Article Text

Abstract
Synovial cysts very rarely affect the temporomandibular joint (TMJ). On review of the literature, there are 29 reported cases of unilateral synovial cysts of the TMJ. We present a case of bilateral synovial cysts occurring at the TMJs.
- plastic and reconstructive surgery
- oral and maxillofacial surgery
- otolaryngology/ENT
Statistics from Altmetric.com
Background
Synovial cysts very rarely affect the temporomandibular joint (TMJ). To date, there have been 29 unilateral cases reported in the literature. We report the second bilateral case of synovial cysts occurring at the TMJs.
Case presentation
An 80-year-old woman presented to our plastic surgery service with a 4 month history of a right pre-auricular mass. There was no associated pain or discharge. The mass occasionally fluctuated in size. There was no history of trauma to the area. She was asymptomatic and denied any changes to her dental occlusion or restriction in mouth opening.
On examination, there was a subcutaneous cystic mass present measuring 2×2 cm. This was visible in the right pre-auricular area when her mouth was closed. It was still visible, but less apparent, when she opened her mouth. On palpation, it was fixed to deeper structures.
Investigations
Ultrasound examination was performed which demonstrated appearances in keeping with a bursa arising from the TMJ. An image guided fine needle aspiration was carried out which demonstrated the presence of macrophages, lymphocytes and synoviocytes.
Subsequent MRI examination was performed which demonstrated a very clear communication with the right TMJ (figure 1). In addition, there was evidence of the same process arising from the left TMJ (figures 1 and 2).
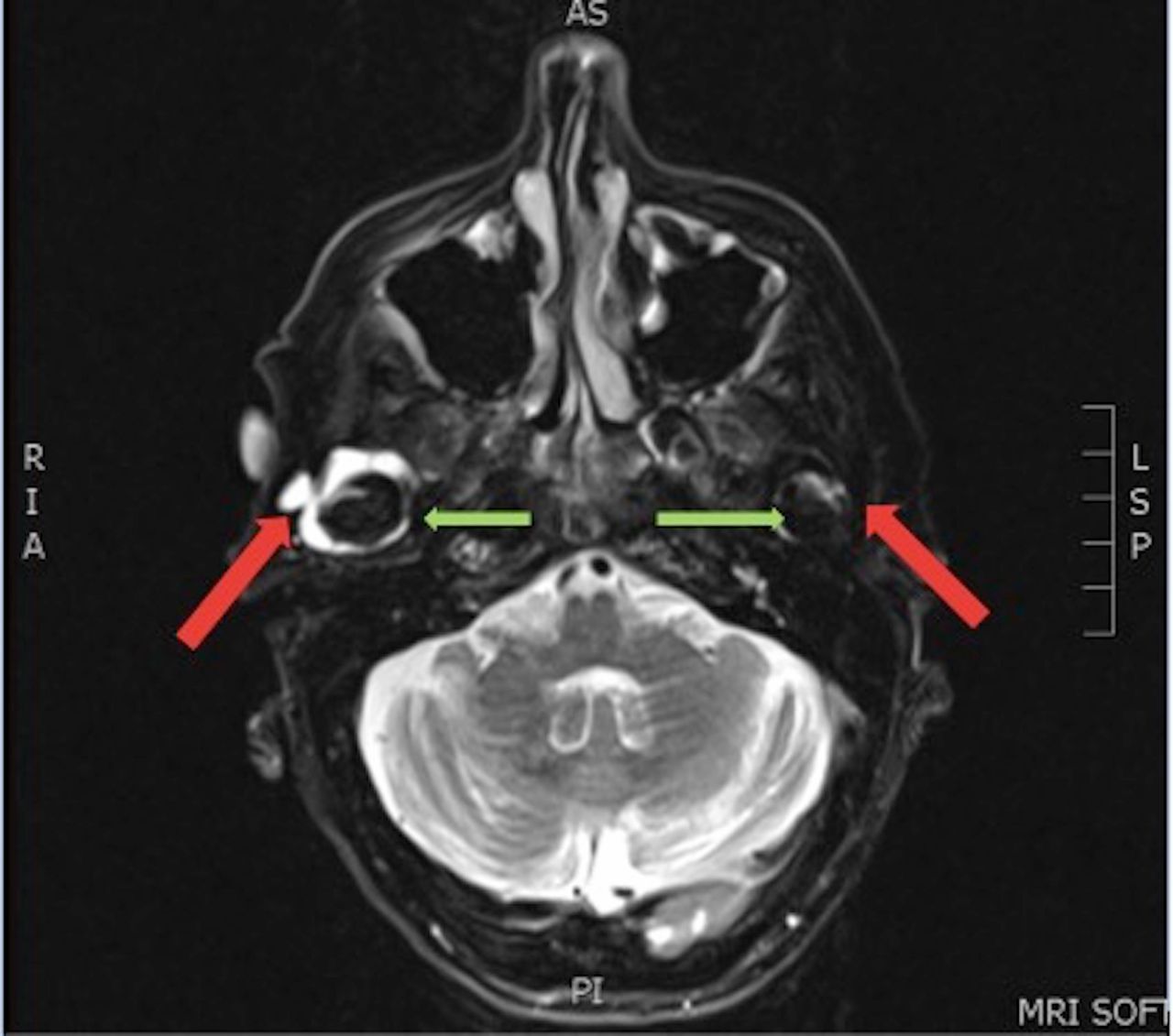
T2 fat suppressed axial MRI with contrast, displaying bilateral synovial cysts of the temporomandibular joints (TMJs). Green arrows: mandibular condyle within the TMJs. Red arrows: neck of synovial cysts.

{kind=link}
{kind=link}
T2 coronal MRI demonstrating bilateral synovial cysts of the temporomandibular joints (TMJs). Green arrows: mandibular condyle within the TMJs. Red arrows: synovial cysts extruding into the soft tissue.
Differential diagnosis
The radiological and cytological findings were in keeping with the diagnosis of synovial cyst affecting both TMJs.
Outcome and follow-up
In keeping with the patient’s wishes, she was managed conservatively without intervention as the right side was asymptomatic and the left side was subclinical. She was asymptomatic and therefore did not require physiotherapy or pharmacological intervention. She was discharged to her general practitioner for follow-up.
Discussion
On review of the literature, there are 29 reported cases of unilateral synovial cysts of the TMJ in the English literature.1–20 This is the second case report of bilateral TMJ synovial cysts.
There was a slight female preponderance (56%), and mean age at presentation was 46 years (range 20–66 years). Our patient was older than those in the reported literature. Table 1 documents the demographics of the patients in all reported cases to date.
Demographics of reported cases of unilateral synovial cysts of the temporomandibular joint
Most patients presented with swelling and/or pain in the pre-auricular area. One patient presented with reduced mouth opening.7 Acute numb lip and chin owing to mental nerve compression from the cyst was the cause of presentation in another case.18 Median symptom duration was 1 year (range 4 days to 5 years). In three of the cases, blunt trauma had preceded the formation of the cyst (4 months to 1 year prior to the onset of symptoms).2 3 5
In total, 87% of patients underwent imaging, with CT and MRI being the the most common modalities (44% and 31%, respectively).
The majority of patients in the case study cohort underwent surgical excision under general anaesthetic. No recurrences were reported. Only one perioperative complication was noted whereby the patient developed asystole owing to a severe trigeminocardiac reflex.20
Differential diagnoses exist for pre-auricular swellings. There can be particular difficulty differentiating a ganglion from a synovial cyst of the TMJ. Maribo et al found that even in the published literature, the terms have been used interchangeably.21 It should be noted that in the other published study claiming to report bilateral synovial cysts, the term was used interchangeably with ganglions.22 Synovial cysts have synoviocytes lining the walls of the cavity. With ganglions, the cells lining the cavity are immunohistochemically different and show signs of myofibroblasts.23 In our case, synoviocytes were found on aspiration, thus diagnosing a synovial cyst. In the case of the other reported bilateral synovial cyst, although the authors referred to them as ganglions in the body of their text, they must be regarded as true synovial cysts owing to the presence of synoviocytes on histological examination.22
In conclusion, synovial cysts of the TMJ should be included in the differential diagnosis of a pre-auricular swelling. This is the second reported case of bilateral synovial cysts of the TMJs.
Learning points
Synovial cyst of the temporomandibular joint is a rare pathology. This is the second known bilateral case.
Patients generally present with a pre-auricular swelling.
Radiological investigations include ultrasound and MRI.
Diagnosis relies on the presence of synoviocytes.
Treatment can be conservative or surgical depending on the severity of symptoms.
References
Footnotes
Contributors All four authors (CB, SB, DS and MO) have contributed to and approved of this submitted manuscript. CB is the submitting author.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Next of kin consent obtained.