





Abstract
Cryolipolysis is a proven and effective means of fat reduction; however, there are no standardized means of measuring volume reduction.
We aim to assess the volume loss using a 3-dimensional (3D) analysis following submental cryolipolysis.
A retrospective cohort study between April 2016 and August 2018 was performed. Thirty-five patients underwent a single 45-minute cycle of cryolipolysis to the submental region using the CoolSculpting System. A 3-fold analysis was performed employing an independent observer assessment of 2-dimensional photographs and 3D volumetric analysis utilizing the Vectra XT system, and patient satisfaction was measured with the FACE-Q questionnaire.
Our results suggested the mean (standard deviation) pretreatment volume (n = 35) was 104.12 cm3 (28.78). The 6-week mean posttreatment volume (n = 26) was 81.55 cm3 (21.29). The mean volume reduction found at 6 weeks posttreatment showed a reduction of 22.46 cm3 (19.10) (95% CI 14.74 to 30.17, P < 0.0001). The 12-week mean posttreatment volume (n = 24) was 82.24 cm3 (23.97). The 12-week posttreatment demonstrated a reduction of 22.30 cm3 (14.04) (95% CI 16.37 to 28.23, P < 0.0001). The mean percentage correct for each reviewer correctly identifying the pretreatment and posttreatment photograph was 76.33% (7.14). Patient satisfaction showed a mean FACE-Q score of 54.10 (20.41).
The study further affirms that submental cryolipolysis is an efficacious and safe, noninvasive method for reducing submental adiposity resulting in notable patient satisfaction rates. Furthermore, results suggest that patients can have a volume loss of about 20% on average, allowing them to be more confident and comfortable with their appearance.

The submental area has been identified as a difficult location for weight loss. It has been suggested that submental fat accumulation ranks highly as an area of aesthetic concern.1,2 Moreover, it has been demonstrated that this concern causes changes in behavior such as the avoidance of photos and the growth of a beard.3 Contributing factors to submental fat accumulation include age, diet, lifestyle, and genetic predisposition.4-6
Cryolipolysis is a noninvasive fat reduction treatment that has gained popularity given the rising use of nonsurgical aesthetic treatments. The American Society for Aesthetic Plastic Surgery published in their 2017 statistics that nonsurgical fat reduction had increased by 24.7%.7 This is due to the lack of surgical complications, recent technological advances, and increasingly positive public perception.7 Cryolipolysis utilizes controlled cooling to selectively damage adipocytes while not affecting surrounding tissue. The proposed mechanism of action is that the selective cooling induces panniculitis. This results in the apoptosis of adipocytes, while water-rich cells remain unaffected.6,8-10 Cryolipolysis is utilized for treatment of the abdomen, arms, back, buttocks, submental area, and thighs.11-13 Although cryolipolysis has a limited complication profile, a complication of note is paroxysmal adipose hypertrophy.13,14 However, it is widely employed and accepted as both a safe and effective method of treatment for fat reduction.14
Assessing aesthetic surgery outcomes is difficult because beauty is subjective (ie, “beauty is in the eye of the beholder”). Therefore, the notion of success largely depends on subjective rather than traditional objective measurements. The safety and efficacy of cryolipolysis has been extensively reported in the literature. The clinical outcomes following submental cryolipolysis have been measured by means of caliper measurements, patient satisfaction, observer impression, MRI, and ultrasound (USS).9,15-17 It has been shown to produce visually perceptible outcomes with a high patient satisfaction rate while also being well-tolerated and safe.18 The adverse outcome profile for cryolipolysis is minimal. Erythema, edema, and numbness are the most common complications, which tend to resolve within weeks of treatment.15
To date in the literature there is only 1 other study that has used 3-dimensional (3D) image analysis to assess volume loss. This was a prospective, nonrandomized study with a small patient group (n = 14).9 The aim of the present study was to expand on this further with a larger patient cohort and evaluate differences. The 3D imaging analysis, independent observer impression, and patient satisfaction scores were utilized to analyze submental volume reduction and therefore comment on efficacy of submental cryolipolysis.
METHODS
A retrospective, nonrandomized interventional cohort study was performed with patients treated from April 2016 to August 2018. Patients were recruited consecutively. We did not have set inclusion and exclusion criteria; however, we did exclude a single patient who had 2 treatments 12 months apart in the study to allow for accurate assessment, standardization, and statistical analysis.
All patients consented to the treatment and were informed of the side-effect profile and possible adverse effects of cryolipolysis. Prior to the collection of data and subsequent analysis, consent was obtained from each patient for permission to use information from their patient file. The present study was performed in accordance with the Declaration of Helsinki and its later amendments. Patients were provided with study information with adequate time to read and understand the information.
Patients
A total of 35 patients underwent submental cryolipolysis treatment (n = 35). Thirty-two of the patients were females and 3 were male. Patients were between the ages of 23 and 71 years. All patients had visible submental fullness, which affected their body perception. Submental tissue was assessed for pliability to ensure it could be drawn into the cryolipolysis cup applicator. A single investigator (K.S.) assessed suitability for treatment for all patients.
Cryolipolysis Treatment
All patients underwent a solitary treatment at a single institution. The area for treatment was based on one investigator’s assessment of the submental area. Each patient was individually assessed for submental fullness. The participant was asked to contract their platysma muscles with their head in a neutral position. Once this was done, the submental fullness was manipulated to assess whether the area would be suited to one singular application. A size template was employed to assess the area for treatment.
The treatment was performed following the protocol for the CoolMini applicator (Supplementary Figure 1, available online at www.aestheticsurgeryjournal.com) for the CoolSculpting System (Allergan USA Ltd, Dublin, Ireland). All patients undertook a 45-minute treatment with a maximum cooling temperature of –11°C. A small volume cup 3 × 8 cm (CoolMini Applicator) was applied to the marked treatment area. The vacuum drew the tissue filling the applicator to its full depth; the aim was to place the applicator centrally over the fullest palpable area.
Before treatment, the skin was cleansed and a transparent gel applied to the treatment area and the vacuum applicator covered with the supplied plastic cover and gel trap. During treatment, the participants were seated at approximately 120 degrees with their head placed in an Allergan Aesthetics foam cool-mini pillow. The vacuum applicator was positioned and the vacuum initiated. Foam straps are attached to Velcro on the sides of the applicator to Velcro on the sides of the pillow to create stability and patient comfort (Supplementary Figure 2, available online at www.aestheticsurgeryjournal.com).
At the termination of the treatment the applicator was removed. Immediately following the completion of the treatment protocol and subsequent removal of the applicator, photographs were taken before a gentle massage of the submental area. Figure 1 shows an example of an immediate posttreatment image and demonstrates the typical appearance of postcryolipolysis tissue. The posttreatment swelling lasts for 2 minutes and the massage process rewarms and reshapes the tissue. The swelling then subsides and there is a small amount of remnant erythema. All patients tolerated the treatment with minimal discomfort. There were no adverse lasting effects experienced by any of the patients.

Photograph of this 37-year-old female showing the immediate posttreatment appearance. The posttreatment swelling lasted for 2 minutes and the massage process rewarms and reshapes the tissue.
Image Analysis
Standardized (2-dimensional) clinical photographs of each patient were captured including frontal, left, right, and three-quarter views. This was performed utilizing an in-house photo studio and cataloguing system (Clinical Imaging, Melbourne, Victoria); pretreatment, 6-week, and 12-week posttreatment photographs were taken. 3D stereo-photogrammetric photos of the face and neck were captured utilizing the Vectra XT system (Canfield Scientific, Inc., Fairfield, NJ). Patients were placed against a standardized color background for the photographs.
Quantitative 3D analysis was performed with the Vectra XT system. The VECTRA analysis module software was utilized to quantify volumetric loss. The pretreatment and 6- and 12-week photos were analyzed. The photos were precisely matched to orientation utilizing facial features (nasal tip and forehead) with the patient positioned in the horizontal Frankfort plane. The volume was then calculated from the area of interest utilizing the predetermined anatomical landmarks: left gonion, mental protuberance, right gonion, and laryngeal prominence.
Figure 2 displays the landmarks utilized to calculate the submental area. Figure 3 shows the highlighted area that was calculated employing the VECTRA analysis module software. The volumes were measured by a single investigator (K.S.). These values were reassessed 3 times to ensure the results were reproducible. An independent reviewer (J.S.) selected 10 patients and assessed volumes based on the instructions provided to calculate volume loss, utilizing the designated landmarks conveyed in the method. An inter-rater reliability was calculated.

(A) Landmark placed on the mental protuberance on this 27-year-old female. (B) Landmark placed on the right gonion. (C) Landmark placed on the laryngeal prominence. Note the right gonion and mental protuberance landmarks in relation. (D) Landmark placed on the left gonion.

(A) Inferior, (B) lateral, and (C) frontal views of the area calculated on this 27-year-old female (the same patient featured in Figure 2).
A total of 15 patients had a measured result at 6 and 12 weeks, 9 patients had measured results at 12 weeks only, and 11 patients had measured data at 6 weeks only. Given this, each group was assessed separately with all available values. One-sample t test analysis was utilized to analyze the submental region volume difference. A repeated-measures test was employed to analyze the difference between 6- and 12-week data. The 6-week and 12-week percentage reductions were calculated by dividing the mean volume reduction by the pretreatment volume.
Patient Satisfaction
Patient satisfaction was determined with FACE-Q satisfaction of outcome scoring. Rasch measurement theory leads to the utilization of 6 questions with a 4-point scale to measure patient satisfaction. The raw score out of 24 is then converted to a number out of 100 by the FACE-Q scoring system; this is a nonlinear scale and not a percentage. This method of satisfaction of outcome measurement has been shown to be reliable and responsive to clinical change.19 The FACE-Q questionnaire was completed at 12 weeks posttreatment. Linear regression analysis was employed to assess the correlation between volume difference and patient satisfaction scores.
Blinded Independent Panel
The pretreatment and 6- and 12-week posttreatment photos were then reviewed by 7 blinded independent observers. This observer group was comprised of nurses, occupational therapists, and members of the general public. The pretreatment and posttreatment photos were shown to each observer individually, who were then asked to identify the posttreatment photo. A 1-sided exact binomial test was utilized to determine statistical significance of the results. Linear regression analysis was employed to assess the correlation between volume difference and blinded observer accuracy. All statistical analysis was performed in 2018 Microsoft Excel (Microsoft, Redmond, WA).
RESULTS
Patients who underwent the cryolipolysis treatment ranged in age from 23 to 71 years (mean, 49.1 [SD, 14.5] years). Figures 4 and 5 show pretreatment and posttreatment photographs of representative patients. Figures 6 and 7 show comparative profile photographs overlaid on the original image to highlight the volume loss following submental cryolipolysis. The mean follow-up time was 12.97 weeks [range (SD), 6-36 weeks (6.7)].


(A, C, E) Pretreatment and (B, D, F) 12-week posttreatment photographs of this 60-year-old female.
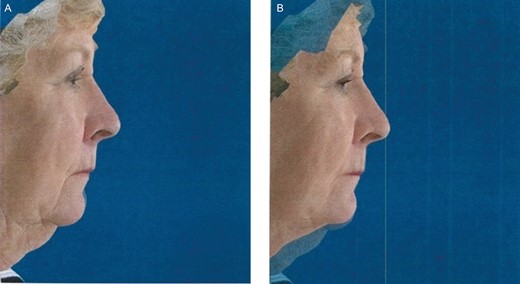
(A) Pretreatment lateral image of this 71-year-old female. (B) Superimposed image at 12 weeks posttreatment displaying the difference in reduction posttreatment.
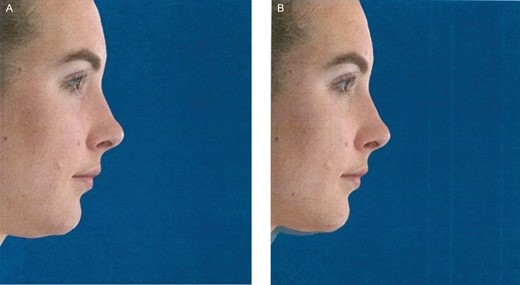
(A) Pretreatment lateral image of this 27-year-old female. (B) Superimposed image at 12 weeks posttreatment displaying the difference in reduction posttreatment.
Quantitative 3-Dimensional Analysis
3D images were analyzed to quantify the total volume lost following treatment. All patients were included in the review. The volumes were measured by a single investigator (K.S.). An independent reviewer (J.S.) selected 10 patients and assessed the volume difference. An inter-rater reliability was calculated yielding a Kappa value of 0.93. The pretreatment study area (n = 35) mean (SD) was 104.12 cm3 (28.78) with a minimum of 64.53 cm3 and a maximum of 186.7 cm3. The 6-week posttreatment study area (n = 26) mean (SD) was 81.55 cm3 (21.29) with a minimum of 40.74 cm3 and a maximum of 128.8 cm3. The 12-week posttreatment study area (n = 24) mean (SD) was 82.24 cm3 (23.97) with a minimum of 49.36 cm3 and a maximum of 128.1 cm3. The mean volume reduction found at 6 weeks posttreatment showed a reduction of 22.46 cm3 (SD, 19.10) (95% CI 14.74 to 30.17, P < 0.0001). The minimum volume reduction was 1.02 cm3 and the maximum volume reduction 89.70 cm3. The 12-week posttreatment demonstrated a reduction of 22.30 cm3 (SD, 14.04) (95% CI 16.37 to 28.23, P < 0.0001). The minimum volume reduction was −0.74 cm3 (volume increased) and the maximum volume reduction 46.49 cm3. This demonstrates a statistically significant volume reduction for all follow-up time periods.
The mean 6-week posttreatment percentage reduction was 20.28%. (SD, 13.71; range, 1.57%-57.87%) The mean 12-week posttreatment percentage reduction was 20.46% (SD, 11.29; range, −1.14%-48.50%). Table 1 displays volume loss in square centimeters and displays the percentage lost at the 6-week and 12-week reviews.
Percentage and Total Volume Reductions at 6 and 12 Weeks
| Summary | 6 weeks | 12 weeks |
|---|---|---|
| No. of patients | 26 | 24 |
| Mean preoperative volume, cm3 | 104.01 | 104.54 |
| Mean volume reduction, cm3 | 22.46 | 22.30 |
| SD volume reduction, cm3 | 19.10 | 14.04 |
| Mean volume reduction, % | 20.28 | 20.46 |
| SD volume reduction, % | 13.71 | 11.29 |
| Summary | 6 weeks | 12 weeks |
|---|---|---|
| No. of patients | 26 | 24 |
| Mean preoperative volume, cm3 | 104.01 | 104.54 |
| Mean volume reduction, cm3 | 22.46 | 22.30 |
| SD volume reduction, cm3 | 19.10 | 14.04 |
| Mean volume reduction, % | 20.28 | 20.46 |
| SD volume reduction, % | 13.71 | 11.29 |
Percentage and Total Volume Reductions at 6 and 12 Weeks
| Summary | 6 weeks | 12 weeks |
|---|---|---|
| No. of patients | 26 | 24 |
| Mean preoperative volume, cm3 | 104.01 | 104.54 |
| Mean volume reduction, cm3 | 22.46 | 22.30 |
| SD volume reduction, cm3 | 19.10 | 14.04 |
| Mean volume reduction, % | 20.28 | 20.46 |
| SD volume reduction, % | 13.71 | 11.29 |
| Summary | 6 weeks | 12 weeks |
|---|---|---|
| No. of patients | 26 | 24 |
| Mean preoperative volume, cm3 | 104.01 | 104.54 |
| Mean volume reduction, cm3 | 22.46 | 22.30 |
| SD volume reduction, cm3 | 19.10 | 14.04 |
| Mean volume reduction, % | 20.28 | 20.46 |
| SD volume reduction, % | 13.71 | 11.29 |
This study’s results show that the outcomes at 6 weeks were comparable to the outcomes at 12 weeks. We found that the mean difference between 6 and 12 week data (n = 15) was 1.15 cm3 (SD, 14.59) (95% CI −6.93 to 9.23, P value 0.77). This showed that there was a small loss in volume from weeks 6 to 12. However, given that this was not statistically significant, the 6- and 12-week volume differences show no evidence of being different.
Patient Satisfaction
Patient satisfaction was then assessed utilizing the FACE-Q questionnaire—satisfaction of outcome scoring. These questionnaires were provided to all patients following their 12-week review. The response rate of the FACE-Q questionnaire was 57%. Patient satisfaction is measured with nonlinear scores ranging from 0 (lowest) to 100 (highest). The mean FACE-Q score was 54.10 (SD, 20.41) with a median of 59 years (range, 0-79 years). The mean volume difference for those who responded was 24.035 cm3 (SD, 14.40; range, 6.44-55.95). The mean observer score for those who responded was 5.50 (SD, 1.28; range, 2-7). Individuals scoring either a 3 or a 4 on the FACE-Q questionnaire eluded to a positive response. The results indicated that 76% of the respondents were pleased with their results, 66% thought the results turned out great, 57% of the respondents expressed they were surprised to see how good they looked in the mirror, and 38% and 42% of the patients thought the results were either fantastic or miraculous. One patient was unhappy with the result despite a volume loss of 55.95 cm3 and gave a FACE-Q score of 0%, which inevitably skewed the results.
Blinded Independent Panel
Noticeable reduction of submental fullness was demonstrated in the standardized photos. An independent blinded panel reviewed a pair of pretreatment and posttreatment photographs. The mean (SD) percentage correct for each reviewer was 76.33% (7.14) with a minimum of 68.57% and a maximum of 88.57%. The 1-sided exact binomial test determined the statistical probability (P < 0.0001) of the mean percentage correct (76.33%; 187/245) given what would be expected if observers could not distinguish between pretreatment and posttreatment photos (50%). For each patient, the percentage of correct reviewer assessments was also measured. The mean (SD) of this measurement was 5.34 (1.63) out of 7 or 76.33% (23.23) with a minimum of 14.29% and a maximum of 100% (95% CI 68.35 to 84.31, P < 0.0001).
Correlation Between Volume Reduction, Patient Satisfaction, and Independent Observer
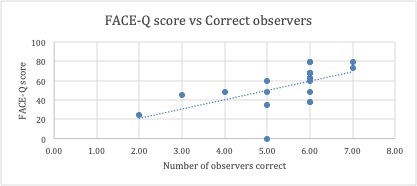
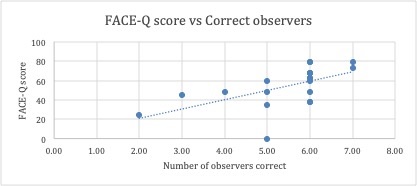
Linear regression analysis was employed to investigate the correlation between each patient’s measurements of efficacy. There was no correlation found between either FACE-Q and volume reduction or number of correct reviewers and volume reduction (R2 values of 0.0078 and 0.0623, respectively). However, there was a significant correlation between FACE-Q scores and number of correct reviewers (Supplemental Figure 3, available online at www.aestheticsurgeryjournal.com), with an R2 value of 0.336 (P =
0.0074). For psychology-based assessments, an R2 value of 0.10 or greater is considered adequate.20
Complications
The complications profile was minimal: 80% had posttreatment numbness, which lasted for 4 days on average; 8 patients reported they had erythema lasting 2 days while the others reported the erythema faded by the night of treatment; and 18 patients reported mild edema in conjunction with the numbness, which lasted on average 3 days. All patients reported a normal appearance and sensation by 2 weeks.
DISCUSSION
Cryolipolysis is a safe and effective solution for unwanted fat accumulation in the submental region. Numerous studies have displayed its efficacy and safety in this region.8-10,15 The present study aimed to quantify the efficacy of submental cryolipolysis by utilizing Standardized Clinical (2-dimensional) photographic images, FACE-Q scores, and 3D analysis. 3D analysis is a cost-effective means of measuring outcome without the patients having to undergo additional investigation to quantify reduction.
There have been numerous studies quantifying submental cryolipolysis volume loss. To our knowledge, there has been only 1 study to date that has reported 3D analysis outcomes for patients who underwent submental cryolipolysis treatment.10
The results demonstrated statically significant results in the 6-week and 12-week posttreatment measurements. 3D volume analysis found that the mean volume reduction at 6 weeks posttreatment showed a statistically significant difference of 22.46 cm3 (SD, 19.10). The 12-weeks-posttreatment values showed a statistically significant difference of 22.30 cm3 (SD, 14.04). Bernstein et al9 quoted a mean (SD) fat volume reduction of 4.82 cm3 (11.42) (95% CI –1.39 to 11.02 cm3). The present study showed a larger mean volume loss despite single treatment. The majority of the patients felt they received satisfactory results with a single treatment. However, this was our experience with the patient population presenting to the clinic. We acknowledge there is a role in second treatment, which must be determined on the case-by-case basis.
There are several possible factors contributing to the large volume reduction difference observed between our study and that of Bernstein et al.9 The submental area we analyzed was defined differently compared with the area noted by Bernstein. However, this area was chosen because the neck is viewed in entirety and not isolated to the submental area. Because the applicator cup sucks the tissue inward, we deemed it necessary to include areas outside those defined by Bernstein et al to estimate volume loss in the area as accurately as possible.
Sogyong et al found through their systematic review that there are inherent difficulties in outcome measurement of noninvasive therapies with no standardized measurement technique.21 A study by Kilmer et al showed a fat reduction of 2 mm by means of USS analysis of the fat layer.15 However, this modality does not measure volume reduction. 3D analysis has the benefit of being less invasive and forming part of routine patient investigation.
A total 15 patients in the present study had both 6- and 12-week data sets; the remainder had either 6-week or 12-week results. This was due to patients not attending appointments despite repeated attempts to contact them. Given the incomplete results, we decided to perform a repeated-measures t test between the results and found no statistically significant difference between the 6- and 12-week volume losses. The results simply suggest that at the 6-week review, the volume loss showed no statistical difference between the 6-week assessment of volume loss and 12-week assessment of volume. This implies that the 6-week volume difference may be a suitable indicator of longer term volume loss. This may suggest a shorter follow-up time is sufficient to perform a relatively accurate volume reduction assessment. However, longer follow-up may be necessary to monitor adverse effects.
The mean FACE-Q score for submental cryolipolysis was 54.10 (SD, 20.41). A study by Berger et al found that submental liposuction resulted in a mean FACE-Q score of 70.56 (SD, 23.52).22 Meanwhile, Sinno et al reviewed FACE-Q scores in patients who had undergone a neck lift and found a mean score of 78.1 (SD, 25.6).23 The satisfaction scores were inferior for cryolipolysis compared with both submental liposuction and surgical neck lift. However, cryolipolysis is a nonsurgical minimally invasive treatment modality with a minimal complication profile and no disadvantage compared with surgical intervention.24,25 Additionally, the results of the previous studies cannot be directly compared given that they were not performed at the same institution, treatments were not randomized, observers were not blinded to treatment, and demographics were not controlled. The utilization of an online FACE-Q questionnaire avoided the bias that could have potentially been caused by the patients reporting satisfaction to the clinic directly.26 The 57% response rate may have introduced selective bias because the response rate may have varied depending on satisfaction. This is supported by the fact that means of volume difference and observer score were higher in the respondent group compared with all patients. Although we cannot completely understand why some of the patients did not respond to the posttreatment questionnaire, a simple measure to rectify this would be to perform an assessment at the 6-week review to capture more data.
The mean (SD) number of correct observers for participants was 5.34 (1.63) out of 7, or 76.33% (23.22). This is slightly lower than the correct identification rate of Bernstein et al of 81.0%. However, the observers of the previous study were board-certified physicians in either plastic surgery or dermatology as opposed to the diverse observers of this study. This may explain the difference between this study’s correct identification rates compared with the previous study. In this study, we felt the chosen observer group better represented the general population, allowing for a nonmedical perception of the results and outcome.
Linear regression analysis allowed investigation of the correlation between outcome measurement modalities. There was no correlation between the objective (volume reduction) and subjective results (FACE-Q and number of correct reviewers). However, there was a significant correlation between FACE-Q score and number of correct reviewers. This is consistent with current literature suggesting that patient satisfaction is not associated with clinical results.9,22,23 The results suggest that patient satisfaction is an independent measure, which does not have an association with volume loss. One hypothesis is that FACE-Q score may not accurately capture the feeling of a patient’s result from the proposed treatment. The total score reflects how pleased a patient is with their result, and therefore a higher score alludes to the fact that they are ecstatic whereas a patient who expected a good result and responded appropriately may not have scored as high. Although skin quality may play a role in the overall result of the contour, the data did not reflect this. The patients who had more lax necks did not score poorly on the FACE-Q and expressed satisfaction with the outcome.
The fact that FACE-Q score is strongly correlated with correct number of reviewers suggests that observer opinion may be a valid method of measuring submental cryolipolysis results. Overall, these results suggest that aesthetic outcome is a subjective parameter. Therefore, results indicative of patient satisfaction should be considered as an adjunct to objective measures of outcome in this patient group. Current literature agrees with this notion, indicating that patient satisfaction is the outcome measurement, which should dictate the success of aesthetic procedures.
Limitations
Given the cohort of patients recruited in the study to undergo submental cryolipolysis, there is the possibility of sampling error within this study. This could not be avoided, because the cohort could not be standardized.
Although the definition of the submental area was consistent in all patients and a single investigator placed the landmarks, it is possible that the precise location of these landmarks differed slightly between patients, which may have affected results and in turn the volume calculations. We aimed to rectify this by utilizing an independent investigator who sampled 10 patients selected and then calculated the measured volume; our inter-rater reliability showed a kappa value of 0.93, indicating that the measurements were accurate.
Loss to follow-up was also an important concern in this study. The fact that patients were informed of the minimal risk of the treatment and low likelihood of complications may have contributed to low follow-up attendance. Consequently, some participants had only 1 posttreatment volume measurement. We compared the volume reduction between the 6- and 12-week data sets to assess the effect on results.
CONCLUSIONS
The present study further affirms that submental cryolipolysis is an efficacious and safe noninvasive method for reducing submental adiposity resulting in notable patient satisfaction rates. The results suggest that patients can have a loss on average of about 20% in volume of the submental region, allowing them to be more confident and comfortable with their appearance. The results for cryolipolysis are similar with published papers suggesting significant volume loss and patient satisfaction with a minimal adverse effect profile.
Disclosures
The authors declared no potential conflicts of interest with respect to the research, authorship, and publication of this article.
Funding
The authors received no financial support for the research, authorship, and publication of this article.
REFERENCES
Author notes
Mrs Spiteri is a registered nurse in private practice in Bendigo, Australia.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}