




Abstract
This report aimed to scrutinize the prevalence of Behçet’s disease (BD)-related clinical manifestations based on age- and sex-specific subgroups using a Japanese nationwide registration database.
The database of newly registered BD was obtained from the Japanese Ministry of Health, Labour and Welfare. Patients who met the International Criteria for Behçet's Disease were selected and analysed.
Among 6627 International Criteria for Behçet's Disease cases, 2651 (40.0%) were men and 3976 (60.0%) were women with a median age of 39 years (interquartile range: 31–50 years). Ocular lesion was more common in male [odds ratio (male: female) 2.64 (95% CI: 2.35, 2.95, P < 0.001)] and genital ulceration was more common in female (odds ratio = 0.29, 95% CI: 0.25, 0.32, P < 0.001). Ocular lesion (P < 0.001), arthritis (P < 0.001) and vascular lesions (P < 0.001) were more frequently observed in elderly registered patients. Contrarily, genital ulceration (P < 0.001), epididymitis of males (P = 0.023) and oral ulceration (P = 0.003) were more common in younger patients. Simultaneous assessment of sex and age revealed that male predominance of ocular involvement was found in the young adult generation, but not in patients over 70 year of age. A female predominance of genital ulcer was prominently observed in patients 20–59 year of age; however, the sex difference was not found in patients over 60 years of age. Sensitivity analysis using International Study Group criteria replicated the results.
We showed that clinical phenotype in early phase of BD was different depending on onset age and sex.
Rheumatology key messages
Male predominance of ocular involvement in Beçhet’s disease was found in the young adult generation only.
Female predominance of genital ulcer in Beçhet’s disease was prominently observed in patients 20–59 year of age.
Introduction
Behçet’s disease (BD) is a chronic immune-mediated disease characterized by mucous membrane ulceration and ocular involvement. The disease has a broad spectrum of clinical phenotypes. Some of the patients suffer from vascular, intestinal and neurological manifestations, which are sometimes fatal, whereas mild mucocutaneous symptoms are predominant in others. Asian and Mediterranean residents, especially in their 30s and 40s, are most frequently affected by this disease [1, 2]. Populations in these areas are probably at higher risk of BD because of genetic, epigenetic and environmental factors. Genome-wide association studies have identified some of the genetic loci responsible with polymorphisms that predispose to BD [3]. However, this genetic information accounts for a small part of susceptibility to BD, suggesting a large component of environmental or epigenetic influences [3–6]. A meta-analysis revealed that the pooled odds ratio of HLA-B51/B5 allele carriers to develop BD compared with non-carriers was 5.78 (95% CI: 5.00, 6.67) [7].
Sex differences in BD presentation have been one of the major topics of BD epidemiology, and a large number of epidemiological studies have been conducted to reveal these. The prevalence of BD was found not to be very different between men and women, whereas that of each symptom showed a clear difference between the sexes. A systematic review in 2014 by Bonitsis et al. [8] meta-analysed data on more than 10 000 patients from 53 reports [8] and clarified the sex difference in BD symptoms. However, it is important to consider the age factor in discussing sex differences, because, besides sex chromosome gene products, the differences are mainly caused by the sex hormone environment in those of reproductive age. In principle, genetic factors contribute to disease phenotype more prominently in young onset patients than elderly ones for any disease [9]. The disease manifestations appear early in life in most of the hereditary diseases caused by a single gene mutation [10]. On the contrary, elderly individuals are more exposed to environmental factors whose effects are accumulated. Unfortunately, age differences in BD have been reported in few studies and then for a small numbers of cases [11–13]. Thus, it is uncertain what causes phenotypical differences that depend on age of onset among BD patients. An evaluation of age differences in the manifestation BD using a reliable database has been awaited. In this study, we evaluated the prevalence of BD-related clinical manifestations with emphasis on onset age and sex difference using a Japanese nationwide registration database.
Methods
Overview
This ongoing nationwide registration project has been carried out by the Behçet’s Disease Research Committee, of the Japanese Ministry of Health, Labour and Welfare. The questionnaire format was adopted from 2003 to 2014. A physician who diagnoses a patient with BD registers the patient’s data by filling in a questionnaire, because the registration is mandatory for the BD patient to access free medical resources in Japan. This incentive leads to high compliance with the registration. Institutional review board approval and informed consent were waived because the current analysis used only data after un-linkable anonymization.
The questionnaire requires demography and background patient characteristics such as date of birth, sex, date of BD onset and place of residence. A physician selects Yes, No or Unclear for each BD manifestation [14]. This registration has two independent databases. The newly diagnosed cases are registered in detailed form followed by annual renewal in a simple form. In this study, we analysed only the database of newly diagnosed cases [14].
The Ministry provides a dataset for eligible researchers after un-linkable anonymization. For the current analysis, we utilized the database from 2003 to 2014. Our analysis followed the Ethical Guidelines for Medical and Health Research Involving Human Subjects published in 2015 by the Japanese Ministry of Health, Labour and Welfare [15].
Diagnostic and inclusion criteria
Among the cases in the database, we selected patients who satisfied International Criteria for BD (ICBD) for the main analyses. These criteria require four or more points after adding two points for each of ocular lesions, genital aphthosis and oral aphtosis, and one point for each of skin lesions, neurological manifestations, vascular manifestations and a positive pathergy test [16]. In addition, we picked up patients who satisfied the International Study Group (ISG) criteria, which require an oral ulcer plus two or more of the following: genital ulceration, eye lesion, skin lesion and a positive pathergy test [2]. Patients satisfying the ISG criteria were used only for sensitivity analyses. Our inclusion criteria did not require or exclude any specific treatment for BD.
Specific description of each manifestation
Each manifestation was judged and registered by an attending physician who had diagnosed a BD patient [14]. The physician was usually a rheumatologist supported by medical doctors with other specialties. However, a general physician, an ophthalmologist, a gastroenterologist, a dermatologist or a neurologist could register the patient data.
Oral ulceration is characterized by recurrent aphthous ulcers on the oral mucosa. Skin lesions consists of erythema nodosum-like eruptions, superficial thrombophlebitis and pseudofolliculitis or acne-like eruptions. A typical ocular lesion is bilateral iridocyclitis and/or retinochoroiditis with episodic attack of conjunctival congestion, ophthalmalgia, decreased visual acuity and visual field deficit. Subsequent lesions caused by the uveitis are also taken into account for ocular symptoms: posterior synechia of the iris, crystalline lens pigmentation, chorioretinal atrophy, optic nerve atrophy, co-morbid cataract, subsequent glaucoma and phthisis of the eyeball. A genital ulcer is typically a well-defined painful aphthous ulcer on the scrotum and penis of a male and the labia major and labia minor of a female. A more detailed description of each manifestation is available elsewhere [14].
Statistics
Preceding the analysis, the following cases were eliminated: duplicate registration, birth place outside of Japan, lack of age of diagnosis, lack of age of onset and diagnosis year before birth year. Our analysis focused on the prevalence of each manifestation. Prevalence was estimated from the number of patients with symptoms divided by the number of evaluated patients. Briefly, prevalence was judged from Yes/(Yes + No) ignoring Unclear. The prevalence of two groups was compared by odds ratio (OR). The age of patients with and without each manifestation was compared by a Mann–Whitney test. Prevalence was also estimated for subgroups simultaneously stratified by 10-year increment and sex.
Results
Flow chart for patient screening
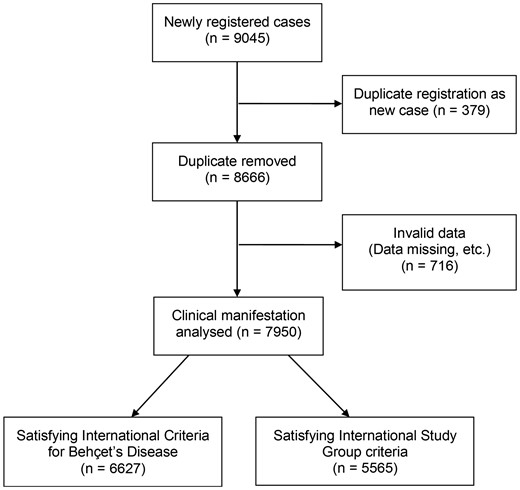
The database for newly diagnosed cases provided data for 9045 individual cases. After eliminating 379 duplicate registrations and 716 invalid cases, 7950 cases were analysable (Fig. 1). Among the 7950 analysable cases, 6627 and 5565 satisfied ICBD criteria and ISG criteria, respectively (Table 1).
Demographic and clinical profiles of the patients
| All | ICBD | ISG criteria | ||
|---|---|---|---|---|
| n | 7950 | 6627 | 5565 | |
| Age, median (IQR), years | 40 (31–52) | 39 (31–50) | 38 (30–48) | |
| Age, years | ||||
| <9 | 342 (5.3) | 293 (4.4) | 231 (4.2) | |
| 20–29 | 1345 (20.7) | 1200 (18.1) | 1065 (19.1) | |
| 30–39 | 2267 (34.8) | 1972 (29.8) | 1719 (30.9) | |
| 40–49 | 1754 (26.9) | 1495 (22.6) | 1250 (22.5) | |
| 50–59 | 1086 (16.7) | 851 (12.8) | 685 (12.3) | |
| 60–69 | 723 (11.1) | 522 (7.9) | 404 (7.3) | |
| >70 | 433 (6.7) | 294 (4.4) | 211 (3.8) | |
| Sex | ||||
| Men | 3379 (42.5) | 2651 (40.0) | 2138 (38.4) | |
| Women | 4571 (57.5) | 3976 (60.0) | 3427 (61.6) | |
| Age of onset, median (IQR), years | 35.5 (27–46) | 35 (27–44) | 35 (27–43) | |
| Registration year | ||||
| 2003–06 | 2296 (28.9) | 1961 (29.6) | 1653 (29.7) | |
| 2007–10 | 3083 (38.8) | 2549 (38.5) | 2123 (38.1) | |
| 2011–14 | 2571 (32.3) | 2117 (31.9) | 1789 (32.1) | |
| Oral ulceration | ||||
| Yes | 7250 (91.2) | 6500 (98.1) | 5565 (100.0) | |
| No | 488 (6.1) | 89 (1.3) | 0 (0.0) | |
| Unclear | 212 (2.7) | 38 (0.6) | 0 (0.0) | |
| Prevalence, % | 93.7 | 98.6 | 100.0 | |
| Skin lesion | ||||
| Yes | 6289 (79.1) | 5674 (85.6) | 5299 (95.2) | |
| No | 1418 (17.8) | 856 (12.9) | 232 (4.2) | |
| Unclear | 243 (3.1) | 97 (1.5) | 34 (0.6) | |
| Prevalence, % | 81.6 | 86.9 | 95.8 | |
| Ocular lesion | ||||
| Yes | 2801 (35.2) | 2617 (39.5) | 2199 (39.5) | |
| No | 4717 (59.3) | 3773 (56.9) | 3166 (56.9) | |
| Unclear | 432 (5.4) | 237 (3.6) | 200 (3.6) | |
| Prevalence, % | 37.3 | 41.0 | 41.0 | |
| Genital ulceration | ||||
| Yes | 4752 (59.8) | 4716 (71.2) | 4308 (77.4) | |
| No | 2780 (35.0) | 1706 (25.7) | 1130 (20.3) | |
| Unclear | 418 (5.3) | 205 (3.1) | 127 (2.3) | |
| Prevalence, % | 63.1 | 73.4 | 79.2 | |
| Positive pathergy test | ||||
| Yes | 1568 (19.7) | 1540 (23.2) | 1492 (26.8) | |
| No | 3204 (40.3) | 2641 (39.9) | 2086 (37.5) | |
| Unclear | 3178 (40.0) | 2446 (36.9) | 1987 (35.7) | |
| Prevalence, % | 32.9 | 36.8 | 41.7 | |
| Arthritis | ||||
| Yes | 3717 (46.8) | 3294 (49.7) | 2858 (51.4) | |
| No | 3728 (46.9) | 3007 (45.4) | 2439 (43.8) | |
| Unclear | 505 (6.4) | 326 (4.9) | 268 (4.8) | |
| Prevalence, % | 49.9 | 52.3 | 54.0 | |
| Epididymitis (male only) | ||||
| Yes | 289 (8.6) | 247 (9.3) | 213 (9.8) | |
| No | 2743 (81.2) | 2150 (81.1) | 1714 (78.5) | |
| Unclear | 347 (10.3) | 254 (9.6) | 211 (9.7) | |
| Prevalence, % | 9.5 | 10.3 | 11.1 | |
| Gastrointestinal symptom | ||||
| Yes | 2368 (29.8) | 1785 (26.9) | 1414 (25.4) | |
| No | 5127 (64.5) | 4557 (68.8) | 3914 (70.3) | |
| Unclear | 455 (5.7) | 285 (4.3) | 237 (4.3) | |
| Prevalence, % | 31.6 | 28.1 | 26.5 | |
| Vascular lesion | ||||
| Yes | 746 (9.4) | 683 (10.3) | 480 (8.6) | |
| No | 5797 (72.9) | 4833 (72.9) | 4146 (74.5) | |
| Unclear | 1407 (17.7) | 1111 (16.8) | 939 (16.9) | |
| Prevalence, % | 11.4 | 12.4 | 10.4 | |
| Neurological manifestation | ||||
| Yes | 1688 (21.2) | 1543 (23.3) | 1168 (21.0) | |
| No | 5821 (73.2) | 4820 (72.7) | 4173 (75.0) | |
| Unclear | 441 (5.5) | 264 (4.0) | 224 (4.0) | |
| Prevalence, % | 22.5 | 24.2 | 21.9 | |
| HLA-B51 positive | ||||
| Yes | 1609 (20.2) | 1356 (20.5) | 1119 (20.1) | |
| No | 1970 (24.8) | 1688 (25.5) | 1380 (24.8) | |
| Unclear | 4371 (55.0) | 3583 (54.1) | 3066 (55.1) | |
| Prevalence, % | 45.0 | 44.5 | 44.8 | |
| All | ICBD | ISG criteria | ||
|---|---|---|---|---|
| n | 7950 | 6627 | 5565 | |
| Age, median (IQR), years | 40 (31–52) | 39 (31–50) | 38 (30–48) | |
| Age, years | ||||
| <9 | 342 (5.3) | 293 (4.4) | 231 (4.2) | |
| 20–29 | 1345 (20.7) | 1200 (18.1) | 1065 (19.1) | |
| 30–39 | 2267 (34.8) | 1972 (29.8) | 1719 (30.9) | |
| 40–49 | 1754 (26.9) | 1495 (22.6) | 1250 (22.5) | |
| 50–59 | 1086 (16.7) | 851 (12.8) | 685 (12.3) | |
| 60–69 | 723 (11.1) | 522 (7.9) | 404 (7.3) | |
| >70 | 433 (6.7) | 294 (4.4) | 211 (3.8) | |
| Sex | ||||
| Men | 3379 (42.5) | 2651 (40.0) | 2138 (38.4) | |
| Women | 4571 (57.5) | 3976 (60.0) | 3427 (61.6) | |
| Age of onset, median (IQR), years | 35.5 (27–46) | 35 (27–44) | 35 (27–43) | |
| Registration year | ||||
| 2003–06 | 2296 (28.9) | 1961 (29.6) | 1653 (29.7) | |
| 2007–10 | 3083 (38.8) | 2549 (38.5) | 2123 (38.1) | |
| 2011–14 | 2571 (32.3) | 2117 (31.9) | 1789 (32.1) | |
| Oral ulceration | ||||
| Yes | 7250 (91.2) | 6500 (98.1) | 5565 (100.0) | |
| No | 488 (6.1) | 89 (1.3) | 0 (0.0) | |
| Unclear | 212 (2.7) | 38 (0.6) | 0 (0.0) | |
| Prevalence, % | 93.7 | 98.6 | 100.0 | |
| Skin lesion | ||||
| Yes | 6289 (79.1) | 5674 (85.6) | 5299 (95.2) | |
| No | 1418 (17.8) | 856 (12.9) | 232 (4.2) | |
| Unclear | 243 (3.1) | 97 (1.5) | 34 (0.6) | |
| Prevalence, % | 81.6 | 86.9 | 95.8 | |
| Ocular lesion | ||||
| Yes | 2801 (35.2) | 2617 (39.5) | 2199 (39.5) | |
| No | 4717 (59.3) | 3773 (56.9) | 3166 (56.9) | |
| Unclear | 432 (5.4) | 237 (3.6) | 200 (3.6) | |
| Prevalence, % | 37.3 | 41.0 | 41.0 | |
| Genital ulceration | ||||
| Yes | 4752 (59.8) | 4716 (71.2) | 4308 (77.4) | |
| No | 2780 (35.0) | 1706 (25.7) | 1130 (20.3) | |
| Unclear | 418 (5.3) | 205 (3.1) | 127 (2.3) | |
| Prevalence, % | 63.1 | 73.4 | 79.2 | |
| Positive pathergy test | ||||
| Yes | 1568 (19.7) | 1540 (23.2) | 1492 (26.8) | |
| No | 3204 (40.3) | 2641 (39.9) | 2086 (37.5) | |
| Unclear | 3178 (40.0) | 2446 (36.9) | 1987 (35.7) | |
| Prevalence, % | 32.9 | 36.8 | 41.7 | |
| Arthritis | ||||
| Yes | 3717 (46.8) | 3294 (49.7) | 2858 (51.4) | |
| No | 3728 (46.9) | 3007 (45.4) | 2439 (43.8) | |
| Unclear | 505 (6.4) | 326 (4.9) | 268 (4.8) | |
| Prevalence, % | 49.9 | 52.3 | 54.0 | |
| Epididymitis (male only) | ||||
| Yes | 289 (8.6) | 247 (9.3) | 213 (9.8) | |
| No | 2743 (81.2) | 2150 (81.1) | 1714 (78.5) | |
| Unclear | 347 (10.3) | 254 (9.6) | 211 (9.7) | |
| Prevalence, % | 9.5 | 10.3 | 11.1 | |
| Gastrointestinal symptom | ||||
| Yes | 2368 (29.8) | 1785 (26.9) | 1414 (25.4) | |
| No | 5127 (64.5) | 4557 (68.8) | 3914 (70.3) | |
| Unclear | 455 (5.7) | 285 (4.3) | 237 (4.3) | |
| Prevalence, % | 31.6 | 28.1 | 26.5 | |
| Vascular lesion | ||||
| Yes | 746 (9.4) | 683 (10.3) | 480 (8.6) | |
| No | 5797 (72.9) | 4833 (72.9) | 4146 (74.5) | |
| Unclear | 1407 (17.7) | 1111 (16.8) | 939 (16.9) | |
| Prevalence, % | 11.4 | 12.4 | 10.4 | |
| Neurological manifestation | ||||
| Yes | 1688 (21.2) | 1543 (23.3) | 1168 (21.0) | |
| No | 5821 (73.2) | 4820 (72.7) | 4173 (75.0) | |
| Unclear | 441 (5.5) | 264 (4.0) | 224 (4.0) | |
| Prevalence, % | 22.5 | 24.2 | 21.9 | |
| HLA-B51 positive | ||||
| Yes | 1609 (20.2) | 1356 (20.5) | 1119 (20.1) | |
| No | 1970 (24.8) | 1688 (25.5) | 1380 (24.8) | |
| Unclear | 4371 (55.0) | 3583 (54.1) | 3066 (55.1) | |
| Prevalence, % | 45.0 | 44.5 | 44.8 | |
Values presented as n (%) unless otherwise stated. Prevalence was judged from Yes/(Yes + No) ignoring Unclear. ICBD: International Criteria for Behçet’s Disease; ISG: International Study Group for Behçet’s disease.
Demographic and clinical profiles of the patients
| All | ICBD | ISG criteria | ||
|---|---|---|---|---|
| n | 7950 | 6627 | 5565 | |
| Age, median (IQR), years | 40 (31–52) | 39 (31–50) | 38 (30–48) | |
| Age, years | ||||
| <9 | 342 (5.3) | 293 (4.4) | 231 (4.2) | |
| 20–29 | 1345 (20.7) | 1200 (18.1) | 1065 (19.1) | |
| 30–39 | 2267 (34.8) | 1972 (29.8) | 1719 (30.9) | |
| 40–49 | 1754 (26.9) | 1495 (22.6) | 1250 (22.5) | |
| 50–59 | 1086 (16.7) | 851 (12.8) | 685 (12.3) | |
| 60–69 | 723 (11.1) | 522 (7.9) | 404 (7.3) | |
| >70 | 433 (6.7) | 294 (4.4) | 211 (3.8) | |
| Sex | ||||
| Men | 3379 (42.5) | 2651 (40.0) | 2138 (38.4) | |
| Women | 4571 (57.5) | 3976 (60.0) | 3427 (61.6) | |
| Age of onset, median (IQR), years | 35.5 (27–46) | 35 (27–44) | 35 (27–43) | |
| Registration year | ||||
| 2003–06 | 2296 (28.9) | 1961 (29.6) | 1653 (29.7) | |
| 2007–10 | 3083 (38.8) | 2549 (38.5) | 2123 (38.1) | |
| 2011–14 | 2571 (32.3) | 2117 (31.9) | 1789 (32.1) | |
| Oral ulceration | ||||
| Yes | 7250 (91.2) | 6500 (98.1) | 5565 (100.0) | |
| No | 488 (6.1) | 89 (1.3) | 0 (0.0) | |
| Unclear | 212 (2.7) | 38 (0.6) | 0 (0.0) | |
| Prevalence, % | 93.7 | 98.6 | 100.0 | |
| Skin lesion | ||||
| Yes | 6289 (79.1) | 5674 (85.6) | 5299 (95.2) | |
| No | 1418 (17.8) | 856 (12.9) | 232 (4.2) | |
| Unclear | 243 (3.1) | 97 (1.5) | 34 (0.6) | |
| Prevalence, % | 81.6 | 86.9 | 95.8 | |
| Ocular lesion | ||||
| Yes | 2801 (35.2) | 2617 (39.5) | 2199 (39.5) | |
| No | 4717 (59.3) | 3773 (56.9) | 3166 (56.9) | |
| Unclear | 432 (5.4) | 237 (3.6) | 200 (3.6) | |
| Prevalence, % | 37.3 | 41.0 | 41.0 | |
| Genital ulceration | ||||
| Yes | 4752 (59.8) | 4716 (71.2) | 4308 (77.4) | |
| No | 2780 (35.0) | 1706 (25.7) | 1130 (20.3) | |
| Unclear | 418 (5.3) | 205 (3.1) | 127 (2.3) | |
| Prevalence, % | 63.1 | 73.4 | 79.2 | |
| Positive pathergy test | ||||
| Yes | 1568 (19.7) | 1540 (23.2) | 1492 (26.8) | |
| No | 3204 (40.3) | 2641 (39.9) | 2086 (37.5) | |
| Unclear | 3178 (40.0) | 2446 (36.9) | 1987 (35.7) | |
| Prevalence, % | 32.9 | 36.8 | 41.7 | |
| Arthritis | ||||
| Yes | 3717 (46.8) | 3294 (49.7) | 2858 (51.4) | |
| No | 3728 (46.9) | 3007 (45.4) | 2439 (43.8) | |
| Unclear | 505 (6.4) | 326 (4.9) | 268 (4.8) | |
| Prevalence, % | 49.9 | 52.3 | 54.0 | |
| Epididymitis (male only) | ||||
| Yes | 289 (8.6) | 247 (9.3) | 213 (9.8) | |
| No | 2743 (81.2) | 2150 (81.1) | 1714 (78.5) | |
| Unclear | 347 (10.3) | 254 (9.6) | 211 (9.7) | |
| Prevalence, % | 9.5 | 10.3 | 11.1 | |
| Gastrointestinal symptom | ||||
| Yes | 2368 (29.8) | 1785 (26.9) | 1414 (25.4) | |
| No | 5127 (64.5) | 4557 (68.8) | 3914 (70.3) | |
| Unclear | 455 (5.7) | 285 (4.3) | 237 (4.3) | |
| Prevalence, % | 31.6 | 28.1 | 26.5 | |
| Vascular lesion | ||||
| Yes | 746 (9.4) | 683 (10.3) | 480 (8.6) | |
| No | 5797 (72.9) | 4833 (72.9) | 4146 (74.5) | |
| Unclear | 1407 (17.7) | 1111 (16.8) | 939 (16.9) | |
| Prevalence, % | 11.4 | 12.4 | 10.4 | |
| Neurological manifestation | ||||
| Yes | 1688 (21.2) | 1543 (23.3) | 1168 (21.0) | |
| No | 5821 (73.2) | 4820 (72.7) | 4173 (75.0) | |
| Unclear | 441 (5.5) | 264 (4.0) | 224 (4.0) | |
| Prevalence, % | 22.5 | 24.2 | 21.9 | |
| HLA-B51 positive | ||||
| Yes | 1609 (20.2) | 1356 (20.5) | 1119 (20.1) | |
| No | 1970 (24.8) | 1688 (25.5) | 1380 (24.8) | |
| Unclear | 4371 (55.0) | 3583 (54.1) | 3066 (55.1) | |
| Prevalence, % | 45.0 | 44.5 | 44.8 | |
| All | ICBD | ISG criteria | ||
|---|---|---|---|---|
| n | 7950 | 6627 | 5565 | |
| Age, median (IQR), years | 40 (31–52) | 39 (31–50) | 38 (30–48) | |
| Age, years | ||||
| <9 | 342 (5.3) | 293 (4.4) | 231 (4.2) | |
| 20–29 | 1345 (20.7) | 1200 (18.1) | 1065 (19.1) | |
| 30–39 | 2267 (34.8) | 1972 (29.8) | 1719 (30.9) | |
| 40–49 | 1754 (26.9) | 1495 (22.6) | 1250 (22.5) | |
| 50–59 | 1086 (16.7) | 851 (12.8) | 685 (12.3) | |
| 60–69 | 723 (11.1) | 522 (7.9) | 404 (7.3) | |
| >70 | 433 (6.7) | 294 (4.4) | 211 (3.8) | |
| Sex | ||||
| Men | 3379 (42.5) | 2651 (40.0) | 2138 (38.4) | |
| Women | 4571 (57.5) | 3976 (60.0) | 3427 (61.6) | |
| Age of onset, median (IQR), years | 35.5 (27–46) | 35 (27–44) | 35 (27–43) | |
| Registration year | ||||
| 2003–06 | 2296 (28.9) | 1961 (29.6) | 1653 (29.7) | |
| 2007–10 | 3083 (38.8) | 2549 (38.5) | 2123 (38.1) | |
| 2011–14 | 2571 (32.3) | 2117 (31.9) | 1789 (32.1) | |
| Oral ulceration | ||||
| Yes | 7250 (91.2) | 6500 (98.1) | 5565 (100.0) | |
| No | 488 (6.1) | 89 (1.3) | 0 (0.0) | |
| Unclear | 212 (2.7) | 38 (0.6) | 0 (0.0) | |
| Prevalence, % | 93.7 | 98.6 | 100.0 | |
| Skin lesion | ||||
| Yes | 6289 (79.1) | 5674 (85.6) | 5299 (95.2) | |
| No | 1418 (17.8) | 856 (12.9) | 232 (4.2) | |
| Unclear | 243 (3.1) | 97 (1.5) | 34 (0.6) | |
| Prevalence, % | 81.6 | 86.9 | 95.8 | |
| Ocular lesion | ||||
| Yes | 2801 (35.2) | 2617 (39.5) | 2199 (39.5) | |
| No | 4717 (59.3) | 3773 (56.9) | 3166 (56.9) | |
| Unclear | 432 (5.4) | 237 (3.6) | 200 (3.6) | |
| Prevalence, % | 37.3 | 41.0 | 41.0 | |
| Genital ulceration | ||||
| Yes | 4752 (59.8) | 4716 (71.2) | 4308 (77.4) | |
| No | 2780 (35.0) | 1706 (25.7) | 1130 (20.3) | |
| Unclear | 418 (5.3) | 205 (3.1) | 127 (2.3) | |
| Prevalence, % | 63.1 | 73.4 | 79.2 | |
| Positive pathergy test | ||||
| Yes | 1568 (19.7) | 1540 (23.2) | 1492 (26.8) | |
| No | 3204 (40.3) | 2641 (39.9) | 2086 (37.5) | |
| Unclear | 3178 (40.0) | 2446 (36.9) | 1987 (35.7) | |
| Prevalence, % | 32.9 | 36.8 | 41.7 | |
| Arthritis | ||||
| Yes | 3717 (46.8) | 3294 (49.7) | 2858 (51.4) | |
| No | 3728 (46.9) | 3007 (45.4) | 2439 (43.8) | |
| Unclear | 505 (6.4) | 326 (4.9) | 268 (4.8) | |
| Prevalence, % | 49.9 | 52.3 | 54.0 | |
| Epididymitis (male only) | ||||
| Yes | 289 (8.6) | 247 (9.3) | 213 (9.8) | |
| No | 2743 (81.2) | 2150 (81.1) | 1714 (78.5) | |
| Unclear | 347 (10.3) | 254 (9.6) | 211 (9.7) | |
| Prevalence, % | 9.5 | 10.3 | 11.1 | |
| Gastrointestinal symptom | ||||
| Yes | 2368 (29.8) | 1785 (26.9) | 1414 (25.4) | |
| No | 5127 (64.5) | 4557 (68.8) | 3914 (70.3) | |
| Unclear | 455 (5.7) | 285 (4.3) | 237 (4.3) | |
| Prevalence, % | 31.6 | 28.1 | 26.5 | |
| Vascular lesion | ||||
| Yes | 746 (9.4) | 683 (10.3) | 480 (8.6) | |
| No | 5797 (72.9) | 4833 (72.9) | 4146 (74.5) | |
| Unclear | 1407 (17.7) | 1111 (16.8) | 939 (16.9) | |
| Prevalence, % | 11.4 | 12.4 | 10.4 | |
| Neurological manifestation | ||||
| Yes | 1688 (21.2) | 1543 (23.3) | 1168 (21.0) | |
| No | 5821 (73.2) | 4820 (72.7) | 4173 (75.0) | |
| Unclear | 441 (5.5) | 264 (4.0) | 224 (4.0) | |
| Prevalence, % | 22.5 | 24.2 | 21.9 | |
| HLA-B51 positive | ||||
| Yes | 1609 (20.2) | 1356 (20.5) | 1119 (20.1) | |
| No | 1970 (24.8) | 1688 (25.5) | 1380 (24.8) | |
| Unclear | 4371 (55.0) | 3583 (54.1) | 3066 (55.1) | |
| Prevalence, % | 45.0 | 44.5 | 44.8 | |
Values presented as n (%) unless otherwise stated. Prevalence was judged from Yes/(Yes + No) ignoring Unclear. ICBD: International Criteria for Behçet’s Disease; ISG: International Study Group for Behçet’s disease.
Flow chart of patients
Background characteristics of ICBD patients
Patients were registered from all prefectures of Japan: 1.8% from Hokkaido, 84.9% from Honshu, 4.5% from Shikoku and 8.9% from Kyushu. Among the 6627 BD patients who satisfied the ICBD, 2651 (40.0%) were men and 3976 (60.0%) were women with a median age of 39 years [interquartile range (IQR) 31–50 years, range 0–106 years]. The median age of onset was 35 years (IQR: 27–44 years) and the median duration between the onset and registration was 1 year (IQR: 0–4 years). Three hundred and twenty-eight patients (4.9%) had a family history of BD (Table 1).
We analysed data of Yes or No after excluding Unclear in individual symptomatic items. Data for each manifestation were obtained for >80% of cases except pathergy test and HLA-B51, which were unclear in 36.9 and 54.1% of patients who satisfied the ICBD, respectively. The prevalence for each manifestation greatly varied. For example, while skin lesion was observed for 86.9% of cases, the prevalence of epididymitis and vascular lesion were 10.3 and 12.4%, respectively (Table 1).
Sex difference
We observed significant sex difference of all manifestations except for neurological manifestations and gastrointestinal symptoms. The difference was prominent for ocular lesions, genital ulceration and oral ulceration (Table 2).
Sex differences of patients who satisfied International Criteria for Behçet’s Disease criteria (n = 6627)
| Men | Women | Comparison, OR (95% CI), P-value | |
|---|---|---|---|
| n | 2651 | 3976 | |
| Oral ulceration | |||
| Yes | 2586 (97.5) | 3914 (98.4) | 0.49 (0.32, 0.75), 0.001 |
| No | 51 (1.9) | 38 (1) | |
| Unclear | 14 (0.5) | 24 (0.6) | |
| Prevalence, % | 98.1 | 99.0 | |
| Skin lesions | |||
| Yes | 2226 (84) | 3448 (86.7) | 0.82 (0.71, 0.94), 0.006 |
| No | 378 (14.3) | 478 (12) | |
| Unclear | 47 (1.8) | 50 (1.3) | |
| Prevalence, % | 85.5 | 87.8 | |
| Ocular lesions | |||
| Yes | 1401 (52.8) | 1216 (30.6) | 2.58 (2.33, 2.86), 0.001 |
| No | 1165 (43.9) | 2608 (65.6) | |
| Unclear | 85 (3.2) | 152 (3.8) | |
| Prevalence, % | 54.6 | 31.8 | |
| Genital ulceration | |||
| Yes | 1491 (56.2) | 3225 (81.1) | 0.29 (0.25, 0.32), 0.001 |
| No | 1055 (39.8) | 651 (16.4) | |
| Unclear | 105 (4) | 100 (2.5) | |
| Prevalence, % | 58.6 | 83.2 | |
| Positive pathergy test | |||
| Yes | 645 (24.3) | 895 (22.5) | 1.2 (1.05, 1.36), 0.006 |
| No | 993 (37.5) | 1648 (41.4) | |
| Unclear | 1013 (38.2) | 1433 (36) | |
| Prevalence | 39.4 | 35.2 | |
| Arthritis | |||
| Yes | 1152 (43.5) | 2142 (53.9) | 0.67 (0.61, 0.74), <0.001 |
| No | 1338 (50.5) | 1669 (42) | |
| Unclear | 161 (6.1) | 165 (4.1) | |
| Prevalence, % | 46.3 | 56.2 | |
| Gastrointestinal symptoms | |||
| Yes | 679 (25.6) | 1106 (27.8) | 0.91 (0.81, 1.02), 0.090 |
| No | 1839 (69.4) | 2718 (68.4) | |
| Unclear | 133 (5) | 152 (3.8) | |
| Prevalence, % | 27.0 | 28.9 | |
| Vascular lesions | |||
| Yes | 339 (12.8) | 344 (8.7) | OR 1.55 (1.32. 1.82), <0.001 |
| No | 1879 (70.9) | 2954 (74.3) | |
| Unclear | 433 (16.3) | 678 (17.1) | |
| Prevalence, % | 15.3 | 10.4 | |
| Neurological manifestations | |||
| Yes | 585 (22.1) | 958 (24.1) | 0.91 (0.81, 1.02), 0.100 |
| No | 1941 (73.2) | 2879 (72.4) | |
| Unclear | 125 (4.7) | 139 (3.5) | |
| Prevalence, % | 23.2 | 25.0 | |
| HLA-B51 positive | |||
| Yes | 645 (24.3) | 711 (17.9) | 1.32 (1.14, 1.52), <0.001 |
| No | 689 (26) | 999 (25.1) | |
| Unclear | 1317 (49.7) | 2266 (57) | |
| Prevalence, % | 48.4 | 41.6 |
| Men | Women | Comparison, OR (95% CI), P-value | |
|---|---|---|---|
| n | 2651 | 3976 | |
| Oral ulceration | |||
| Yes | 2586 (97.5) | 3914 (98.4) | 0.49 (0.32, 0.75), 0.001 |
| No | 51 (1.9) | 38 (1) | |
| Unclear | 14 (0.5) | 24 (0.6) | |
| Prevalence, % | 98.1 | 99.0 | |
| Skin lesions | |||
| Yes | 2226 (84) | 3448 (86.7) | 0.82 (0.71, 0.94), 0.006 |
| No | 378 (14.3) | 478 (12) | |
| Unclear | 47 (1.8) | 50 (1.3) | |
| Prevalence, % | 85.5 | 87.8 | |
| Ocular lesions | |||
| Yes | 1401 (52.8) | 1216 (30.6) | 2.58 (2.33, 2.86), 0.001 |
| No | 1165 (43.9) | 2608 (65.6) | |
| Unclear | 85 (3.2) | 152 (3.8) | |
| Prevalence, % | 54.6 | 31.8 | |
| Genital ulceration | |||
| Yes | 1491 (56.2) | 3225 (81.1) | 0.29 (0.25, 0.32), 0.001 |
| No | 1055 (39.8) | 651 (16.4) | |
| Unclear | 105 (4) | 100 (2.5) | |
| Prevalence, % | 58.6 | 83.2 | |
| Positive pathergy test | |||
| Yes | 645 (24.3) | 895 (22.5) | 1.2 (1.05, 1.36), 0.006 |
| No | 993 (37.5) | 1648 (41.4) | |
| Unclear | 1013 (38.2) | 1433 (36) | |
| Prevalence | 39.4 | 35.2 | |
| Arthritis | |||
| Yes | 1152 (43.5) | 2142 (53.9) | 0.67 (0.61, 0.74), <0.001 |
| No | 1338 (50.5) | 1669 (42) | |
| Unclear | 161 (6.1) | 165 (4.1) | |
| Prevalence, % | 46.3 | 56.2 | |
| Gastrointestinal symptoms | |||
| Yes | 679 (25.6) | 1106 (27.8) | 0.91 (0.81, 1.02), 0.090 |
| No | 1839 (69.4) | 2718 (68.4) | |
| Unclear | 133 (5) | 152 (3.8) | |
| Prevalence, % | 27.0 | 28.9 | |
| Vascular lesions | |||
| Yes | 339 (12.8) | 344 (8.7) | OR 1.55 (1.32. 1.82), <0.001 |
| No | 1879 (70.9) | 2954 (74.3) | |
| Unclear | 433 (16.3) | 678 (17.1) | |
| Prevalence, % | 15.3 | 10.4 | |
| Neurological manifestations | |||
| Yes | 585 (22.1) | 958 (24.1) | 0.91 (0.81, 1.02), 0.100 |
| No | 1941 (73.2) | 2879 (72.4) | |
| Unclear | 125 (4.7) | 139 (3.5) | |
| Prevalence, % | 23.2 | 25.0 | |
| HLA-B51 positive | |||
| Yes | 645 (24.3) | 711 (17.9) | 1.32 (1.14, 1.52), <0.001 |
| No | 689 (26) | 999 (25.1) | |
| Unclear | 1317 (49.7) | 2266 (57) | |
| Prevalence, % | 48.4 | 41.6 |
Values listed as n (%) unless otherwise stated. Prevalence was judged from Yes/(Yes + No) ignoring Unclear. Epididymitis was excluded from this table. OR: odds ratio evaluating females as reference.
Sex differences of patients who satisfied International Criteria for Behçet’s Disease criteria (n = 6627)
| Men | Women | Comparison, OR (95% CI), P-value | |
|---|---|---|---|
| n | 2651 | 3976 | |
| Oral ulceration | |||
| Yes | 2586 (97.5) | 3914 (98.4) | 0.49 (0.32, 0.75), 0.001 |
| No | 51 (1.9) | 38 (1) | |
| Unclear | 14 (0.5) | 24 (0.6) | |
| Prevalence, % | 98.1 | 99.0 | |
| Skin lesions | |||
| Yes | 2226 (84) | 3448 (86.7) | 0.82 (0.71, 0.94), 0.006 |
| No | 378 (14.3) | 478 (12) | |
| Unclear | 47 (1.8) | 50 (1.3) | |
| Prevalence, % | 85.5 | 87.8 | |
| Ocular lesions | |||
| Yes | 1401 (52.8) | 1216 (30.6) | 2.58 (2.33, 2.86), 0.001 |
| No | 1165 (43.9) | 2608 (65.6) | |
| Unclear | 85 (3.2) | 152 (3.8) | |
| Prevalence, % | 54.6 | 31.8 | |
| Genital ulceration | |||
| Yes | 1491 (56.2) | 3225 (81.1) | 0.29 (0.25, 0.32), 0.001 |
| No | 1055 (39.8) | 651 (16.4) | |
| Unclear | 105 (4) | 100 (2.5) | |
| Prevalence, % | 58.6 | 83.2 | |
| Positive pathergy test | |||
| Yes | 645 (24.3) | 895 (22.5) | 1.2 (1.05, 1.36), 0.006 |
| No | 993 (37.5) | 1648 (41.4) | |
| Unclear | 1013 (38.2) | 1433 (36) | |
| Prevalence | 39.4 | 35.2 | |
| Arthritis | |||
| Yes | 1152 (43.5) | 2142 (53.9) | 0.67 (0.61, 0.74), <0.001 |
| No | 1338 (50.5) | 1669 (42) | |
| Unclear | 161 (6.1) | 165 (4.1) | |
| Prevalence, % | 46.3 | 56.2 | |
| Gastrointestinal symptoms | |||
| Yes | 679 (25.6) | 1106 (27.8) | 0.91 (0.81, 1.02), 0.090 |
| No | 1839 (69.4) | 2718 (68.4) | |
| Unclear | 133 (5) | 152 (3.8) | |
| Prevalence, % | 27.0 | 28.9 | |
| Vascular lesions | |||
| Yes | 339 (12.8) | 344 (8.7) | OR 1.55 (1.32. 1.82), <0.001 |
| No | 1879 (70.9) | 2954 (74.3) | |
| Unclear | 433 (16.3) | 678 (17.1) | |
| Prevalence, % | 15.3 | 10.4 | |
| Neurological manifestations | |||
| Yes | 585 (22.1) | 958 (24.1) | 0.91 (0.81, 1.02), 0.100 |
| No | 1941 (73.2) | 2879 (72.4) | |
| Unclear | 125 (4.7) | 139 (3.5) | |
| Prevalence, % | 23.2 | 25.0 | |
| HLA-B51 positive | |||
| Yes | 645 (24.3) | 711 (17.9) | 1.32 (1.14, 1.52), <0.001 |
| No | 689 (26) | 999 (25.1) | |
| Unclear | 1317 (49.7) | 2266 (57) | |
| Prevalence, % | 48.4 | 41.6 |
| Men | Women | Comparison, OR (95% CI), P-value | |
|---|---|---|---|
| n | 2651 | 3976 | |
| Oral ulceration | |||
| Yes | 2586 (97.5) | 3914 (98.4) | 0.49 (0.32, 0.75), 0.001 |
| No | 51 (1.9) | 38 (1) | |
| Unclear | 14 (0.5) | 24 (0.6) | |
| Prevalence, % | 98.1 | 99.0 | |
| Skin lesions | |||
| Yes | 2226 (84) | 3448 (86.7) | 0.82 (0.71, 0.94), 0.006 |
| No | 378 (14.3) | 478 (12) | |
| Unclear | 47 (1.8) | 50 (1.3) | |
| Prevalence, % | 85.5 | 87.8 | |
| Ocular lesions | |||
| Yes | 1401 (52.8) | 1216 (30.6) | 2.58 (2.33, 2.86), 0.001 |
| No | 1165 (43.9) | 2608 (65.6) | |
| Unclear | 85 (3.2) | 152 (3.8) | |
| Prevalence, % | 54.6 | 31.8 | |
| Genital ulceration | |||
| Yes | 1491 (56.2) | 3225 (81.1) | 0.29 (0.25, 0.32), 0.001 |
| No | 1055 (39.8) | 651 (16.4) | |
| Unclear | 105 (4) | 100 (2.5) | |
| Prevalence, % | 58.6 | 83.2 | |
| Positive pathergy test | |||
| Yes | 645 (24.3) | 895 (22.5) | 1.2 (1.05, 1.36), 0.006 |
| No | 993 (37.5) | 1648 (41.4) | |
| Unclear | 1013 (38.2) | 1433 (36) | |
| Prevalence | 39.4 | 35.2 | |
| Arthritis | |||
| Yes | 1152 (43.5) | 2142 (53.9) | 0.67 (0.61, 0.74), <0.001 |
| No | 1338 (50.5) | 1669 (42) | |
| Unclear | 161 (6.1) | 165 (4.1) | |
| Prevalence, % | 46.3 | 56.2 | |
| Gastrointestinal symptoms | |||
| Yes | 679 (25.6) | 1106 (27.8) | 0.91 (0.81, 1.02), 0.090 |
| No | 1839 (69.4) | 2718 (68.4) | |
| Unclear | 133 (5) | 152 (3.8) | |
| Prevalence, % | 27.0 | 28.9 | |
| Vascular lesions | |||
| Yes | 339 (12.8) | 344 (8.7) | OR 1.55 (1.32. 1.82), <0.001 |
| No | 1879 (70.9) | 2954 (74.3) | |
| Unclear | 433 (16.3) | 678 (17.1) | |
| Prevalence, % | 15.3 | 10.4 | |
| Neurological manifestations | |||
| Yes | 585 (22.1) | 958 (24.1) | 0.91 (0.81, 1.02), 0.100 |
| No | 1941 (73.2) | 2879 (72.4) | |
| Unclear | 125 (4.7) | 139 (3.5) | |
| Prevalence, % | 23.2 | 25.0 | |
| HLA-B51 positive | |||
| Yes | 645 (24.3) | 711 (17.9) | 1.32 (1.14, 1.52), <0.001 |
| No | 689 (26) | 999 (25.1) | |
| Unclear | 1317 (49.7) | 2266 (57) | |
| Prevalence, % | 48.4 | 41.6 |
Values listed as n (%) unless otherwise stated. Prevalence was judged from Yes/(Yes + No) ignoring Unclear. Epididymitis was excluded from this table. OR: odds ratio evaluating females as reference.
The prevalence of ocular lesion was 54.6 and 31.8% in men and women, respectively, yielding an OR of 2.58 (95% CI: 2.33, 2.86, P < 0.001). Among the 6627 ICBD cases, 58.6% of men and 83.2% of women had genital ulceration. This led to an OR of 0.29 (95% CI: 0.25, 0.32, P < 0.001). The frequency of oral ulceration was 98.1% for men and 99.0% for women. The oral ulceration showed female predominance with an OR of 0.49 (95% CI: 0.32, 0.75, P < 0.001) (Table 2).
Age difference
We asked whether age of onset affected presence or absence of a particular symptom at registration. Ocular lesion (P < 0.001), arthritis (P < 0.001) vascular lesions (P < 0.001) and neurological manifestations (P = 0.004) were more frequently observed for the elder population, whereas oral ulceration (P = 0.003), skin lesions (P < 0.001) and genital ulceration (P < 0.001) were more common in younger patients (Table 3).
Age differences of patients who satisfied International Criteria for Behçet’s Disease criteria (n = 6627)
| Manifestation (+) | Manifestation (−) | ||||
|---|---|---|---|---|---|
| Manifestation | n | Median age (IQR), years | n | Median age (IQR), years | P-value |
| Oral ulceration | 6500 | 39 (30.75–49.25) | 89 | 44 (33–57) | 0.003 |
| Skin lesions | 5674 | 38 (30–48.75) | 856 | 42 (31.75–55) | <0.001 |
| Ocular lesions | 2617 | 40 (32–52) | 3773 | 38 (29–47) | <0.001 |
| Genital ulceration | 4716 | 38 (30–48) | 1706 | 41 (32–53) | <0.001 |
| Positive pathergy test | 1540 | 38 (30–50) | 2641 | 38 (30–48) | 0.180 |
| Arthritis | 3294 | 39 (31–50) | 3007 | 38 (29–48) | <0.001 |
| Epididymitis (men only) | 247 | 38 (31–46.5) | 2150 | 40 (31–53) | 0.023 |
| Gastrointestinal symptoms | 1785 | 39 (30–52) | 4557 | 38 (31–48) | 0.038 |
| Vascular lesions | 683 | 43 (33–55.5) | 4833 | 38 (30–48) | <0.001 |
| Neurological manifestations | 1543 | 39 (31–51) | 4820 | 38 (30–49) | 0.004 |
| HLA-B51 positive | 1356 | 38 (30–49) | 1688 | 37 (29–46.25) | 0.022 |
| Manifestation (+) | Manifestation (−) | ||||
|---|---|---|---|---|---|
| Manifestation | n | Median age (IQR), years | n | Median age (IQR), years | P-value |
| Oral ulceration | 6500 | 39 (30.75–49.25) | 89 | 44 (33–57) | 0.003 |
| Skin lesions | 5674 | 38 (30–48.75) | 856 | 42 (31.75–55) | <0.001 |
| Ocular lesions | 2617 | 40 (32–52) | 3773 | 38 (29–47) | <0.001 |
| Genital ulceration | 4716 | 38 (30–48) | 1706 | 41 (32–53) | <0.001 |
| Positive pathergy test | 1540 | 38 (30–50) | 2641 | 38 (30–48) | 0.180 |
| Arthritis | 3294 | 39 (31–50) | 3007 | 38 (29–48) | <0.001 |
| Epididymitis (men only) | 247 | 38 (31–46.5) | 2150 | 40 (31–53) | 0.023 |
| Gastrointestinal symptoms | 1785 | 39 (30–52) | 4557 | 38 (31–48) | 0.038 |
| Vascular lesions | 683 | 43 (33–55.5) | 4833 | 38 (30–48) | <0.001 |
| Neurological manifestations | 1543 | 39 (31–51) | 4820 | 38 (30–49) | 0.004 |
| HLA-B51 positive | 1356 | 38 (30–49) | 1688 | 37 (29–46.25) | 0.022 |
P: Mann–Whitney test.
Age differences of patients who satisfied International Criteria for Behçet’s Disease criteria (n = 6627)
| Manifestation (+) | Manifestation (−) | ||||
|---|---|---|---|---|---|
| Manifestation | n | Median age (IQR), years | n | Median age (IQR), years | P-value |
| Oral ulceration | 6500 | 39 (30.75–49.25) | 89 | 44 (33–57) | 0.003 |
| Skin lesions | 5674 | 38 (30–48.75) | 856 | 42 (31.75–55) | <0.001 |
| Ocular lesions | 2617 | 40 (32–52) | 3773 | 38 (29–47) | <0.001 |
| Genital ulceration | 4716 | 38 (30–48) | 1706 | 41 (32–53) | <0.001 |
| Positive pathergy test | 1540 | 38 (30–50) | 2641 | 38 (30–48) | 0.180 |
| Arthritis | 3294 | 39 (31–50) | 3007 | 38 (29–48) | <0.001 |
| Epididymitis (men only) | 247 | 38 (31–46.5) | 2150 | 40 (31–53) | 0.023 |
| Gastrointestinal symptoms | 1785 | 39 (30–52) | 4557 | 38 (31–48) | 0.038 |
| Vascular lesions | 683 | 43 (33–55.5) | 4833 | 38 (30–48) | <0.001 |
| Neurological manifestations | 1543 | 39 (31–51) | 4820 | 38 (30–49) | 0.004 |
| HLA-B51 positive | 1356 | 38 (30–49) | 1688 | 37 (29–46.25) | 0.022 |
| Manifestation (+) | Manifestation (−) | ||||
|---|---|---|---|---|---|
| Manifestation | n | Median age (IQR), years | n | Median age (IQR), years | P-value |
| Oral ulceration | 6500 | 39 (30.75–49.25) | 89 | 44 (33–57) | 0.003 |
| Skin lesions | 5674 | 38 (30–48.75) | 856 | 42 (31.75–55) | <0.001 |
| Ocular lesions | 2617 | 40 (32–52) | 3773 | 38 (29–47) | <0.001 |
| Genital ulceration | 4716 | 38 (30–48) | 1706 | 41 (32–53) | <0.001 |
| Positive pathergy test | 1540 | 38 (30–50) | 2641 | 38 (30–48) | 0.180 |
| Arthritis | 3294 | 39 (31–50) | 3007 | 38 (29–48) | <0.001 |
| Epididymitis (men only) | 247 | 38 (31–46.5) | 2150 | 40 (31–53) | 0.023 |
| Gastrointestinal symptoms | 1785 | 39 (30–52) | 4557 | 38 (31–48) | 0.038 |
| Vascular lesions | 683 | 43 (33–55.5) | 4833 | 38 (30–48) | <0.001 |
| Neurological manifestations | 1543 | 39 (31–51) | 4820 | 38 (30–49) | 0.004 |
| HLA-B51 positive | 1356 | 38 (30–49) | 1688 | 37 (29–46.25) | 0.022 |
P: Mann–Whitney test.
Sex and age subgroup
Prevalence of each manifestation at the registration was compared among subgroups stratified by 10-year increment of the registration age in male and female patients (Fig. 2). Most of the symptoms showed similar age dependency between male and female patients. Neurological manifestation, vascular lesion and gastrointestinal symptoms were more common in elderly onset patients than young onset patients, whereas oral ulceration showed the reverse pattern in both sexes.
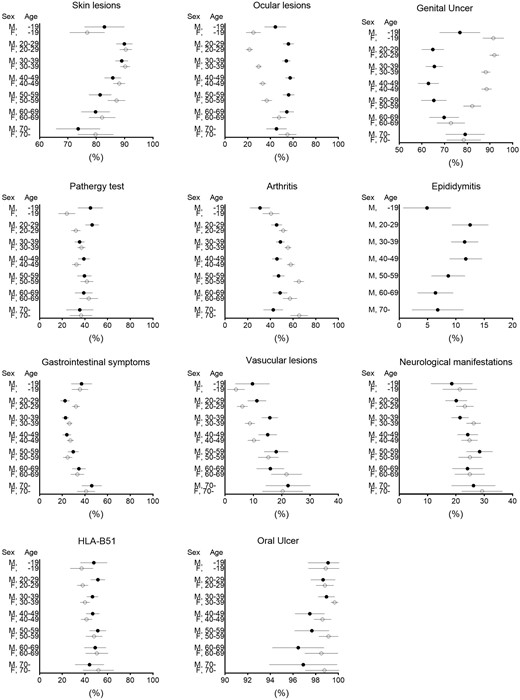
Subgrouping by sex and age of patients who satisfied International Criteria for Behçet’s Disease criteria
A filled/open circle indicates estimated prevalence. An error bar indicates 95% CI. Note that x axes were modified for each figure. M: male; F: female.
The association of HLA-B51 was also closer with young patients than elderly onset patients. Skin lesion and genital ulcer were more frequent in young adult patients with onset during reproductive age. This was the case for epididymitis seen only in males. On the other hand, we found different age-dependent patterns in ocular lesions and arthritis between male and female patients. Ocular lesion was more prevalent in elderly onset female patients than in males. The most prevalent generation of arthritis was the elderly female population, whereas it was the reproductive-aged population in males.
Sensitivity analysis using data from ISG criteria cases
Among 7950 analysable cases in our database, 5565 met ISG criteria. Some of ISG-required symptoms, namely oral ulceration (100.0%), skin lesion (95.8%), genital ulceration (79.2%) and pathergy test (41.7%), were more prevalent in ISG cases than ICBD cases. Contrarily, vascular lesion (10.4%) and neurological manifestation (21.9%), which is included in ICBD but not in ISG criteria, were less frequently observed in the ISG subset (Table 1).
In the ISG subgroup, female (P = 0.495) and young (P = 0.446) dominance of skin lesions that was observed in ICBD cases was not found. Female dominance of neurological manifestation (OR = 0.81, P < 0.001) was more clearly observed in this subset, but age difference of the neurological manifestations was not apparent (supplementary Tables S1 and S2, available at Rheumatology Online).
Otherwise, the results from analyses using patients who satisfied ISG criteria generally replicated those of our main analysis based on ICBD criteria though minor transitions of marginal statistical significance were revealed (supplementary Tables S1 and S2, available at Rheumatology Online). Subgroup analyses among ISG cases stratified by 10-year increment of the registration age and sex also revealed similar clinical presentation to those among ICBD cases. (supplementary Fig. S1, available at Rheumatology Online).
Discussion
We investigated age and sex differences in BD manifestation based on the database from a national registration system of intractable diseases in Japan. The data represent disease phenotypes at diagnosis in most of the patients, because the registration was directly connected to financial support for medical costs. Therefore, the clinical manifestations were little affected by therapies, though we and others have revealed that therapies, particularly immunosuppressive agents, suppress or prevent most symptoms besides the primary target organ involvement, resulting in modification of the disease process [17, 18]. In addition, compared with previous studies, our database had a much larger number of patients with individual manifestation data [8]. Although prevalence showed a linear increasing or decreasing trend for some symptoms, interestingly, a peak or a nadir of prevalence was observed for patients in their 20s to 40s for other manifestations. This reproductive generation overlaps the peak age of BD. It is also noted that the impact of age on symptom prevalence was not parallel for both sexes. Such age and sex differences of disease expression may provide insights into the mechanisms and phenotypes of BD. Another advantage of the current study is that our analysis was not affected by racial differences because we analysed data of only the Japanese population having homogeneous genetic backgrounds. Additionally, sex-specific subgroup analyses provided data free from the sex ratio in our country (Table 2 andFig. 2).
As expected, the present study reproduced the data of our previous smaller study that analysed 412 patients from two university hospitals in Japan [19]. Similarly, most of the results in the present study were generally compatible with those from the published reports, though some discrepancies were found presumably due to difference of race, data collection method and analysis technique. Because our national registration database is very large, we could assess the prevalence of each age/sex subgroup (Fig. 2), which we believe to be informative.
A systematic review by Bonitsis et al. [8] analysed data of more than 10 000 patients from 53 reports. According to this review, ocular involvement (relative risk = 1.34, 95% CI: 1.24, 1.45), pathergy test positive (relative risk = 1.14, 95% CI: 1.05, 1.23) and vascular involvement (relative risk = 2.27, 95% CI: 1.75, 2.93) were more frequently observed for men, while genital ulcers (relative risk = 0.92, 95% CI: 0.89, 0.96) and joint involvement (relative risk = 0.89, 95% CI: 0.83, 0.96) were more common for women. Our study replicated these results.
When compared with previous large-scale studies from Turkey [20] (n = 2313), Korea [21] (n = 1901) and Iran (n = 6075) [22], male predominance of ocular involvement and vascular involvement, and female predominance of genital ulcer were consistent among the studies. Another report from China also revealed that males had a more severe course and were at higher risk for losing vision than females [23]. Interestingly, our data were more similar to those from Korea than Turkey. Neurological involvement was more frequent in male Turkish patients, whereas the involvement was more prevalent in female Korean and Japanese patients. Ethnic differences in proportion of neuro-BD subgroups, parenchymal and non-parenchymal types may be involved in the discrepancy. Non-parenchymal types with male predominance are very rare in East Asia [24], whereas the type is found in 10–20% of neuro-BD patients in the Mediterranean region [25]. Another critical issue is difference in observation periods, because neurological involvement is recognized as a late-onset manifestation in general [24]. While our study focused on newly diagnosed patients, the Turkish study evaluated BD patients regardless of duration since the BD diagnosis [20]. The Korean study also revealed female predominance of oral ulcers, skin lesions and articular symptoms, all of which is compatible with our studies. The data suggest that genetic backgrounds and lifestyle affect the disease manifestations.
Age difference was investigated in studies with relatively small numbers of BD cases. Krause et al. [13] compared 59 BD paediatric and adult patients and showed that the first manifestation of paediatric BD was almost exclusively recurrent oral ulcer. However, less than one-third of adult BD patients presented first with oral ulcers. The trend was reproduced in the present study revealing the significant linear decline of oral ulcer prevalence in our analysis, though our previous study from Japan showed that oral ulceration was the most common initial manifestation even in adult patients [19]. The results of Krause et al. and our analysis together suggest that oral ulcer-negative BD might be missed by the ISG diagnostic, especially in adult and elderly onset patients. However, a proportion of the BD patients are categorized as non-oral ulcer BD patients, who have distinct clinical features including high prevalence of eye involvement and positive pathergy [26]. Timely institution of therapy in BD patients without oral ulcer may result in a favourable outcome [27].
Yazici et al. [12] collected data on 297 BD patients and concluded that ocular manifestation was more common for patients whose age at onset was 24 years or younger than those whose age at onset was 25 years or older. However, they did not detect an age difference for the other manifestations. Hamzaoui et al. [11] compared 81 cases with age at onset before 20 years and 68 cases with age at onset after 40 years of age. In their report, skin lesions were more common for the younger group, whereas articular involvement was more common for the elder group. Otherwise, the study failed to show age dependency in most of the manifestations. The key advantage of our study over these published analyses is its statistical power supported by the large number of cases. Therefore, we were able to detect a subtle change of prevalence depending on the patient generation.
Among the evaluated symptoms, genital ulcer and ocular manifestations showed a characteristic trend of prevalence based on both sex and age (Tables 2 and 3, Fig. 2). This was also reproduced in ISG patient sensitivity analyses (supplementary Tables S1 and S2, supplementary Fig. S1, available at Rheumatology Online). Women of reproductive age had a remarkably high risk of genital ulcers and a low risk of ocular manifestations whereas the reverse findings were found in the same generation of male patients. It seems that genital ulceration and ocular lesions presented exclusively (Fig. 2). Previous studies have suggested that sex hormones may affect both symptoms [28–31]. In support of the potential role of oestrogens in predisposing to collagen vascular diseases, the Nurse’s Health study showed that women with early menarche or treated with oestrogen-containing regimens such as oral contraceptives or postmenopausal hormone replacement therapies have a significantly increased risk for SLE [32, 33]. Further research is necessary to clarify the impact of complexed female hormones on the disease manifestation of BD [28–31].
We should comment on a few limitations of this study. First, we only used data on newly diagnosed patients. However, clinical manifestations evolve along the clinical course, as we have previously shown [19]. Unfortunately, our study did not directly provide data on BD symptoms after a long follow-up and data regarding BD treatment, though our study has the advantage of avoiding various external factors such as treatment. Second, we could not obtain data from a certain proportion of patients because of the questionnaire design, which allowed the physicians to answer Unclear to some symptoms and findings, especially the pathergy test and HLA-B51, which were not counted as major/minor symptom for Japanese BD diagnostic criteria. Although this may slightly reduce the data quality, all the items were supported by a sufficiently large amount of data.
In conclusion, the present study revealed that clinical phenotype in early phase of BD was different depending on onset age and sex.
Acknowledgement
We would thank the Japanese Ministry of Health, Labour and Welfare for providing the nationwide BD registration database.
Funding: This work was partly supported by the Health and Labour Sciences Research Grants (Research on Intractable Diseases) from the Ministry of Health, Labour and Welfare of Japan.
Disclosure statement: The authors have declared no conflicts of interest.
Supplementary data
Supplementary data are available at Rheumatology Online.
References
Japanese Ministry of Health, Labour and Welfare. Statutory intractable diseases implemented on January 1st, 2015.

{kind=link}
{kind=link}
Comments