after the procedure and I was discharged from the urology team a few months after being followed up. It is believed that this episode was most likely related to my diabetes and I am still being closely monitored by the diabetic team. I do feel that I am now getting better control of my sugar levels than before which is good news. I am keeping a diary and my blood sugar levels are now mainly single figures with a few readings that are double figures. I have also been encouraged to exercise more and remain active to lose weight. I am grateful to both the urology and diabetic teams for what they have done for me over the past year. I am hoping that I will still continue to have good control of my sugar levels to avoid a further episode in the future.
Learning points
Renal papillary necrosis is associated with poorly controlled diabetes and can lead to ureteric obstruction presenting with renal colic, acute kidney injury or urinary sepsis.
In cases of an infected and obstructed kidney, emergency decompression is imperative, and direct visualisation may be required to allow for removal of the sloughed papilla followed by emergency stent for relief of obstruction.
It is essential to gain optimal diabetic control to avoid renal papillary necrosis which could lead to sloughed papilla.
Footnotes
Contributors MGF involved in writing up and final drafting of paper. MC involved in design and revising the manuscript. MB involved in image collection, revising and approving the manuscript for final submission.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.