

Abstract
Wearing lead aprons and thyroid collars for long periods of time has a subjective component: to balance the effective dose reduction with the effort of carrying a heavy load. Occupational radiation exposure has decreased dramatically in the last century within the health care system. During the same period the use of lead aprons and thyroid collars has also gone up. Therefore, a question that may be raised is: how safe is safe enough? In order to promote stakeholder involvement, the aim of the present study was to investigate staff's experience of discomforts associated with wearing lead aprons and thyroid collars for long periods of time, and also to investigate staff's willingness to tolerate personal dose equivalent (expressed as radiation dose) and the corresponding increase in future cancer risk to avoid wearing these protective tools. A questionnaire was developed and given to staff working in operating or angiography rooms at Skaraborg Hospital in Sweden. The results from the 245 respondents showed that 51% experienced bothersome warmth, 36% experienced fatigue and 26% experienced ache or pain that they believed was associated with wearing lead aprons. One third of the respondents would tolerate a personal dose equivalent of 1 mSv per year to avoid wearing lead aprons, but only a fifth would tolerate the corresponding increase in future cancer risk (from 43% to 43.2%). In conclusion, discomforts associated with wearing lead aprons and thyroid collars for long periods of time are common for the staff using them. At the same time, only a minority of the staff would tolerate a small increase in future cancer risk to avoid wearing them. The present study gives an example of stakeholder involvement and points at the difficulties in making reasonable decisions about the use of these protective tools.
Export citation and abstract BibTeX RIS

Original content from this work may be used under the terms of the Creative Commons Attribution 4.0 license. Any further distribution of this work must maintain attribution to the author(s) and the title of the work, journal citation and DOI.
1. Introduction
Short after the discovery of x-rays, Antoine Béclère introduced lead aprons as a protective tool [1]. In 1935 approximately 60% of radiographers working in the U.S. were using lead aprons, 35 years later (in the 1970s) the proportion was estimated to be 97% [2]. During the last decades the use of thyroid collars has also gone up [3], from 47% reported in 1993 by Niklason et al [4] to 94% reported in 2013 by Lynskey et al [5].
The obvious benefit of these protective tools is their capability of dose reduction, for lead aprons the effective dose reduction is estimated to be 75%–97% [6, 7] and for thyroid collars it is around 50% [4, 8]. However, lead aprons and thyroid collars are associated with drawbacks [9]. By using an infrared camera, Alexandre et al [10] have shown that working in an operating room with lead aprons gives an increased temperature of the skin for several muscle groups opposed to working without. They concluded that this increase in temperature is associated with increased muscular activity and fatigue. Another serious drawback with lead aprons is the link between back pain and working with lead aprons for long periods of time [3, 11–18]. For example, a survey conducted in China in 2022 (with 1044 respondents) reported that interventional cardiologists had a significantly higher incidence of body pain compared to non-interventional cardiologists (56.6% versus 24.2%) [17]. To ease the workload, solutions with 20% lighter aprons (mainly consisting of tungsten and tin) have been developed [19]. Also, ceiling-suspended lead aprons are available on the market [20].
During the last century, a dramatical decrease in occupational radiation exposure has been reported [2, 21–23]. In a cohort study of 88 000 U.S. radiographers, a 72% decline in badge doses from the 1930s to the 1950s could be seen, furthermore, from the 1950s to the end of the 1970s another decline of 92% was reported [2]. For radiologists, their effective doses in the 1920s could have been as high as several hundreds of mSv per year, and after the year of 2000 it has been reported to be less than 0.25 mSv per year [21]. UNSCEAR has reported that the worldwide average effective dose within diagnostic radiology has decreased from 0.9 mSv per year in the late 1970s to 0.4 mSv per year in early 2010s [23]. Vano et al [22] reported that during the 15 years between 1989 and 2004 the mean annual effective dose for interventional cardiologists decreased from 11.2 mSv down to 1.2 mSv per year. Despite the drawbacks with lead aprons and the decrease of occupational radiation exposure, it is still often recommended that lead aprons should be worn by all staff working with fluoroscopy [8, 24, 25].
The limit on the effective dose for occupational exposure is set to be 20 mSv per year by the European Union [26]. At current levels of occupational exposure within the healthcare system, some of the staff can work without lead aprons and thyroid collars and still fall below the dose limit. According to the European legislation [26] it is the so-called radiation protection expert that gives competent advice on optimisation of occupational exposure. The principle of optimisation of protection (also known as the ALARA principle) is one of the key principles of radiological protection stated by the International Commission on Radiological Protection (ICRP) [27]: 'The likelihood of incurring exposure, the number of people exposed, and the magnitude of their individual doses should all be kept as low as reasonably achievable, taking into account economic and societal factors'. In this context, ICRP also expresses that radiological protection comes with a cost for society, which can include work, time, materials or even risks [28]. Furthermore, ICRP states that optimisation should not be seen as minimisation, the best solution is not always the one with the lowest dose [29]. They also stress the importance of stakeholder involvement in radiological protection [29]. When it comes to lead aprons, ICRP declares that they are likely to have a negative impact of working efficiency, and this factor should be considered in the decision of using them [30].
One way to work with the ALARA principle is to use cost-benefit analysis. When only focusing on costs and effective dose reduction, it has been shown that the use of a single lead apron needs to avert a collective effective dose of 0.26 man.mSv per year (for a single thyroid collar 0.044 man.mSv per year), otherwise these investments can be considered to be too expensive in a health economics perspective [31]. In another cost-benefit analysis, Russell and Hufton [32] showed that the maximum recommended lead equivalence for the average radiologist is 0.35 mm.
Several studies [33–36] have shown that during some procedures anaesthesia personnel receive just a few micro-sievert and therefore concluded that the use of lead aprons during these procedures is questionable. Mori et al [37] estimated that for interventional cardiologists an exchange of lead aprons from 0.25 mm to 0.5 mm would bring an effective dose reduction of 2.2 mSv per year. However, since wearing an even heavier lead apron for long periods of time would expose the cardiologists to an extra risk of getting back pain, they concluded that this was not recommended.
According to Huda and Boutcher [38] the ALARA principle has a laudable intent, but it is also problematic. Wearing lead aprons and thyroid collars for long periods of time have a subjective component: to balance the effective dose reduction with the effort of carrying a heavy load. For technologists working in nuclear medicine, Huda and Boutcher [38] described an efficiency parameter for lead aprons, where the effective dose reduction in different situations was divided with the time spent by the technologists wearing the lead apron. They concluded that technologists could choose their own strategy when it comes to the decision of wearing lead aprons.
In order to promote stakeholder involvement, the aim of the present study was to investigate staff's experience of discomforts associated with wearing lead aprons and thyroid collars for long periods of time, and also to investigate staff's willingness to tolerate personal dose equivalent (expressed as radiation dose) and the corresponding increase in future cancer risk to avoid wearing these protective tools. The staff worked as physicians, radiographers, nurses, and assistant nurses in operating or angiography rooms.
2. Method
The present study was approved by the Swedish Ethical Review Authority (Dnr 2021–03027) and written informed consent was obtained from all the respondents. The research was conducted in accordance with the principles embodied in the Declaration of Helsinki and in accordance with local statutory requirements.
To investigate staff's willingness to wear lead aprons and thyroid collars for long periods of time, a questionnaire with 21 items was developed in the present study. Face validity [39] of the questionnaire was established by four medical engineers, and content validity [39] was established by four medical physicists. The questionnaire was pilot tested [39–41] on respondents, seven radiographers working in the field of interventional radiology. A small number of respondents can be enough to discover deficiencies in a questionnaire [41].
The questionnaire was handed out to 255 members of the staff (physicians, radiographers, nurses and assistant nurses) at Skaraborg Hospital in Sweden from January to September in 2022. The physicians', the nurses' and the assistant nurses' knowledge of radiological protection primarily comes from a radiation safety education given to them every three years (for one hour) at Skaraborg Hospital. Radiographers (a small proportion of the respondents) have a university education in radiological protection. The questionnaire was handed out to the staff right before their periodical radiation safety education. In this way the respondents can be seen as a captive group which usually gives a high response rate [40].
2.1. The questionnaire
In the questionnaire, items 1–3 were subject descriptors of occupation, sex, and age. Items 4–7 asked the respondents to estimate the numbers of years and hours per week they have been using lead aprons and thyroid collars in their work. Items 8–16 asked about the respondents' experience of discomforts (bothersome warmth, fatigue, ache or pain) associated with wearing lead aprons and thyroid collars. For example (item 14), 'Do you or have you previously experienced any ache or pain from your neck, shoulders or back? (Yes/No)' and (item 15) 'If so, do you experience that this ache or pain comes from or is exacerbated by wearing lead aprons in your work? (Yes/No)'. Items 17 and 18 asked the respondents on how much radiation dose per year (personal dose equivalent) they are willing to tolerate to avoid wearing lead aprons and thyroid collars. As an aid for the respondents' estimations, they were given information about the natural background radiation in Sweden for non-smokers, an effective dose of 1.3 mSv per year [42]. In items 19 and 20 the respondents were asked similar questions, but instead of personal dose equivalent the concept was cancer risk, how much excess future cancer risk are they willing to tolerate to avoid wearing these protective tools. For item 19, an aid was presented of the baseline future risk for 25 year-olds to develop cancer (as a mean of male and female risks), to be approximately 43% [43]. For item 20, the baseline future risk for thyroid cancer was presented as 0.4% [43]. In surveys, respondents often have difficulties to handle different magnitudes of risk, referred to as scale insensitivity [44]. Therefore, aids (like these ones) can be presented to help respondents with their risk estimations [44, 45]. For example, item 19 was phrased like this: 'The risk for 25 year-olds to receive a cancer diagnosis at some point during the rest of their lives is estimated at 43%. In exchange for not having to use lead aprons during your working life. How large increase in future cancer risk would you tolerate? From 43% (to 60%, to 50%, to 47%, to 45%, to 44%, to 43.2%, to 43.02%, to 43.002%), or No increased risk at all, or I do not want to take a position.' Item 21 asked the respondents about their opinions on rules regarding lead aprons and thyroid collars.
2.2. A link between personal dose equivalent and future cancer risk
To be able to compare the respondents' answers between item 17 (their willingness to tolerate personal dose equivalent) and item 19 (their willingness to tolerate an increase in future cancer risk) an organ dose estimation method developed by Simon et al [2] and progressed by Choi et al [46], and the RadRAT program [43] were used. This approach has been used by Lee et al [47] to estimate excess lifetime cancer risks among diagnostic medical workers in South Korea.
To estimate organ absorbed doses (DT) for both males and females from measured personal dose equivalents Hp(d), two conversion coefficients from ICRP were used: the organ absorbed dose per unit of air kerma free-in-air (DT/Ka) [48] and the personal dose equivalent per unit of air kerma free-in-air (Hp(d)/ Ka) [49]. Organ absorbed doses can be calculated by equation (1)

The predominant energy in scattered diagnostic radiation fields was assumed to be 35 keV [2, 46], therefore organ absorbed doses calculated from conversion coefficients of 30 keV and 40 keV were used for interpolations. Furthermore, the staff were assumed to be turned towards the patient when exposed to scattered radiation [2, 46]. In this way, organ absorbed doses (DT) were calculated for males (16 organs) and for females (18 organs) from a personal dose equivalent Hp(10) of 1 mSv per year.
The RadRAT program [43] is a radiation risk assessment tool developed by the National Cancer Institute in the US. The program is based on risk models described by the BEIR VII committee [50, 51]. Exposure scenarios for males and females, exposed to chronic ionizing radiation between the age of 25 and 65 (assumed working age), corresponding to a personal dose equivalent Hp(10) of 1 mSv per year were calculated by Monte Carlo simulations (sample size of 300) in the RadRAT program. Excess future cancer risks (the risk that a population will develop radiation-induced cancer from present time until the end of expected lifetime) were calculated for 16 organs (cancer sites) for males and 18 organs for females. The total excess future cancer risk was summed from all the cancer sites for males and females respectively [50, 51]. A 90% uncertainty interval was expressed by the RadRAT program, based on both statistical and subjective components [51]. The cancer site 'the remainder' expressed in ICRP Publication 116 [48] includes 14 organs, five of these were calculated separately in the RadRAT program. Therefore, the organ absorbed dose to the corresponding 'other and ill-defined sites' in the RadRAT program was multiplied with a factor of (9/14).
The link between item 17 (the respondents' willingness to tolerate personal dose equivalent) and item 19 (the respondents' willingness to tolerate an increase in future cancer risk) is presented in table 1. By using the Monte Carlo simulations in the RadRAT program corresponding to a personal dose equivalent Hp(10) of 1 mSv per year, the excess future cancer risks for the other seven levels of personal dose equivalents were calculated by extrapolations. To not reveal the link between item 17 and item 19 for the respondents, three out of eight levels of personal dose equivalents were excluded from item 17. If a respondent tolerated a level of future cancer risk without a corresponding level of personal dose equivalent, this answer was downgraded to the nearest level of future cancer risk with a corresponding level of personal dose equivalent. As can be seen in table 1, the excess future cancer risks are higher for females compared to males. Therefore, when expressing the total future cancer risks in item 19, the excess future cancer risks for females were chosen as a precautionary. For items 18 and 20 (about thyroid collars), the excess future thyroid cancer risk was calculated in the same way as described above and used as a link between these items.
Table 1. The link between item 17 expressed as personal dose equivalents (mSv per year) and item 19 expressed as an increase from baseline future cancer risk to total future cancer risk (%), for 25 year-olds assumed to work up to an age of 65.
| Item 17, personal dose equivalent (mSv/y) | Female, excess future cancer risk, cases per 100 000 (90% uncertainty level) | Male, excess future cancer risk, cases per 100 000 (90% uncertainty level) | Item 19, from baseline future cancer risk to total future cancer risk (%) |
|---|---|---|---|
| 100 | 17 570 (6520–38 110) | 10 830 (3370–26 560) | From 43% to 60% |
| 40 | 7028 (2608–15 244) | 4332 (1348–10 624) | From 43% to 50% |
| 20 | 3514 (1304–7622) | 2166 (674–5312) | From 43% to 47% |
| 12 | 2108 (782–4573) | 1300 (404–3187) | From 43% to 45% |
| 6 | 1054 (391–2287) | 650 (202–1594) | From 43% to 44% |
| 1 | 175.7 (65.2–381.1) | 108.3 (33.7–265.6) | From 43% to 43.2% |
| 0.1 | 17.6 (6.5–38.1) | 10.8 (3.4–26.6) | From 43% to 43.02% |
| 0.01 | 1.8 (0.7–3.8) | 1.1 (0.3–2.7) | From 43% to 43.002% |
a These levels of personal dose equivalents were excluded from item 17.
2.3. Analyses
Normal approximation to binominal proportions was used to calculate 95% confidence intervals (CI) of the proportions of respondents that experience discomforts (bothersome warmth, fatigue, ache or pain) associated with wearing lead aprons and thyroid collars. Differences between subgroups of respondents were analysed by calculating absolute differences between proportions (with 95% CI).
Wilcoxon signed-rank tests were performed to analyse differences in the respondents' willingness to tolerate personal dose equivalent and their willingness to tolerate an increase in future cancer risk. Mann–Whitney U tests were used to analyse differences between subgroups of respondents. In cases where several independent variables showed a significant association (p < 0.05) with a dependent variable a multivariate ordinal regression analysis and stratified univariate analyses were performed.
3. Results
In the present study, the response rate was 96% and the number of analysed answers were 245. The respondents worked in operating or angiography rooms as physicians (50%), nurses or radiographers (42%) and assistant nurses (9%). The distribution between the sexes was 44% males and 56% females. Of the respondents, 41% were in the age group of 20–39 years old, 50% were 40–59 years old and 9% were 60 years or older. The respondents' experience of working with lead aprons was: <1 year (9%), between 1–4 years (25%), between 5–10 years (18%) and >10 years (48%). Their use of lead aprons in the last 12 months was: <1 h/w (28%), 1–4 h/w (39%), 5–10 h/w (18%) and >10 h/w (14%). Of the respondents, 6% reported on experience of working with lead aprons but not with thyroid collars. Apart from this group, the respondents' experience and use of lead aprons and thyroid collars were similar.
For frequent users of lead aprons (>10 h/w), 80.0% (95% CI 66.7–93.3%) reported on former or present ache or pain in their neck, shoulders or back. The corresponding proportion for infrequent users (⩽10 h/w) was 59.3% (95% CI 52.6–66.1%). The absolute difference between these groups was calculated to be 20.7 percentage points (95% CI 5.8–35.6 percentage points).
Out of all of the respondents: 50.8% (95% CI 44.5–57.1%) experienced bothersome warmth, 35.7% (95% CI 29.6–41.7%) experienced fatigue and 25.9% (95% CI 20.4–31.5%) experienced ache or pain that they believed came from or was exacerbated by wearing lead aprons. Discomforts associated with wearing thyroid collars were less common: 31.3% (95% CI 25.2–37.3%) experienced bothersome warmth, 13.2% (95% CI 8.8–17.5%) experienced fatigue and 6.7% (95% CI 3.4–9.9%) experienced ache or pain. Table 2 shows numbers, proportions, absolute differences, and CI of respondents who experienced discomforts (bothersome warmth, fatigue, ache or pain) and believed that these discomforts came from or was exacerbated by wearing lead aprons or thyroid collars. Compared to physicians, a significantly higher proportion of nurses (including radiographers and assistant nurses) reported on bothersome warmth associated with wearing both lead aprons and thyroid collars. Significant absolute differences could be shown between frequent user (>10 h/w) and infrequent users (⩽10 h/w) for the discomforts of fatigue and ache or pain associated with wearing lead aprons and also for the discomfort of ache or pain associated with wearing thyroid collars. No significant absolute differences could be seen between the sexes nor between age groups for the investigated discomforts.
Table 2. The respondents' experience of discomforts (bothersome warmth, fatigue, ache or pain) associated with wearing lead aprons and thyroid collars. The table includes significant absolute differences between frequent user (>10 h/w) and infrequent users (⩽10 h/w) and also between nurses and physicians for those discomforts where it could be found.
| Lead aprons | |||
|---|---|---|---|
| n | Proportion (%) (95% CI) | ||
| Bothersome warmth | All users (242) | 123 | 50.8 (44.5–57.1) |
| Nurses (121) | 70 | 57.9 (49.1–66.6) | |
| Physicians (121) | 53 | 43.8 (35.0–52.6) | |
| Absolute difference (Nurses−Physicians) | — | 14.0 (1.6–26.5) | |
| Fatigue | All users (241) | 86 | 35.7 (29.6–41.7) |
| Frequent users (35) | 21 | 60.0 (43.8–76.2) | |
| Infrequent users (206) | 65 | 31.6 (25.2–37.9) | |
| Absolute difference (Frequent−Infrequent) | — | 28.4 (11.0–45.9) | |
| Ache or pain | All users (239) | 62 | 25.9 (20.4–31.5) |
| Frequent users (35) | 18 | 51.4 (34.9–68.0) | |
| Infrequent users (204) | 44 | 21.6 (15.9–27.2) | |
| Absolute difference (Frequent−Infrequent) | — | 29.9 (12.4–47.4) | |
| Thyroid collars | |||
| n | Proportion (%) (95% CI) | ||
| Bothersome warmth | All users (227) | 71 | 31.3 (25.2–37.3) |
| Nurses (118) | 45 | 38.1 (29.4–46.9) | |
| Physicians (109) | 26 | 23.9 (15.9–31.9) | |
| Absolute difference (Nurses-Physicians) | — | 14.3 (2.4–26.1) | |
| Fatigue | All users (228) | 30 | 13.2 (8.8–17.5) |
| Ache or pain | All users (225) | 15 | 6.7 (3.4–9.9) |
| Frequent users (33) | 8 | 24.2 (9.6–38.9) | |
| Infrequent users (192) | 7 | 3.6 (1.0–6.3) | |
| Absolute difference (Frequent-Infrequent) | — | 20.6 (5.7–35.5) | |
To avoid wearing lead aprons and thyroid collars, the respondents' willingness to tolerate personal dose equivalent and their willingness to tolerate an increase in future cancer risk are presented in figures 1 and 2 as cumulative ratios. One third of the respondents would tolerate a personal dose equivalent of 1 mSv per year to avoid wearing lead aprons, but only a fifth would tolerate the corresponding increase in future cancer risk (from 43% to 43.2%). Around three quarters of the respondents would continue to wear their lead aprons instead of tolerating an increase in future cancer risk from 43% to 43.002%. A Wilcoxon signed-rank test showed that for lead aprons the respondents tolerated a higher personal dose equivalent compared to the corresponding increase in future cancer risk (p < 0.001).

Figure 1. The respondents' willingness to tolerate personal dose equivalent and increase in future cancer risk to avoid wearing lead aprons are presented as cumulative ratios. Error bars represent 95% CI of proportions.
Download figure:
Standard image High-resolution image
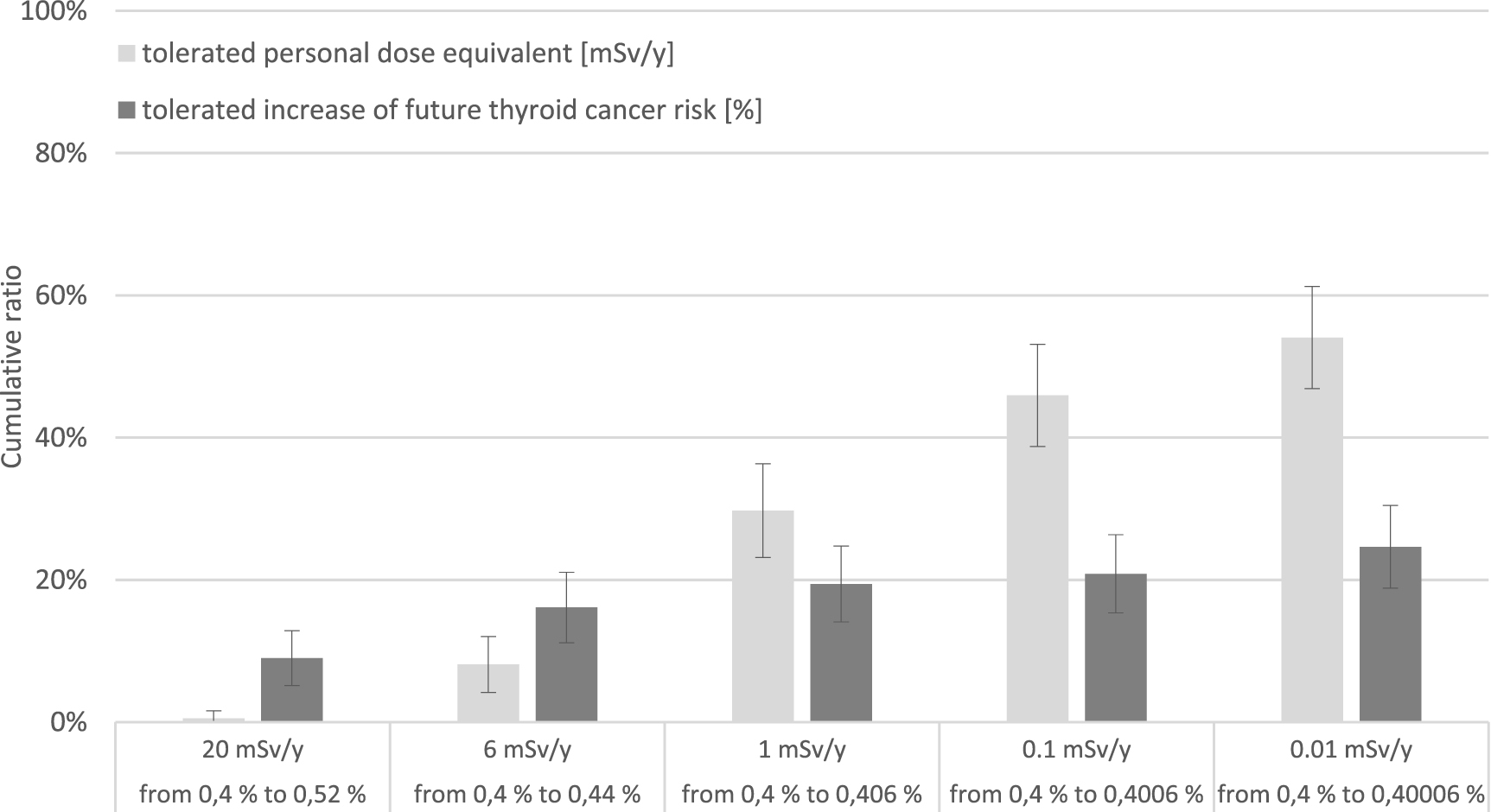
Figure 2. The respondents' willingness to tolerate personal dose equivalent and increase in future thyroid cancer risk to avoid wearing thyroid collars are presented as cumulative ratios. Error bars represent 95% CI of proportions.
Download figure:
Standard image High-resolution imageAs can be seen in table 2, discomforts associated with wearing thyroid collars were less common compared to wearing lead aprons. However, 90% of the respondents tolerated the same exposure of personal dose equivalent to avoid wearing thyroid collars as they did to avoid wearing lead aprons. Despite differences in risks between tolerating an increase in future cancer risk to avoid wearing lead aprons and tolerating an increase in future thyroid cancer risk to avoid wearing thyroid collars, the respondents' answers have similar distributions.
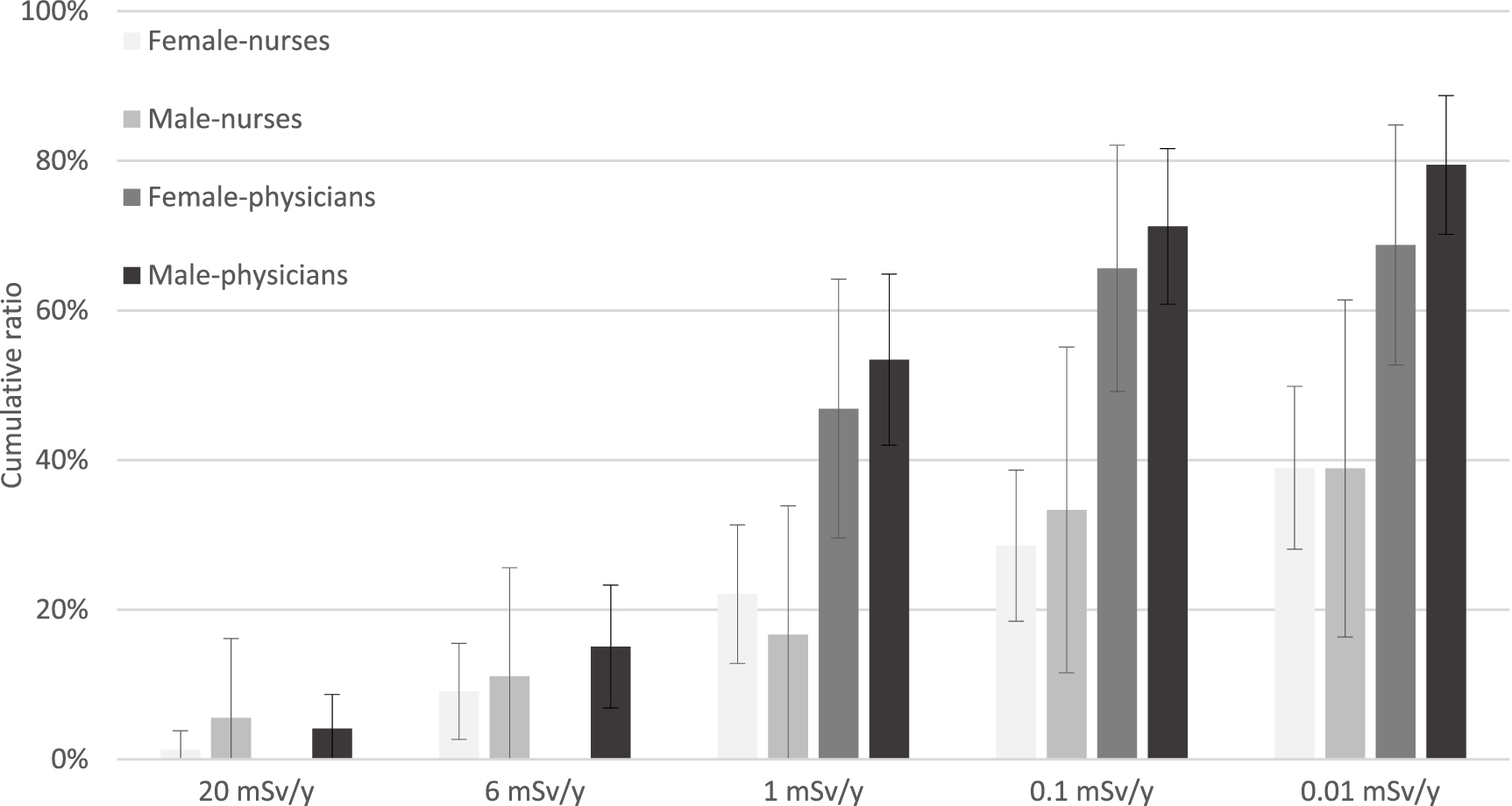
For the respondents' willingness to tolerate personal dose equivalent to avoid wearing lead aprons significant differences could be seen between occupations and between sexes (Mann–Whitney U tests). However, an ordinal regression analysis showed a significant association only for the occupation variable (p < 0.001) but not for the sex variable. Figure 3 shows the respondents' willingness to tolerate personal dose equivalent to avoid wearing lead aprons as cumulative ratios. In a stratified analysis the respondents were divided into four categories (female-nurses, male-nurses, female-physicians, male-physicians). Radiographers and assistant nurses were included in the group of nurses. Significant differences (Mann–Whitney U test) could be seen between male-physicians and male-nurses (p = 0.003) and between female-physicians and female-nurses (p = 0.007).

Figure 3. The respondents' willingness to tolerate personal dose equivalent to avoid wearing lead aprons, divided into four categories (female-nurses, male-nurses, female-physicians, male-physicians). Error bars represent 95% CI of proportions.
Download figure:
Standard image High-resolution imageFor the four categories of respondents, figure 4 shows differences in cumulative ratios of their willingness to tolerate an increase in future cancer risk to avoid wearing lead aprons. A significant difference (Mann–Whitney U test) was found between female-physicians and female-nurses (p < 0.001). For thyroid collars a similar pattern could be seen as for lead aprons in figures 3 and 4.

{kind=link}
{kind=link}
{kind=link}
Figure 4. The respondents' willingness to tolerate an increase in future cancer risk to avoid wearing lead aprons, divided into four categories (female-nurses, male-nurses, female-physicians, male-physicians). Error bars represent 95% CI of proportions.
Download figure:
Standard image High-resolution image{kind=link}
No significant differences could be seen between age groups nor between frequent users (>10 h/w) and infrequent users (⩽10 h/w) of lead aprons in their willingness to tolerate personal dose equivalent or their willingness to tolerate an increase in future cancer risk to avoid wearing lead aprons or thyroid collars. In the same way, no significant differences were found between respondents who experience some sort of discomfort (bothersome warmth, fatigue, ache or pain) associated with wearing lead aprons or thyroid collars compared to those who are not.
In a close-ended question, 72% of the respondents answered that rules regarding the use of lead aprons and thyroid collars should be decided by the Swedish Radiation Safety Authority, 23% answered that it should be up to the employees themselves to decide if they want to wear these protective tools and 5% did not to take a position in the question.
4. Discussion
In order to promote stakeholder involvement, the aim of the present study was to investigate staff's experience of discomforts associated with wearing lead aprons and thyroid collars for long periods of time, and also to investigate staff's willingness to tolerate personal dose equivalent (expressed as radiation dose) and the corresponding increase in future cancer risk to avoid wearing these protective tools.
The results from the 245 respondents at Skaraborg Hospital in Sweden showed that 51% experienced bothersome warmth, 36% experienced fatigue and 26% experienced ache or pain that they believed was associated with wearing lead aprons. Discomforts associated with wearing thyroid collars were also present. One third of the respondents would tolerate a personal dose equivalent of 1 mSv per year to avoid wearing lead aprons, but only a fifth would tolerate the corresponding increase in future cancer risk (from 43% to 43.2%). The respondents' answers for thyroid collars had a similar distribution.
Publications in table 3 shows a growing body of evidence between pain and working with lead aprons for long periods of time. In the present study, 80% of frequent users of lead aprons (>10 h/w) reported on former or present ache or pain in their neck, shoulders or back, compared to 59% for infrequent users, an absolute difference of 21 percentage points (95% CI 5.8–35.6 percentage points). In comparison, Moore et al [11] reported on back pain for 52% of frequent users of lead aprons (>10 h/w), compared to 46% for infrequent users, an absolute difference of 6 percentage points.
Table 3. Publications reporting on the link between pain and working with lead aprons for long periods of time.
| Publication (year) | Number of respondents | Results | Absolute differences (percentage points) |
|---|---|---|---|
| Moore et al [11] (1992) | 179 | 'Back pain was reported by 52% of those who estimated their lead apron use at greater than or equal to 10 h per week, the mean response, as opposed to 46% of those who wore lead aprons fewer than 10 h a week. These and related results were not statistically significant.' | 6 |
| Ross et al [12] (1997) | 714 | 'Cardiologists also received more specific therapies (primarily nonsteroidal anti-inflammatory drugs and mechanical support devices) than other physician groups, 52.7% versus 40.5% of orthopaedic surgeons and 31.8% of rheumatologists (p < 0.0001).' | 12 |
| Birnie et al [13] (2011) | 94 | 'There was a significantly higher prevalence of cervical spondylosis among electrophysiologists compared to matched noninterventional cardiologists (20.7% compared to 5.5%, P = 0.033).' | 15 |
| Orme et al [14] (2015) | 1 541 | 'Clinical employees with occupational exposure to procedures involving radiation requiring lead apron use reported experiencing work-related pain more often than the control group (54.7% vs. 44.7%; p < 0.001).' | 10 |
| Andreassi et al [15] (2016) | 746 | Exposed workers had a significantly higher prevalence of orthopaedic illness (30.2%) when compared with unexposed subjects (5.4%) p < 0.001. | 25 |
| Andrew et al [16] (2021) | 121 | 'This study has shown that back pain is more prevalent among staff who regularly used lead aprons (63%) compared to staff who do not (32%).' | 31 |
| Jiang et al [17] (2022) | 1 044 | The interventional cardiologists had significantly higher incidence of body pain (56.6% vs. 24.2%, p < 0.001) than the matched non-interventional cardiologists. | 32 |
| The present study (2023) | 245 | For frequent users of lead aprons (>10 h/w), 80.0% (95% CI 74.9–85.1%) reported on former or present ache or pain in their neck, shoulders or back. The corresponding proportion for infrequent users (⩽10 h/w) was 59.3% (95% CI 53.1–65.5%). The absolute difference between these groups was calculated to be 20.7 percentage points (95% CI 5.8–35.6). | 21 |
Considering both the reported link between pain and working with lead aprons for long periods of time in table 3 and the reported decrease in occupational radiation exposure during the last century [2, 21, 22] it may be time to raise the question: how safe is safe enough? Several studies in risk management argue that it is impossible to answer this question with a specific universal number [52–55]. Cost-benefit analysis shows that targeting a specific risk-level can lead to disproportionately high costs for society [52]. A negligible risk for an individual, for example 10−6 fatalities per year, can be regarded as serious if 100 million are exposed, that is, the theoretical deaths of 100 people per year [54]. Perception of risk is individual and regardless of the risk-level chosen to be negligible some would disagree with the alternative chosen [52].
Despite the arguments against expressing negligible risks with a specific number several authorities around the world has used this concept [56, 57]. Examples of broadly acceptable risk-levels has been expressed from 10−5 to 10−8 fatalities per year for the public and from 10−4 to 10−6 fatalities per year for workers [57]. In 1993 the National Council on Radiation Protection and Measurements considered a dose level of 0.01 mSv per year to be negligible, estimated to correspond to a risk of fatal cancer of 10−7 per year [58]. ICRP considers the dose level of 0.01 mSv per year to be of no concern (exempted from regulatory requirements) if the source is used in a justified practice [59].
An important distinguishment should be made between negligible and tolerable risks. A tolerable risk is a risk that stakeholders are prepared to live with to secure a certain benefit [60]. Optimisation is a balance between costs and benefits [61], and when it comes to stop wearing lead aprons, the cost is a small increase in future cancer risk and the benefit is the avoidance of discomforts associated with wearing them.
Several studies have shown that males are often more risk-taking compared to females [62–64], a study by Olofsson and Rashid [65] have shown the opposite result. In the present study, no significant difference in risk-taking between the sexes could be seen. On the other hand, in the present study physicians significantly tolerated more personal dose equivalent to avoid wearing lead aprons and thyroid collars compared to nurses. Cross [66] concluded that one of the errors in public perception of risk originates from poor knowledge in statistics and probability. The difference in risk-taking between physicians and nurses reported in the present study could possibly be explained from differences in education within this field.
Loewenstein et al [67] concluded that people interpret risks at two levels, they think about it cognitively and they react to it emotionally. Emotions such as fear, dread, and anxiety are spontaneous, not cortically mediated. These emotions are sensitive to the vividness of mental images associated with the risk [67], but very little to variations in the probability of the risk, often referred to as 'the affect heuristic' [67, 68]. Rottenstreich and Hsee [69] have shown that people are quite indifferent of how much they are willing to pay to avoid a 1% risk versus a 99% risk of receiving a painful but harmless electric shock. In decision making under risk, cognitively and emotionally levels often diverge from each other, and when they do emotional levels often drive the behaviour. When a risk is estimated to be above zero it becomes a source of worry, and variations in the smallness of the risk has little emotional impact [67]. In conclusion, people's perceptions on risk is much more than just a number [70].
When experts work cognitively with riskiness they tend to focus on technical terms such as annual fatalities and therefore their conclusions sometimes differ from the public, which are more driven from spontaneous emotions [71, 72]. People also tend to interpret information in a way that preserve their beliefs. When information is confirming it is often given too much confidence and when it is conflicting it is often dismissed as unreliable [73]. To some frustration for the experts, information about risk statistics has little effect on persuading people regarding their beliefs about riskiness. Therefore, risk management are destined to fail if it does not include the opinions of stakeholders [71, 72], a position also taken by the ICRP [29]. For example, Rasmussen et al [64] reported that 58% of the respondents in a survey expressed fairly or very strongly worries about radiation levels that have been declared harmless by authorities.
It has been pointed out that anaesthesia personnel sometimes wear lead aprons during producers where their exposure without is estimated to be just a few micro-sievert [33–36]. Huda and Boutcher [38] concluded that technologists working in nuclear medicine can choose their own strategy when it comes to the decision of wearing lead aprons. However, in the present study three quarters of the respondents wanted the Swedish Radiation Safety Authority to set rules regarding the use of lead aprons as opposed to individuals deciding for themselves. Authorities need research to lean on when setting rules and recommendations. In the present study, researchers hoped that the opinion of the stakeholders (the staff) would help to conclude on the topic. If so, it would have been beneficial if a broad majority of the stakeholders would have tolerated a certain limit of personal dose equivalent or a certain limit of increase in future cancer risk to avoid wearing lead aprons and thyroid collars for long periods of time.
The average difference in natural background radiation (excluding indoor radon) between Denver and Orlando is around 0.7 mSv per year [74]. ICRP has concluded that natural background radiation makes a small contribution to the overall health issues in societies and that dose levels corresponding to variations in natural background radiation could hardly be seen as unacceptable [75]. In this perspective, ICRP recommended the dose limit for the public to be set at 1 mSv per year [27, 75]. Considering variations in natural background radiation together with the discomforts of wearing lead aprons and thyroid collars for long periods of time, it might be reasonable to make it voluntary for staff exposed to less than 1 mSv per year to wear them. If so, the present study shows that only a third of the staff would probably stop wearing them.
There are several limitations of the present study. For example, the proportions of discomforts associated with wearing lead aprons and thyroid collars have been investigated but not the severity of the discomforts. Items about how much radiation dose per year the respondents are willing to tolerate to avoid wearing lead aprons and thyroid collars are in some ways problematic. As an aid the respondents were given information about the natural background radiation. However, a few respondents expressed that they did not know how dangerous the background radiation is and could therefore not answer the question. There are uncertainties in the link presented between personal dose equivalent and future cancer risk in the present study. In table 1, a 90% uncertainty interval was given based on both statistical and subjective components by the RadRAT program [51]. However, there are also inhomogeneities in the exposure of the staff, and the staff is also often moving around in an operating room, and there are uncertainties in measuring personal dose equivalent with a personal dosimeter. Together, these conditions will increase the uncertainties in the link between personal dose equivalent and future cancer risk even further. Finally, the questionnaire was handed out to the staff right before their periodically radiation safety education. The results of the present study might have been different if the questionnaire instead would have been handed out to them after the radiation safety education.
5. Conclusion
For staff exposed to ionizing radiation at Skaraborg Hospital in Sweden, 51% experienced bothersome warmth, 36% experienced fatigue and 26% experienced ache or pain associated with wearing lead aprons. Discomforts associated with wearing thyroid collars were also present. One third of the staff would tolerate a personal dose equivalent of 1 mSv per year to avoid wearing lead aprons, but only a fifth would tolerate the corresponding increase in future cancer risk (from 43% to 43.2%). The staffs' answers for thyroid collars had a similar distribution. The results show that discomforts associated with wearing lead aprons and thyroid collars for long periods of time are common, and at the same time only a minority of the staff would tolerate a small increase in future cancer risk to avoid wearing them. The present study gives an example of stakeholder involvement and points at the difficulties in making reasonable decisions about the use of these protective tools.
Acknowledgments
The authors declare no conflicts of interest. The present study was funded by the Research Fund at Skaraborg Hospital (VGSKAS-967871) and The Local Research and Development Council Skaraborg (VGFOUSKB-970108
Data availability statement
All data that support the findings of this study are included within the article (and any supplementary files).