
Abstract
We developed a novel method for tracking myocardial deformation using cardiac magnetic resonance (CMR) cine imaging. We hypothesised that circumferential strain using deformation-tracking has comparable diagnostic performance to a validated method (Displacement Encoding with Stimulated Echoes- DENSE) and potentially diagnostically superior to an established cine-strain method (feature-tracking). 81 healthy adults (44.6 ± 17.7 years old, 47% male), without any history of cardiovascular disease, underwent CMR at 1.5 T including cine, DENSE, and late gadolinium enhancement in subjects >45 years. Acquisitions were divided into 6 segments, and global and segmental peak circumferential strain were derived and analysed by age and sex. Peak circumferential strain differed between the 3 groups (DENSE: −19.4 ± 4.8%; deformation-tracking: −16.8 ± 2.4%; feature-tracking: −28.7 ± 4.8%) (ANOVA with Tukey post-hoc, F-value 279.93, p < 0.01). DENSE and deformation-tracking had better reproducibility than feature-tracking. Intra-class correlation co-efficient was >0.90. Larger magnitudes of strain were detected in women using deformation-tracking and DENSE, but not feature-tracking. Compared with a reference method (DENSE), deformation-tracking using cine imaging has similar diagnostic performance for circumferential strain assessment in healthy individuals. Deformation-tracking could potentially obviate the need for bespoke strain sequences, reducing scanning time and is more reproducible than feature-tracking.
Similar content being viewed by others


Introduction
The standard method for describing left ventricular (LV) pump function, the LV ejection fraction (LVEF), is based on the displacement of the endocardial borders during the cardiac cycle, and myocardial contractility is not directly assessed. Although echocardiography is the widely-used standard of care for imaging cardiac structure and function, cardiovascular magnetic resonance (CMR) has superior signal-to-noise ratio and endocardial border definition, and superior reproducibility1. In addition, echocardiography is limited by acoustic shadows and body habitus. LVEF derived by echocardiography is user-dependent and potentially imprecise2,3,4.
Myocardial strain is defined as the deformation of an object relative to its original length. Strain reflects myocardial deformation and is more closely linked with myocyte metabolism and contractility than LVEF5. Fibre shortening is reflected by a negative value for circumferential and longitudinal strain, whereas radial strain is positive, since LV thickening occurs with contraction. Strain can be estimated with echocardiography, cardiac magnetic resonance imaging or computed tomography (CT)6, and described globally or segmented for myocardial regions. A validated method for estimation of myocardial strain involves displacement encoding with stimulated echoes (DENSE). This technique has been validated using phantoms7,8,9, and myocardial tagging10,11,12,13,14.
Feature-tracking is a technique which derives strain from routinely acquired cine sequences, avoiding additional breath-hold imaging acquisitions that would be required with a bespoke strain method, such as DENSE, therefore shortening the duration of the CMR examination. Strain is derived by tracking features of interest along the endo- and epi-cardial borders as well as from columns of pixels radiating out from the endocardium15. Feature-tracking derived strain has been described as having larger magnitudes when compared to strain derived from reference methods, such as myocardial tagging, in healthy volunteers16, and in patients with cardiovascular disorders17,18,19. Displacement at the tissue-blood pool interface may be subtly greater than within the myocardial tissue, and this discrepancy may explain the potential inaccuracy of feature-tracking20.
Biomathematicians in our group (H.G., X.L.) have developed a method of estimating myocardial strain designed to overcome some of the theoretical limitations of feature-tracking, which uses local features, by estimating pixel-wise strain for myocardial deformation incorporating both local and global myocardial features from cine images. Deformation-tracking21 is based on an in-house intensity-based b-spline deformable registration method22. Our prelimary study21 and other studies23,24 have demonstrated that deformable image registration methods could be an alternative way to quantify regional LV deformation.
Circumferential strain (Ecc) is a key function inherent in myocardial contractility. The aim of our study was to compare two different cine-strain methods with a reference method of strain (DENSE). Since deformation-tracking derives strain from the entire myocardial region of interest, we hypothesised that circumferential strain derived with this method, would match strain derived from DENSE more closely than strain derived using feature-traking software. To this end, we enrolled a reasonably large group of healthy volunteers across a broad age range with no upper limit.
Results
Characteristics of the Study Participants
89 subjects underwent cardiac MRI at 1.5 T. Of these, 81 patients had short-axis views acquired with DENSE. The characteristics of these participants (n = 81) and their LV mass and function are presented in Table 1.
Quality Assessment
Image quality was higher for the cine scans than the DENSE acquisitions (Table 2). DENSE and deformation-tracking had better reproducibility than feature-tracking, (Table 3), and the intra-class correlation co-efficient was >0.90 for all analyses. Feature-tracking derived strain had larger standard deviations and wider limits of agreement.
The mean time (standard deviation) taken to analyse a short-axis slice was 105 ± 11 s for deformation-tracking, 53 ± 1 s for DENSE, and 76 ± 1 s for feature-tracking (ANOVA p < 0.009).
Strain results
Peak circumferential strain was lower with tissue deformation-tracking than with DENSE (deformation-tracking: −16.8 ± 2.4%, variance 4.7, DENSE: −19.4 ± 4.8%, variance 6.4). Feature-tracking derived strain was higher in magnitude than with the other two methods (−28.7 ± 4.8%, variance 23.2). Peak strain differed between the three methods (ANOVA with Tukey post-hoc, F-value 279.93, p < 0.01) (Fig. 1). Regional differences in strain were also observed with all three methods. Segmental data with feature-tracking had higher standard deviations when compared against DENSE and deformation-tracking (Table 4).

Peak circumferential strain assessed in 81 healthy volunteers using deformation-tracking, feature tracking and DENSE.
Outliers are depicted by circles.
Sex differences in LV strain
Global circumferential strains were greater in magnitude in women than in men with all three methods (Table 4) though the differences were not detected to be significantly different with feature-tracking, reflecting a consistent sex-related difference in strain.
Age differences in LV strain
There was no correlation between age and strain as revealed by DENSE (Pearson coefficient = 0.45, p = 0.70); Weak correlations were revealed by deformation-tracking (Pearson coefficient = 0.249, p = 0.025) and feature-tracking (Pearson coefficient = 0.379, p < 0.01). There was no difference in peak circumferential strain with age with DENSE and with deformation-tracking, after accounting for sex in a multivariate regression model. Using feature-tracking, there was a significant relationship with age, but not sex (Table 5).
Discussion
We have assessed the diagnostic performance of a novel deformation-tracking method for the assessment of circumferential strain across the full thickness of the myocardium. The method differs from feature-tracking which is mainly restricted to strain estimation from border deformation. We assessed both methods in a group of healthy volunteers with a broad age range and reasonably balanced sex distribution, and compared the strain values from these methods against strain data derived from a reference method (DENSE). Both deformation-tracking and feature-tracking enable strain estimation from standard cine scans.
We found that the shortest analysis time was with DENSE, and the longest time was with deformation-tracking, but overall the analysis times were broadly similar (<1.5 minutes) for all 3 methods. In a small group of patients with acute myocardial infarction, feature-tracking strain analysis was shown to be more reproducible than tagging analysis with a shorter analysis time17.
The peak circumferential strain derived from tissue deformation-tracking was lower than DENSE, whereas peak strain was higher with feature-tracking. Our results are consistent with those from previous studies16,17,18, in which feature-tracking over-estimated systolic strain when compared with reference data derived from myocardial tagging which is a dedicated strain imaging technique (Fig. 2, Table 4). On the other hand, some studies have reported similar circumferential strain values between feature-tracking and tagging in patients with Duchenne’s muscular dystrophy19, and in patients with acute myocardial infarction17 were both endo- and epicardial derived feature-tracking strains were averaged though the limits of agreement were wider than with tagging.

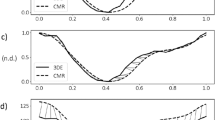
Cine-strain estimation with in-house developed tissue deformation-tracking software.
Schematic illustration of deforming a target image to a reference image using a b-spline deformable registration method. Myocardial strain is calculated from the estimated deformation fields. The similarity measurement is defined as the sum of squared differences in pixel intensity between the two images, the deformation transformation between the target and the reference images is modeled with uniform cubic b-splines.
Deformation-tracking identified a sex difference in strain as previously reported using DENSE25, i.e. that females may generate larger magnitudes of circumferential strain. In this study, feature-tracking derived strain revealed larger magnitudes of strain in females, which were not statistically significant. This result is in keeping with other studies using feature-tracking to look at healthy volunteers. Augustine16 (n = 145, 37% male) and Taylor26 (n = 100, 50% male) reported that circumferential strain was not associated with sex, whilst André27 (n = 150, 50% male) identified a statistically significant difference in circumferential strain between the sexes, with females having larger magnitudes of strain.
Due to sex-related association with peak strains as revealed by DENSE and deformation-tracking, we used a multivariate regression model to account for the influence of sex on strain, there was no association with age for DENSE and for deformation-tracking. Feature-tracking identified a relationship of strain with age. Whilst the best-fit regression line might be statistically significant, the spread (or variance) of the results is wider with feature-tracking than with deformation-tracking or DENSE, possibly due to the over-estimation of values by this technique, and the clinical significance of this result is uncertain. Looking to the literature, André27 using feature-tracking, Oxenham28 using tagging, and Neizel29 using strain-encoded CMR did not identify any association between age and strain. On the other hand Taylor26 reported an age related increase in circumferential strain, but no information was provided on the potential associations with sex.
There was marked heterogeneity in segmental values in feature-tracking and deformation-tracking, in keeping with that observed in studies with large numbers of healthy volunteers16. Segmental circumferential strain with feature-tracking had higher standard deviations than segmental strain acquired with DENSE or deformation-tracking, though segmental differences in healthy volunteers utilising feature-tracking strain have been previously described27.
There is controversy in the literature whether segmental feature-tracking derived strain is ready for clinical utility, as it has lower intra-class correlation co-efficients as compared to tagging, and because of high inter-study variability20,30. On the other hand studies have shown that segmental circumferential strain has utility in predicting segmental recovery post infarction31,32; as well as being correlated with infarct size17. Further, the analysis and interpretation of segmental strain data should account for repeated sampling, since strain within neighbouring segments is not independent.
A limitation of this study is that only mid-LV circumferential strain was assessed.
Tissue deformation-tracking performed well when compared with a reference method. The advantage of utilising a cine-strain derived method is that this would obviate the need for bespoke strain sequences being acquired, limiting the total duration of an CMR scan, and making strain more accessible in the clinical setting. Future research should assess whether deformation-tracking can accurately identify pathology such as infarct scar, and whether strain derived from deformation-tracking predicts prognosis.
Methods
Study Population
The UK Research Ethics Service (ethics reference 11/AL/0190) approved the study and all of the participants provided written informed consent. Healthy volunteers aged at least 18 years with no prior medical history (including cardiovascular health problems, medication or systemic illness) were invited to participate by placing advertisements in public buildings (e.g. hospital, university). The other exclusion criteria included standard contraindications to MR (e.g. metallic implants and metallic foreign body) and known or suspected pregnancy. A 12-lead electrocardiogram (ECG) was obtained in all subjects and a normal ECG was an eligibility requirement. Patient characteristics were recorded and body surface area was calculated with the Dubois formula.
MR Acquisition
Participants underwent CMR at 1.5 T (MAGNETOM Avanto, Siemens Healthcare, Erlangen, Germany) located in the Radiology Department of our hospital, using an anterior phased-array body coil (12-element) and a posterior phased-array spine coil (24-element). MR scanning was performed in line with current international guidelines33.
MR protocol
LV dimensions were assessed using balanced steady state free precession (b-SSFP) cinematographic breath-hold sequences. Typical imaging parameters are as shown in Table 6. The heart was imaged in multiple parallel short-axis planes 7-mm thick separated by 3-mm gaps, as well as in the 2-chamber, 3-chamber, and 4-chamber long-axis views.
A two-dimensional (2D) echo planar imaging (EPI) DENSE sequence (work-in-progress sequence 611, Siemens Healthcare, Erlangen, Germany) was used to acquire mid-ventricular short-axis and 4-chamber long-axis views. Typical imaging parameters are shown in Table 6. Through-plane dephasing and 2-point complementary spatial modulation of magnetization (CSPAMM) were used for artefact suppression during DENSE acquisition34. Fat suppression was carried out using a fast water excitation option provided by the vendor. The readout and phase-encoding direction of displacement were acquired in a single breath-hold.
Participants over 45 years of age had a blood chemistry test and if the estimated glomerular filtration rate (eGFR) was >30 mls/min/1.73 m2 gadolinium contrast was administered (0.15 mmol/kg per bolus of gadolinium diethyltriaminepenta -acetic acid (Gd-DTPA, Magnevist, Bayer Healthcare). Late gadolinium enhancement imaging covering the entire LV was performed 10–15 minutes after intravenous contrast agent administration using a segmented phase-sensitive inversion recovery (PSIR) turbo fast low-angle shot pulse sequence.
Image Analysis
Image analysis is as previously described25. The imaging datasets were anonymised to ensure that the imaging analysts were blinded to all other data. The strain data for each method were analysed separately in order to minimise observer bias. The data were co-ordinated by G.C. and C.H.
DENSE data were analysed using the CIM_DENSE2D software (University of Auckland, New Zealand)35 as previously described25. K.M and G.C. carried out DENSE image quality and artefact scoring and X.Z. acted as a blinded independent adjudicator when there was discordance. Cine image quality and artefact scoring was carried out by K.M. and C.M. and C.B. acted as a blinded independent adjudicator when there was discordance. The assessments involved using a Likert scale based scoring system developed by C.M.25.
Diogenes feature-tracking software (TomTec Imaging Systems, Germany) was used to quantify strain from cine images. The same operator (K.M.) derived strain following a standard protocol in line with the software manufacturer’s instructions16,19.
Deformation-tracking strain was calculated by the same operator (K.M.) using in-house developed code by H.G. in Matlab (Mathworks, Natick, US), in line with a standard, automated protocol that minimised variability and bias (H.G.)21. In the deformation-tracking approach21 (Fig. 2), an intensity-based b-spline deformable registration method22 was implemented to deform one target image into a reference image by minimizing the sum of squared differences of the two images, the deformation fields were represented by cubic b-spline basis functions, and further smoothed by introducing a regularized term in the minimization procedure. The deformation gradient F inside the LV wall was defined as  , u is the tracked deformation field inside the LV wall, X denotes the reference position of the LV wall. Finally the 2D myocardial strain tensor, defined as
, u is the tracked deformation field inside the LV wall, X denotes the reference position of the LV wall. Finally the 2D myocardial strain tensor, defined as  , was summarized for each segment, where I is the identity matrix. Details of deformation-tracking approach can be found in our preliminary study21.
, was summarized for each segment, where I is the identity matrix. Details of deformation-tracking approach can be found in our preliminary study21.
The results were saved as text files, and then the data were extracted using in-house code written in Matlab (Mathworks, Natick, US) by C.M. to minimize transcription errors.
The LGE images were reviewed by 2 experienced imaging cardiologists (D.C. and C.B.). The presence of LGE would imply sub-clinical or incidental cardiac disease such that the participant would then ineligible for continuing in the study.
Quality assessment
To minimise observer bias, 20 DENSE and 20 cine images were identified at random by G.C., and coded using a different code sequence to the main dataset. These 20 DENSE and 20 cine images were re-analysed 2 weeks later, by the same operator (K.M.) and by a 2nd expert operator (C.M. for DENSE, feature-tracking; H.G. for deformation-tracking). The time taken to analyse 20 data sets was measured for each of the operators and averaged. The study identifiers were released by G.C. once the analysis was carried out by K.M., C.M. and H.G.
Statistical Analysis
The statistical analyses were performed using SPSS software (SPSS Inc, Chicago, IL, USA, version 22). Normality was tested using the Shapiro-Wilk test. Continuous variables were expressed as mean ± standard deviation (SD). For comparison of two or more normally distributed variables, Student’s t-test and ANOVA with Tukey post-hoc analysis, or multivariate regression analysis were used. A p-value of <0.05 was considered statistically significant.
Additional Information
How to cite this article: Mangion, K. et al. A Novel Method for Estimating Myocardial Strain: Assessment of Deformation Tracking Against Reference Magnetic Resonance Methods in Healthy Volunteers. Sci. Rep. 6, 38774; doi: 10.1038/srep38774 (2016).
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
Epstein, F. H. MRI of left ventricular function. J. Nucl. Cardiol. Off. Publ. Am. Soc. Nucl. Cardiol. 14, 729–744 (2007).
Authors/Task Force Members et al. ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force on the management of ST-segment elevation acute myocardial infarction of the European Society of Cardiology (ESC). Eur. Heart J. 33, 2569–2619 (2012).
Bellenger, N. G. et al. Comparison of left ventricular ejection fraction and volumes in heart failure by echocardiography, radionuclide ventriculography and cardiovascular magnetic resonance; are they interchangeable? Eur. Heart J. 21, 1387–1396 (2000).
Popović, Z. B. The uncertainties of certainty: using LV function to predict arrhythmic event after AMI. JACC Cardiovasc. Imaging 6, 861–863 (2013).
Sengupta, P. P. & Narula, J. Cardiac Strain as a Universal Biomarker. JACC Cardiovasc. Imaging 7, 534–536 (2014).
Tee, M., Noble, J. A. & Bluemke, D. A. Imaging techniques for cardiac strain and deformation: comparison of echocardiography, cardiac magnetic resonance and cardiac computed tomography. Expert Rev. Cardiovasc. Ther. 11, 221–231 (2013).
Aletras, A. H., Ding, S., Balaban, R. S. & Wen, H. DENSE: Displacement Encoding with Stimulated Echoes in Cardiac Functional MRI. J. Magn. Reson. San Diego Calif 1997 137, 247–252 (1999).
Spottiswoode, B. S. et al. Motion-Guided Segmentation for Cine DENSE MRI. Med. Image Anal. 13, 105–115 (2009).
Young, A. A., Axel, L., Dougherty, L., Bogen, D. K. & Parenteau, C. S. Validation of tagging with MR imaging to estimate material deformation. Radiology 188, 101–108 (1993).
Young, A. A., Li, B., Kirton, R. S. & Cowan, B. R. Generalized spatiotemporal myocardial strain analysis for DENSE and SPAMM imaging. Magn. Reson. Med. 67, 1590–1599 (2012).
Kim, D., Gilson, W. D., Kramer, C. M. & Epstein, F. H. Myocardial tissue tracking with two-dimensional cine displacement-encoded MR imaging: development and initial evaluation. Radiology 230, 862–871 (2004).
Kim, D., Epstein, F. H., Gilson, W. D. & Axel, L. Increasing the signal-to-noise ratio in DENSE MRI by combining displacement-encoded echoes. Magn. Reson. Med. 52, 188–192 (2004).
Kar, J., Knutsen, A. K., Cupps, B. P. & Pasque, M. K. A Validation of Two-Dimensional In Vivo Regional Strain Computed from Displacement Encoding with Stimulated Echoes (DENSE), in Reference to Tagged Magnetic Resonance Imaging and Studies in Repeatability. Ann. Biomed. Eng. 42, 541–554 (2014).
Spottiswoode, B. S. et al. Tracking myocardial motion from cine DENSE images using spatiotemporal phase unwrapping and temporal fitting. IEEE Trans. Med. Imaging 26, 15–30 (2007).
Hor, K. N. et al. Magnetic Resonance Derived Myocardial Strain Assessment Using Feature Tracking. JoVE J. Vis. Exp. e2356–e2356, doi: 10.3791/2356 (2011).
Augustine, D. et al. Global and regional left ventricular myocardial deformation measures by magnetic resonance feature tracking in healthy volunteers: comparison with tagging and relevance of gender. J. Cardiovasc. Magn. Reson. 15, 8 (2013).
Khan, J. N. et al. Comparison of cardiovascular magnetic resonance feature tracking and tagging for the assessment of left ventricular systolic strain in acute myocardial infarction. Eur. J. Radiol. 84, 840–848 (2015).
Singh, A. et al. Intertechnique agreement and interstudy reproducibility of strain and diastolic strain rate at 1.5 and 3 tesla: A comparison of feature-tracking and tagging in patients with aortic stenosis. J. Magn. Reson. Imaging 41, 1129–1137 (2015).
Hor, K. N. et al. Comparison of Magnetic Resonance Feature Tracking for Strain Calculation With Harmonic Phase Imaging Analysis. JACC Cardiovasc. Imaging 3, 144–151 (2010).
Wu, L. et al. Feature tracking compared with tissue tagging measurements of segmental strain by cardiovascular magnetic resonance. J. Cardiovasc. Magn. Reson. 16, 10 (2014).
Gao, H., Allan, A., McComb, C., Luo, X. & Berry, C. Left ventricular strain and its pattern estimated from cine CMR and validation with DENSE. Phys. Med. Biol. 59, 3637 (2014).
Rueckert, D. et al. Nonrigid registration using free-form deformations: application to breast MR images. IEEE Trans. Med. Imaging 18, 712–721 (1999).
Phatak, N. S. et al. Strain measurement in the left ventricle during systole with deformable image registration. Med. Image Anal. 13, 354–361 (2009).
Veress, A. I., Gullberg, G. T. & Weiss, J. A. Measurement of strain in the left ventricle during diastole with cine-MRI and deformable image registration. J. Biomech. Eng. 127, 1195–1207 (2005).
Mangion, K. et al. Myocardial strain in healthy adults across a broad age range as revealed by cardiac magnetic resonance imaging at 1.5 and 3.0 T: Associations of myocardial strain with myocardial region, age, and sex. J. Magn. Reson. Imaging n/a–n/a, doi: 10.1002/jmri.25280 (2016).
Taylor, R. J. et al. Myocardial strain measurement with feature-tracking cardiovascular magnetic resonance: normal values. Eur Heart J Cardiovasc Imaging, doi: 10.1093/ehjci/jev006 (2015).
André, F. et al. Age- and gender-related normal left ventricular deformation assessed by cardiovascular magnetic resonance feature tracking. J. Cardiovasc. Magn. Reson. 17, 1–14 (2015).
Oxenham, H. C. et al. Age-related changes in myocardial relaxation using three-dimensional tagged magnetic resonance imaging. J. Cardiovasc. Magn. Reson. Off. J. Soc. Cardiovasc. Magn. Reson. 5, 421–430 (2003).
Neizel, M. et al. Strain-encoded (SENC) magnetic resonance imaging to evaluate regional heterogeneity of myocardial strain in healthy volunteers: Comparison with conventional tagging. J. Magn. Reson. Imaging JMRI 29, 99–105 (2009).
Morton, G. et al. Inter-study reproducibility of cardiovascular magnetic resonance myocardial feature tracking. J. Cardiovasc. Magn. Reson. 14, 43 (2012).
Buss, S. J. et al. Prediction of functional recovery by cardiac magnetic resonance feature tracking imaging in first time ST-elevation myocardial infarction. Comparison to infarct size and transmurality by late gadolinium enhancement. Int. J. Cardiol. 183, 162–170 (2015).
Khan, J. N. et al. Relationship of Myocardial Strain and Markers of Myocardial Injury to Predict Segmental Recovery After Acute ST-Segment–Elevation Myocardial Infarction. Circ. Cardiovasc. Imaging 9, e003457 (2016).
Kramer, C. M., Barkhausen, J., Flamm, S. D., Kim, R. J. & Nagel, E. Standardized cardiovascular magnetic resonance imaging (CMR) protocols, society for cardiovascular magnetic resonance: board of trustees task force on standardized protocols. J. Cardiovasc. Magn. Reson. 10, 35 (2008).
Zhong, X., Spottiswoode, B. S., Cowart, E. A., Gilson, W. D. & Epstein, F. H. Selective suppression of artifact-generating echoes in cine DENSE using through-plane dephasing. Magn. Reson. Med. 56, 1126–1131 (2006).
Young, A. A., Li, B., Kirton, R. S. & Cowan, B. R. Generalized spatiotemporal myocardial strain analysis for DENSE and SPAMM imaging. Magn. Reson. Med. 67, 1590–1599 (2012).
Acknowledgements
This research was supported by Project Grants from the Chief Scientist Office (SC01), Medical Research Scotland (343 FRG) and the British Heart Foundation (BHF-PG/14/64/31043). Dr Mangion is supported by a Fellowship from the British Heart Foundation (FS/15/54/31639). Dr. Gao is supported by funding from the EPSRC (EP/N014642/1). Professor Luo is supported by funding from the EPSRC (EP/N014642/1) and by a Leverhulme Research Fellowship (RF-2015-510). Professor Berry is supported by a Senior Clinical Fellowship from the Scottish Funding Council.
Author information
Authors and Affiliations
Contributions
K.M., C.M., C.B. made substantial contributions to conception and design. D.C., C.B., K.M. made substantial contributions to acquisition of data; K.M., C.H., C.M., H.G., X.Z., X.L., C.B. made substantial contributions to the analysis and interpretation of data; K.M., C.M., H.G., X.Z., C.H., C.B. drafted the article; All authors were involved in revising it critically for important intellectual content; All authors gave final approval of the version to be submitted.
Ethics declarations
Competing interests
X.Z. is an employee of Siemens. The University of Glasgow holds a research agreement with Siemens Healthcare, who provided the DENSE work-in-progress CMR sequence and data analysis software. The other authors declare no competing financial interests.
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Mangion, K., Gao, H., McComb, C. et al. A Novel Method for Estimating Myocardial Strain: Assessment of Deformation Tracking Against Reference Magnetic Resonance Methods in Healthy Volunteers. Sci Rep 6, 38774 (2016). https://doi.org/10.1038/srep38774
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep38774
This article is cited by
-
Sensitivity analysis and inverse uncertainty quantification for the left ventricular passive mechanics
Biomechanics and Modeling in Mechanobiology (2022)
-
Feature-tracking myocardial strain in healthy adults- a magnetic resonance study at 3.0 tesla
Scientific Reports (2019)
-
Detecting Methylomic Biomarkers of Pediatric Autism in the Peripheral Blood Leukocytes
Interdisciplinary Sciences: Computational Life Sciences (2019)
-
The feasibility of a novel limited field of view spiral cine DENSE sequence to assess myocardial strain in dilated cardiomyopathy
Magnetic Resonance Materials in Physics, Biology and Medicine (2019)
-
A Novel Hierarchical Template Matching Model for Cardiac Motion Estimation
Scientific Reports (2018)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
