


Visual Overview

Abstract
Medical devices are becoming key players on health monitoring and treatment. Advances in materials science and electronics have paved the way to the design of advanced wearable, insertable, and implantable medical devices suitable for the prevention and cure of diseases and the physical or functional replacement of damaged tissues or organs. However, intimate and prolonged contact of the medical devices with the human body increases the risks of adverse foreign-body reactions and biofilm formation. Drugs can be included in/on the medical device not only to minimize the risks but also to improve the therapeutic outcomes. Drug-eluting medical devices can deliver the drug in the place where it is needed using lower doses and avoiding systemic effects. Drug-device combination products that release the drug following preestablished rates have already demonstrated their clinical relevance. The aim of this mini-review is to bring attention to medical devices that can actively regulate drug release as a function of tiny changes in their environment, caused by the pathology itself, microorganisms adhesion or some external events. Thus, endowing medical devices with stimuli-responsiveness should allow for precise, on-demand, regulated release of the ancillary drugs to expand the therapeutic performance of the medical device and also should serve as a first step to offer personalized solutions to each patient. Main sections deal with smart drug-eluting medical devices that are sensitive to infection-related stimuli, natural healing processes, mechanical forces, electric fields, ultrasound, near-infrared radiation, or chemicals such as vitamin C.
Introduction
Human health quality has undergone an unprecedented improvement in the last century, which is evidenced as the decrease in the death ratio at infancy and the much longer life expectation. Such health achievements are mainly associated with better feeding, the prevention of pandemic illnesses through worldwide-distributed vaccines, advances in less-invasive surgical maneuvers under clean conditions, and the development of treatments that turn incurable illnesses into chronic ones or that go to the roots of the illness to reverse it (Fielding, 1999). The strong evolution of pharmacologic and radiotherapy approaches has been critical for these achievements (Heath and Colburn, 2000; Bhide and Nutting, 2010). At present, most health-monitoring systems and treatments involve the use of precisely designed medical devices.
According to the U.S. Food and Drug Administration (FDA), medical devices comprise a large variety of instruments, apparatuses, implants, and in vitro reagents intended for the diagnosis, prevention, or cure of diseases or to affect the structure or any function of the body, which do not achieve any of their primary intended purposes through chemical action. Such (bio)chemical action has been restricted to the medicaments (FDA, 2018b). Flash glucose monitoring systems; versatile stents that allow simultaneous diagnostic and therapeutic maneuvers, particularly in the gastrointestinal organs; devices that trap blood clots and help reduce stroke risk; noninvasive devices that allow assessment of head injuries at point-of-care; test devices for solid tumors that help make immunotherapy decisions; advanced dermal regeneration matrices that can regenerate native tissues, particularly intended for diabetic ulcers; breast imaging devices that offer high-contrast, real, three-dimensional (3D) images of all structures; implantable drug infusion pumps that precisely deliver the correct amount of drug needed at each time; and sensors inside oral medicines that track whether the medication has been taken and send the information to a smartphone app or web portal, among others are not a dream. All these are already counted in the list of the most innovative medical devices (Kirsh, 2018). Advances in materials sciences and electronics are behind sophisticated, wearable medical devices that allow continuous monitoring of certain physiologic functions for diagnosis or of pharmacologic levels of therapeutic substances for efficient personalized treatments (Yetisen et al., 2018).
Despite these achievements, the use of medical devices carries the intrinsic risk of causing adverse foreign-body reactions or other side effects from the adherence of the user’s proteins and cells or from the proliferation of microorganisms (Anderson, 2001). Medical devices are categorized into three classes according to their intended use and the risk they may pose to the patient or the user. Invasiveness increases these risks, so devices intended to penetrate the body and remain in contact with or inside the body for prolonged time should follow very strict rules. Yet adverse events remain common; for example, restenosis associated with vascular stents (Iqbal et al., 2013), posterior capsule opacification associated with intraocular lenses after cataracts surgery (Nibourg et al., 2015), or biofilm formation on urinary catheters, bone prostheses, or central venous catheters with the subsequent infection spreading in host tissues (De Angelis et al., 2010; Wallace et al., 2017) affect a relevant percentage of patients and have had a strong economic impact on health care systems.
The evolution of materials science has been enormous in improving the performance and safety of medical devices (Teo et al., 2016), but in most cases the risks have been strongly minimized by combinations with the right drugs (Couto et al., 2012; Alvarez-Lorenzo et al., 2017). Systemic treatments prescribed to patients wearing medical devices still have relevant untoward effects—for instance, the risk of respiratory and gastrointestinal disorders associated with postimplantation pain and inflammation treatment, bleeding events due antithrombosis therapy after the implantation of stents or other blood-contact biomaterials, or emerging microbial resistance from using prophylactic antimicrobial therapy (Bhusal et al., 2016; Reviakine et al., 2017).
As an alternative, the advantages of incorporating the drug on/in the medical device itself are clear. The drug is delivered in the place where it is needed (usually a place that is hardly accessible through a systemic route), which lowers the amount required (lower dilution, fewer barriers, and slower clearance); the device itself may adjust the release to the therapeutic demands. This strategy increases both efficiency and safety, and it is not dependent on patient compliance (Wenke and Guelcher, 2011; Bhusal et al., 2016; Cyphert and von Recum, 2017; Sanchez-Rexach et al., 2017). However, endowing medical devices with the drug-delivery performance is not a simple task because most materials do not uptake sufficient amounts and/or do not regulate the release according to the therapeutic needs (Alvarez-Lorenzo and Concheiro, 2013; Lee et al., 2017).
The increasing demand for medical devices with improved or even novel performance parameters has blurred the boundary between medicaments and medical devices. Historically, pharmaceutical companies have been drug-centric and the medtechs have been technology device-centric; however, both sectors have joined in offering patient-centric approaches with a strong life-changing impact. Indeed, the definition of medical device provided by the World Health Organization (WHO) is now wider: even if a medical device does not achieve its primary mode of action by pharmacologic, immunologic, or metabolic means, it may be assisted in its intended function by such means (WHO, 2018). In this regard, combination products have appeared as a novel, broad regulatory category, which includes any binary or ternary combination of a drug, biologic product, and/or device (Alvarez-Lorenzo and Concheiro, 2013; FDA, 2018c).
Drug–device combination products in which the device is responsible for the primary mode of action—it makes the greatest contribution to the overall intended therapeutic effects, while the drug performs as an ancillary medicinal substance—are commonly known as drug-eluting devices or drug-enhanced device products. Drug-eluting stents (DES) are a clear example of the strong research in this field (Huang et al., 2014). The use of coronary bare-metal stents remarkably reduced the mortality associated with coronary artery diseases, but the risk of failure due to in-stent restenosis was approximately 30% patients (Holmes, 2003). The first-generation DES, introduced in 2002, relied on antiproliferative agents incorporated into a polymer coating that regulated the release. This product can be considered as the first regulated drug–medical device combination product (Simard et al., 2014).
Nevertheless, coatings with nonbiodegradable polymers (first generation) or thinner inorganic composites (second generation) trigger inflammatory responses that cause late stent restenosis. Biodegradable coatings (third generation) may attenuate some of the untoward events, but the polymer itself may still be responsible for adverse immune reactions. Thus, current efforts are focused on polymer-free stents that can still regulate drug release through a very precise design of the topology of the stent surface and a slowdown of intrinsic solubility rate of the drug (Acharya and Park, 2006; Sanchez-Rexach et al., 2017; Kommineni et al., 2018; Konishi et al., 2018). Some of these fourth-generation DES as well as several other drug–device combinations products are already in the market (Table 1).
Common examples of commercially available devices coated/impregnated or otherwise combined with drugs according to FDA classification of combination products. The device has an additional function in addition to delivering the drug (FDA, 2018c).
It should be noted that the drug can be included in the matrix of the device during fabrication, layered as a coating in a subsequent step, or placed into a specific reservoir. The two latter options are preferred for labile ancillary drugs or for matrices whose mechanical properties may be affected if the drug is incorporated (Raval and Parikh, 2010).
This mini-review revisits the recent advances in medical devices that can actively regulate drug release as a function of tiny changes in their environment caused by the progression/remission of the pathology, the growth of microorganisms, or some external events. Thus, in contrast to medical devices (such as stents) that release the drug in a sustained, preestablished rate, as reported elsewhere (Zilberman and Elsner, 2008; Concheiro and Alvarez-Lorenzo, 2013), the following sections deal with medical devices endowed with stimuli-responsiveness as a tool for efficient drug loading and elution as a function of specific demands.
Medical devices made of materials that can modify their properties as a function of stimuli coming from inside or outside the body have been attracting a great deal of attention. As a relevant example, strong efforts are been made in the design of 3D architectures for implantation with properties that evolve over time. These four-dimensional systems may offer advantages in terms of shape-memory that facilitates the implantation through minimally invasive maneuvers and adapts to the required shape once placed in the patient (Oliver et al., 2016; Antony et al., 2017). Similarly, hydrogels, which undergo phase volume transitions (e.g., modify the swelling) as a function of tiny changes in certain variables in the body, have found application as chemical sensors and soft actuators (Ikeda et al., 2014; Yoshida et al., 2018).
A step farther is to exploit such stimuli-responsiveness for a precise, on-demand regulated release of the ancillary drugs to expand the therapeutic performance of the medical device and attenuate its risks. Smart drug delivery by means of nanocarriers has been widely reported (Alvarez-Lorenzo and Concheiro, 2014), but stimuli-responsive drug release from medical devices has yet to be fully explored (Alvarez-Lorenzo and Concheiro, 2013). Smart drug eluting devices may offer novel ways of addressing unmet clinical needs and may open the path to truly custom/personalized medical devices (Fig. 1).

Internal and external stimuli evaluated to trigger ancillary drug release from medical devices and main outcomes expected.
Infection-Responsive Antimicrobials-Eluting Medical Devices.
Medical devices are prone to microorganism contamination not only before implantation via contact with the skin or mucosa of the patient but also after implantation if latent microorganisms migrate from infection focuses in other parts of the body (Percival et al., 2015). The settling of microorganisms on a medical device usually evolves as biofilm formation: a highly structured community undergoes phenotypic changes mediated by a quorum sensing communication mechanism that makes the microorganisms highly resistant to conventional antimicrobial agents (Remy et al., 2018). Thus, once a biofilm has formed, its eradication is difficult; the risk of it spreading to other tissues through bloodstream is high and could compromise the patient’s life. Implantable medical devices are responsible of almost 50% of nosocomial infections (WHO, 2011).
Even in a less acute situation, biofilm formation may compromise the mode of action of the medical device; for example, biofilms may block catheter flow (Jones et al., 2005) or delay the natural healing of wounds if they colonize either the suture or the adjacent tissue (Hong et al., 2018). Various bone cements that incorporate antimicrobial agents are already on the market, but they usually release most of their drug on the first day, followed by sustained elution of sometimes subtherapeutic doses, which may compromise the prophylactic role (King et al., 2018).
Because the prolonged release of antimicrobials may cause adverse events and favor antimicrobial resistance (McLaren, 2004), a variety of stimuli-responsive polymers have been tested for the development of drug nanocarriers capable of site-specific delivery of antimicrobial agents in the infection location. More recently, they have been used to adorn medical devices with networks that release the antimicrobial agent only if the colonization occurs (Alvarez-Lorenzo et al., 2016; Cyphert and von Recum, 2017; Wei et al., 2019).
Infection-responsive (or bacteria self-defensive) medical devices rely on three main mechanisms: 1) coatings responsive to the changes in enzymes and pH associated with microbial growth; 2) surfaces that expose contact-killing moieties in the presence of the microorganisms; and 3) bioinspired moieties that release the antimicrobial agent through a competitive mechanism with the microorganism wall (Fig. 2). Specific examples are summarized in Table 2.

Main mechanisms explored so far to endow medical devices with self-defensive behavior against biofilm formation. (A) Coatings that switch antimicrobial drug release on/off in response to enzymes and pH changes associated with microbial growth. (B) Contact-killing moieties that activate in the presence of microorganisms. (C) Bioinspired moieties that resemble natural receptors of the microorganisms and transfer the antimicrobial agent through a competitive mechanism.
Examples of infection-responsive antimicrobial-eluting medical devices
The design of wound dressings that can simultaneously favor healing and prevent infections has received a great deal of attention as well. For example, electrospun mats of poly(lactic-co-glycolic) acid (PLGA) can degrade faster—and thus release their encapsulated drugs more rapidly—as microorganisms grow and release lipolytic esterases. As demonstrated for Pseudomonas aeruginosa, Staphylococcus aureus standard strain, and methicillin-resistant S. aureus (MRSA1), biofilm formation on electrospun mats causes the hydrolysis of PLGA and thus the release of fusidic acid, which in turn leads to the killing of the bacteria (Said et al., 2011). The benefits of this approach have been demonstrated both in vitro and in vivo (Said et al., 2012). Also poly-l-lysine coatings have been shown to be degradable by chymotrypsin, showing bacterial infection-dependent release of gentamicin (Xu et al., 2017).
Bacteria growth is also associated with changes in the surrounding pH, which can be exploited as a stimulus to trigger drug release from the medical devices (Pavlukhina et al., 2014). In this regard, layer-by-layer coatings of oppositely charged polymers and antimicrobial agents have been shown to rapidly disassemble in response to the drop in pH that occurs as Staphylococcus epidermidis or Escherichia coli grow and generate lactic acid and acetic acid, respectively. The films can be designed to not release the drug at pH 7.4, but to efficiently elute the antimicrobial agent as the surroundings become acidic, which causes bacteria eradication (Zhuk et al., 2014). Nevertheless, pH-responsive systems may not discriminate between the drop in pH associated with bacteria growth and that caused by the migration of macrophages to the implantation site after surgery. Further in vivo studies are required to examine these conditions.
Changes in pH also can be exploited to trigger the release of antimicrobial agents immobilized on the device surface. The surface of medical devices can be easily modified with poly(acrylic acid) (PAA) by use of either plasma polymerization or gamma-ray grafting approaches; PAA-grafted chains act as intermediates for binding cationic drugs through strong ionic interactions (Mendes, 2008; Alvarez-Lorenzo et al., 2010). Remarkably, changes in pH in the typical range of microorganism growth may reverse the affinity and thus trigger the release of the drug, as demonstrated for vancomycin and antimicrobial peptides (Ruiz et al., 2008; Muñoz-Muñoz et al., 2012; García-Vargas et al., 2014; Traba and Liang, 2015). In case of the lytic peptide agents, their direct transfer from the device to the bacteria membrane and the increase in their activity as the pH decreases strongly contributes to the inhibition of biofilm formation (Traba and Liang, 2015).
Interestingly, PAA grafts also allow for the spontaneous formation of gold nanoparticles on the surface of the medical devices, which opens the way to near-infrared (NIR) responsive photothermal ablation of biofilm (Cabana et al., 2017). Grafting of cationic polymers has been explored for loading anionic antimicrobial agents (Contreras-García et al., 2011). Also, antimicrobial agents covalently linked to the medical device through labile bonds have shown pH-responsive release in media mimicking bacteria growth (McCoy et al., 2016).
Urease-producing microorganisms cause an increase in the pH of urine, which may lead to salt deposition on the lumen of catheters and their blockage. To prevent this phenomenon, urinary catheters have been coated with a reservoir containing bacteriophages with a sealing layer of pH-responsive Eudragit S100. The coating is stable in the presence of urease-negative bacteria but provides a burst release of bacteriophages in the presence of Proteus mirabilis, which in turn causes a significant decrease in bacteria cells and doubles the time required until blockage (Milo et al., 2017).
Using a similar approach, pH-responsive coatings have been recently developed to act as infection-responsive theranostic materials. Layers of PAA and chitosan-trapping ciprofloxacin, sealed with Eudragit S100, have been designed to undergo distinct chromatic color transitions from blue to purple and red as the pH becomes more alkaline, acting as a sensor for early infection and also as a warning of the risk of blockage. Moreover, the pH-responsive release of the antimicrobial agent notably decreased bacterial growth in an in vitro infected bladder model (Zhou et al., 2018).
A second family of self-defensive materials relies on the design of surfaces that trap microorganisms and kill them through immobilized biocide groups (Luna-Straffon et al., 2014; Huang et al., 2015). Contac-killing surfaces have been prepared that combine the temperature-responsive poly(N-isopropylacrylamide) (PNIPAAm) with biocidal quaternary ammonium salts. At 37°C, PNIPAAm brushes are shrunken, and the biocidal groups protrude on the surface. Thus, bacteria that adhere to the surface through hydrophobic interactions are exposed to the biocidal agent. The killed bacteria can be removed from the surface by washing in water at temperature below the low critical solubility temperature of PNIPAAm (Pavlukhina et al., 2012). The surface also can be designed to exhibit the opposite performance: oligo(ethylene glycol) methacrylates conjugated with antimicrobial peptides show a swelling-collapse transition at 35°C. Below this temperature, bacteria can freely enter into contact with the peptide, and the bactericide effect occurs. At 37°C, the ethylene glycol moieties predominate, and the material becomes a bacteria repellent (Laloyaux et al., 2010). Also pH-responsive polymer brushes such as poly(2-ethylacrylic acid), poly(2-n-propylacrylic acid), and poly(2-n-butylacrylic acid) have been shown to exhibit contact-killing capability under acidic conditions (Lu et al., 2015).
The third mechanism relies on bioinspired strategies to host the antimicrobial drug and to trigger its release through a competitive mechanism when the microorganisms are present. The small structural differences between cholesterol (a structural component of mammalian membranes) and ergosterol (present in fungi walls) are the basis of the discovery of a relevant family of antifungal drugs. Polyenes, azols, and allylamines selectively interact with fungi, blocking their growth while remaining innocuous for mammalians. Thus, applying ergosterol on medical devices has been investigated as a way to endow the surface with the capability of hosting therapeutically efficient amounts of antifungal agents and of retaining them at physiologic pH without leakage; the release is triggered when a fungal infection has been mimicked (Segura et al., 2014). Tests performed in the presence of Candida albicans showed the fungi-responsive, ergosterol-functionalized devices efficiently inhibited biofilm formation.
A different approach was explored with cyclodextrin-functionalized wound dressing. Cyclodextrins have the ability to host quorum-sensing inhibitors and antimicrobial agents forming inclusion complexes, and they also can host quorum-sensing signaling molecules—that is, the molecules released by bacteria to communicate with each other and develop biofilm (Okano et al., 2016). Thus, cyclodextrin-functionalized gauzes were successfully loaded with hamamelitannin (a quorum-sensing inhibitor) and vancomycin, and then they were exposed to S. aureus monospecies biofilm and to S. aureus plus Pseudomonas aeruginosa mixed biofilm mimicking a chronic wound infection. Relevantly, the loaded gauzes decreased biofilm formation and increased bacteria susceptibility toward vancomycin in both biofilm types. The release of the active ingredients was favored by the presence of the quorum-sensing signaling molecules due to competitive mechanisms for forming inclusion complexes with the cyclodextrins (Brackman et al., 2016).
Drug-Eluting Medical Devices for Smart Regenerative Medicine.
In addition to infection prevention, orthopedic implants, vascular grafts, and other medical devices intended for tissue regeneration demand the release of active substances that can mimic the natural cascade that takes places during the natural healing process (Bagherifard, 2017). Strong efforts are being made to create synthetic devices that can stabilize the site of injury, with mechanical properties similar to the tissue to be repaired and an architecture that allows host-cell colonization. Encouraging the adhesion of specific cell types and their further growth should be carefully driven toward efficient regeneration that avoids scarring or unnecessary healing delays (Winkler et al., 2018).
Any injury triggers a healing cascade that involves three phases: inflammation, proliferation, and maturation, with the participation of different cells. Migration of inflammatory cells is essential for healing because they not only remove bacteria and foreign materials but also release critical enzymes and cytokines for the subsequent phases. However, an excessive, prolonged inflammation may delay the healing, degrade the scaffold, and provoke fibrosis and scarring. Thus, the inflammation-triggered release of anti-inflammatory drugs has been been explored as a way of recapitulating natural tissue regeneration. For example, the covalent grafting of nonsteroidal anti-inflammatory drugs (NSAIDs) via ester groups to hydrogel coatings or electrospinnable components has been shown to be useful in regulating NSAID release as a function of overexpressed esterases (Pan et al., 2015; He et al., 2017) (Table 3).
Examples of stimuli-responsive release from scaffolds for regenerative medicine
The next regeneration steps require the sequential release of adequate growth factors for cell proliferation and differentiation. Thus, a variety of strategies are being explored for, commonly, dual delivery of growth factors at different time points or release rates (Izadifar et al., 2015). Although most approaches rely on coatings that encapsulate a given growth factor and release it at a preestablished rate, some evidence of the potential of stimuli-responsive release has been already published (Bruggeman et al., 2018). The relevant examples are summarized in Table 3. External modulation of the release can be achieved by engineering acoustically responsive scaffolds; the scaffolds contain different growth factors in differently designed sonosensitive emulsion droplets, and each droplet releases the content at different acoustic pressures. Thus, precise spatiotemporal control of the release of each growth factor is possible (Moncion et al., 2018). The feasibility of this approach has been already demonstrated in vivo (Moncion et al., 2017). Release that is responsive to magnetic fields has been observed for hydrogels encapsulating magnetic particles and platelet lysates: the application of an external magnetic field can modulate the release of the growth factors, which in turn determine cell expression and the synthesis of tendon-and bone-like matrices (Silva et al., 2018).
Recent research has focused on cell-responsive remodeling of the scaffolds in such a way that specific cell inputs may trigger the release of the adequate growth factor at each time (Murphy and Lampe, 2015). Metalloproteinases released by the cells can regulate the degradation of certain scaffold components and thus the release of encapsulated active substances. Metalloproteinases can also break the labile bonds of growth factors tethered to the scaffold (Van Hove et al., 2015). Also, cell-produced heparinase has been evaluated as a stimulus for the release of growth factors bound to the scaffold through heparin moieties. Heparin has a high affinity for many growth factors, and the dissociation (passive release) is quite slow under physiologic conditions (Martino et al., 2013; Vulic and Shoichet, 2014). Thus, it has been shown that cells may mediate much faster release of the growth factors, which in turn determine the subsequent cell development (Sakiyama-Elbert and Hubbell, 2000).
Foreseeably, the advent of 3D printing technologies makes the design of medical devices with precise locations for active molecules and responsive materials to construct truly dynamic, cell-responsive, or externally activated scaffolds in the near future (Nadgorny and Ameli, 2018).
Mechanically Activated Drug Release.
Medical devices inserted or implanted in the body are subjected to physiologic stress and are also susceptible to the action of externally applied forces. A variety of strategies have been explored to trigger drug release using the common mechanical stimuli of compression, tension, and shear (Fig. 3). Physiologic mechanical stimuli and the principles behind the design of mechano-responsive drug delivery systems have been recently reviewed elsewhere (Wang et al., 2017), and relevant examples are summarized in Table 4.
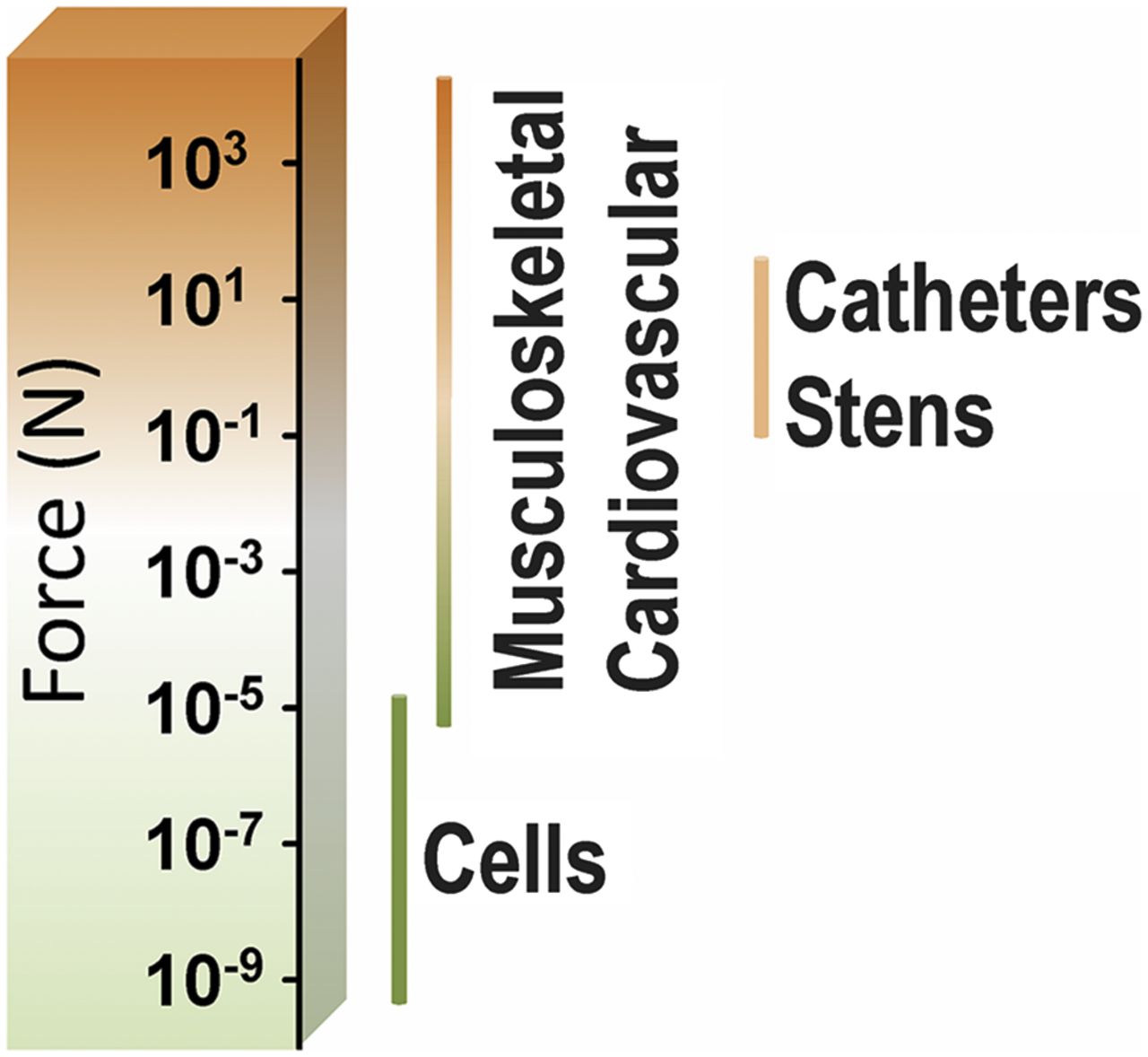
Magnitude of the physiologic and external forces that can be exerted on medical devices. Data taken from Wang et al. (2017).
Examples of mechanically activated drug release from medical devices
Compressive medical devices are formed by elastomers (viscoelastic materials) that withstand compressive loadings. Compression may allow the release of a certain amount of drug through a squeezing-like mechanism. For example, wound dressings that elute hydrocortisone in response to mechanical stimuli have been designed from alginate hydrogels bearing grafted cyclodextrins. The responsiveness has been attributed to changes in the conformation of the cyclodextrin cavity and the hydrogel network as function of the pressure, which impels the release of the drug from the cyclodextrin cavity and thus accelerates the diffusion out of the hydrogel (Tan et al., 2015). Also, soft contact lenses containing either drugs or comfort ingredients are being designed to release these hydrophilic components toward the cornea surface during blinking (Galante et al., 2015). The pressure of the eyelid on the hydrogel surface combined with the shear stress (dragging components from the contact lens surface) may allow for a pulsate release of the lubricating macromolecules, making wearing the lenses more comfortable and minimizing the risk of dry eye symptoms (Alvarez-Lorenzo et al., 2019).
Tension forces are typical of stents. Several layered composite systems have been reported useful for achieving tension-driven drug release. Stretching of polyelectrolyte films can open nanopores, which act as nanovalves that allow the exit of the drug but close when the film is at rest (Mertz et al., 2007). Similarly, drug-loaded polymer layers coated with a thin titanium layer develop micro-sized cracks when subjected to external tensile strains. The crack area is proportional to the applied strain, and the cracks perform as channels for drug release (Jeon et al., 2018). A different strategy relies on the coating of esophageal stents with superhydrophobic multilayers containing drug-loaded microparticles; the crack propagation of the superhydrophobic coating can be triggered by physiologic forces that facilitate the entrance of the release medium in the coating, thus releasing the drug from the microparticles. The release of both hydrophobic and hydrophilic drugs has been shown to be dependent on the applied strains (Wang et al., 2016, 2018).
Also, stretching may accelerate the release of antimicrobial agents from hydrogels prepared with cyclodextrin monomers. Once again, the deformation of the cyclodextrin cavity drives the release of the previously encapsulated drug molecule (Ballance et al., 2018). Intriguingly, deformable catheters have been tested for the removal of preformed biofilms using strain forces. C. albicans biofilms have been detached from prototypes by selectively inflating the inner chambers, which causes strain on the surface (Maskarinec et al., 2018).
Shear-forces are particularly relevant in the cardiovascular system, and large increases in shearing occur when the vessels become narrow due to physiologic or pathologic events (e.g., atherosclerotic plaques or clots) (Saxer et al., 2013). Indeed, direct correlations between sirolimus release from PLGA films and flow rate of the medium have been found, which may have an impact on DES (Zheng et al., 2017). Nevertheless, much knowledge is still required to reproduce in vitro biorelevant conditions of blood flow (Reviakine et al., 2017).
Electric-Responsive Release.
Natural mechanical stimuli can be transformed into electrical stimuli that trigger drug release from a medical device. As a proof of concept, disposable gastric lavage tubes were coated with a piezoelectric network made of poly(vinylidene fluoride-co-hexafluoropropylene) and reduced graphene fillers (PEI-rGO/PVDF-HFP). On these were subsequently deposited a polyamidoamine (PAMAM) dendrimer able to host a variety of drugs, including the antiemetic metoclopramide. Pressure on the gastric lavage tube mimicking human swallowing force (7–10 kPa) was transformed by the piezoelectric network into an electrostatic field (2.7 V) to accelerate drug release. The purpose was the attenuation of nausea to facilitate the intubation process itself. The release rate under the mechanical stimulus was approximately 2-fold the rate recorded at rest. In addition to the wavelike motion of the esophagus, manual deformation of the external portion of the gastric tube caused a similar effect on drug release, and the generated voltages remained in the safe interval for the human body (Zhang et al., 2018).
A different approach consists in exploiting the electrical fields generated by some implantable medical devices during their normal functioning. For example, cochlear implants restore a functional level of hearing to profoundly deaf individuals by means of the electrical stimulation of spiral ganglion neurons. The device involves an electrode array that is implanted into the scala tympani of the cochlea. However, the continuous electrical discharges to activate the central auditory pathways may exacerbate the loss of more hair cells (responsible for the sensorineural deafness), causing the apoptosis of more neurons. This untoward effect may be solved by coating the electrodes with a conductive polymer layer containing therapeutic neurotrophins. The generated electrical stimulus increases the release of the neurotrophic proteins, increasing the biocompatibility (Richardson et al., 2009; Thompson et al., 2010, 2011).
Also, cochlear implants have been combined with gene therapy to stimulate spiral ganglion neurite regeneration. The electrode array was arranged to create a close-field electroporation for efficient transduction of adjacent mesenchymal stem cells. The regenerated neurites improved the auditory response (Pinyon et al., 2014).
Other Stimuli.
As mentioned with biofilm eradication, immobilization of gold nanoparticles on medical devices allows exploiting their NIR sensitiveness. Therefore, irradiating with an external source of NIR may cause local heating, useful for direct thermal ablation of cells (tumor cells, proliferative cells, bacteria) but also for the controlled release of drugs encapsulated in temperature-responsive materials. This strategy has been investigated for esophageal stents implanted to prevent tumor recurrence with combined gold nanoturfs and doxorubicin (Fig. 4) (Lee et al., 2018).
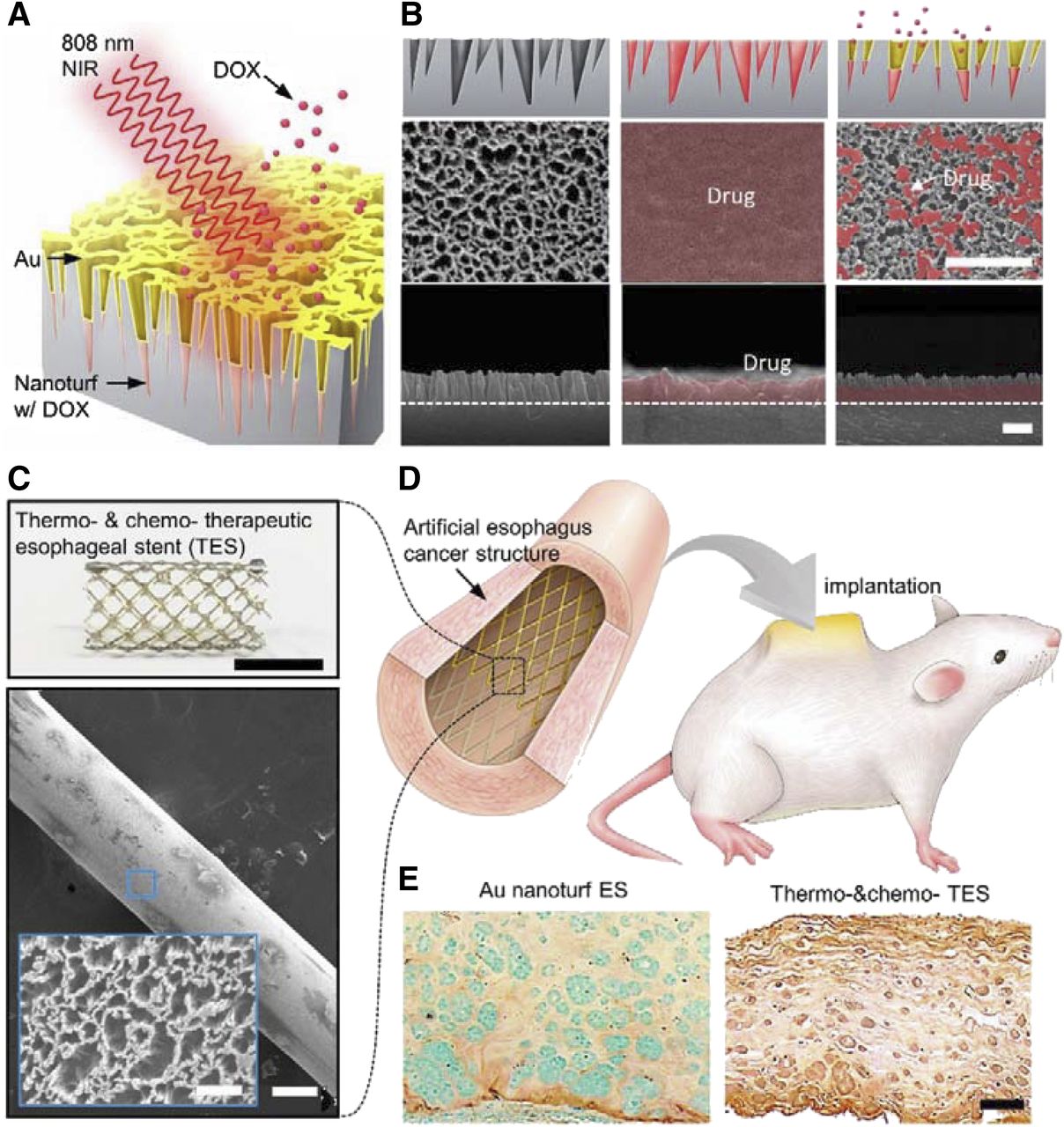
Structure and performance of an esophageal stent coated with a nanoturf structure containing gold (Au) and doxorubicin (DOX) for combining thermotherapy and chemotherapy. (A) Near-infrared (NIR) responsiveness of the Au coating triggers localized increase in temperature while DOX is being released. (B) SEM images of pristine (left), DOX/Au-coated (middle), and partial drug release (right) nanoturf structures, after incubation in PBS solution for 6 hours. Scale bar: 1 μm. (C) Appearance and surface structure of a nitinol wire stent coated with the nanoturf structures. (D) The esophageal stent covered with an esophagus-mimicking organoid tube prepared for subdermal implantation. (e) TUNEL stains of esophagus-mimicking organoid tubes treated with the nanoturf esophageal stent containing only Au (left) or DOX and Au (right) after NIR irradiation in vivo. Live cells are shown in blue and apoptotic cells in brown. Scale bar: 400 μm. Reprinted with permission from Lee et al. (2018). Copyright (2018) American Chemical Society.
Finally, vitamin C has been shown to be useful for deactivating the adhesion of dressings to wounds to facilitate their peeling from damaged skin without causing a secondary trauma. Such vitamin C responsiveness relies on its capability to disassemble the protein supramolecular structures contained in the wound dressings (Zhao et al., 2018). This capability could be also exploited for triggering the release of encapsulated drugs.
Conclusions
Medical devices that can precisely regulate the time at which the ancillary drug should be released offer undoubted advantages over devices designed for a preestablished release rate. The amount of drug that can be hosted by the medical devices is limited (because of limited affinity and also to avoid changes in bulk properties), so regulating the moment at which the drug is delivered is critical for maximizing its prophylactic/therapeutic performance. Smart drug-eluting medical devices have benefited from the knowledge gathered on stimuli-responsive drug nanocarriers.
Additional specific stimuli can be exploited in the case of medical devices. Cell-triggering release of growth factors from orthopedic implants may determine the fate of both the cells and the implant, allowing for optimized healing. Or natural physical forces exerted onto the medical device can directly, or by previous transformation into an electric field, act as efficient stimuli to release drugs that can either minimize untoward reactions (e.g., emesis) or help restoring natural functions (e.g., hearing).
Advances in materials science and pharmaceutical technology together with deeper knowledge about the physiologic variables that can serve as stimuli make foreseeable upgraded medical devices that are more sensitive and robust in the release response and may even have theranostic capabilities. Such devices could play a key role in the health care system in the near future.
The incorporation of drugs into medical devices to create device-led combination products adds complexity to the regulation pathway, compared with solely medical device products. Nevertheless, the efforts that are being made by the regulatory agencies to clarify the premarket pathways are very valuable (Office of Combination Products, 2019).
Authorship Contributions
Performed data analysis: Alvarez-Lorenzo, Concheiro.
Wrote or contributed to the writing of the manuscript: Alvarez-Lorenzo, Concheiro.
Footnotes
- Received February 8, 2019.
- Accepted April 1, 2019.
This work was funded by MINECO [SAF2017-83118-R], Agencia Estatal de Investigación (AEI) Spain, Xunta de Galicia [Grupo de Referencia Competitiva ED431C 2016/008; Agrupación Estratégica en Materiales-AEMAT ED431E 2018/08], and FEDER (Spain).
Abbreviations
- 3D
- three dimensional
- DES
- drug-eluting stents
- FDA
- U.S. Food and Drug Administration
- NIR
- near-infrared
- NSAIDs
- nonsteroidal anti-inflammatory drugs
- PAA
- poly(acrylic acid)
- PLGA
- poly(lactic-co-glycolic) acid
- PNIPAAm
- poly(N-isopropylacrylamide)
- Copyright © 2019 by The American Society for Pharmacology and Experimental Therapeutics





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}