
Abstract
Study design: Single case study.
Objectives: To evaluate the energy expenditure during ambulation with the Advanced Reciprocating Gait Orthosis (ARGO), with and without functional electrical stimulation (FES), and with the Parastep system in a single subject, in order to avoid the effect of inter-subject variability.
Setting: The Centre of Sport Medicine and Bioengineering Centre ‘Don C Gnocchi’ Foundation ONLUS IRCCS, Milano, Italy.
Methods: A single patient (lesion level T5–T6) was trained specifically for each walking system and was evaluated after each training period. The effects of FES on muscle conditioning, spasticity and bone density were also evaluated. The HR/V̇O2 relationship and the energy cost of locomotion were measured during wheelchair (WHCH) use, during locomotion with ARGO (with and without FES) and Parastep system at different speeds.
Results: The following was observed at the end of the whole training: (a) circumferences of both lower limbs and quadriceps forces were increased, whereas fatigue index was slightly decreased, spasticity and bone density were unchanged; (b) compared to WHCH locomotion, the slope of HR/VO2 curves with ARGO was higher (slope difference=51.1 b 1O2−1), with ARGO+FES was similar (slope difference=−5.3 b 1O2−1) and with Parastep was smaller (slope difference=−55.6 b 1O2−1); (c) HR increased linearly with all locomotion systems, but did not rise above 125 bpm with Parastep; (d) the cost of locomotion was higher with Parastep than with ARGO (with and without FES), tested at each velocity; (e) Parastep appears to be easier to use for the subject.
Conclusions: (a) FES can improve ambulation with orthosis, but the cost of locomotion remains very high; (b) the Parastep assisted gait elicits a higher energy expenditure than other orthoses, probably due to the lower speed of locomotion and to the high isometric effort of the stimulated muscles.
Sponsorship: This work has been partially supported by the Italian Minister of Public Health (Ricerca Finalizzata IRCCS no ICS030.7/RF97.25).
Similar content being viewed by others

Introduction
Standing and walking inability in paraplegic subjects can cause several secondary effects, such as joint contractures, pressure sores, accelerated osteoporosis, edema, spasticity, urinary and intestinal stasis.1,2 Moreover, spinal cord injured patients usually develop a global cardiovascular deconditioning, which presumably leads to the increased cardiovascular risk observed in these patients.1,2 For these reasons, the possibility to restore gait in paraplegics has been studied for several years, leading to the development of different types of orthoses. The first devices proposed were the long leg braces. However, they were too heavy, cumbersome and poorly efficient.3,4 The introduction of the reciprocating orthoses increased paraplegic gait efficiency.5,6 These devices facilitate the hip extension during stance and the hip flexion during swing, through a cable linkage between the two hips. More recently, the reciprocating mechanical orthoses were combined with functional electrical stimulation (FES), in order to facilitate the leg propulsion phase of orthoses-assisted gait and to reduce the overall energy expenditure.7,8,9,10
Unfortunately, in spite of the rapid evolution of orthotic devices, their efficiency is very low when compared to normal gait11 and even to wheelchair ambulation.12,13 The walking speed is low and the mean walking distance remains short. The most important reason for that is presumably that orthotic-assisted gait requires a very high energy expenditure, leading patients to stop after a few minutes.13 This critically affects the patient compliance to orthosis use.
To date, many studies were performed in order to compare the energy requirements of the different types of orthosis for paraplegics deambulation9,13,14,15,16,17,18 However, one of the main problems in studying the energy cost of different orthotic devices is that the groups of paraplegic subjects considered in these studies are often numerically small, and include individuals with different lesion levels and/or cardiovascular fitness. Hence, the assessment of the energy cost of the assisted locomotion in spinal cord injury patients can elicit very high variability.
The aim of the present study was to compare the energy cost of locomotion and the cardio-respiratory response with three different orthotic systems within a single patient, specifically trained for each device, in order to reduce the effect of inter-subject variability, previously reported to be very high.19,20 To this aim, we evaluated the actual most widespread orthoses among paraplegics: the Advanced Reciprocating Gait Orthosis (ARGO), with and without FES, and the Parastep system.
Material and methods
Patient
A male paraplegic subject was enrolled (age 28 years, weight 66 kg, height 160 cm). The patient was characterised by a traumatic spinal cord injury from 2 years at T5–T6 level (ASIA impairment scale: A).21 He had no previous experience with orthosis and electrical stimulation. The subject matched the inclusion criteria proposed for the reciprocating hybrid orthosis and Parastep.5,6,22,23 The patient gave his written informed consent for the study.
Walking systems
The Advanced Reciprocating Gait Orthosis (ARGO)
Constructive principles and mechanical characteristics of the ARGO (Hugh Steeper Limited, London, UK, weight 6.9 kg) used in this study are reported elsewhere.24 No significant modifications were applied to the orthosis.
The functional neuromuscular stimulator
The stimulator (DEM, Torino, Italy, weight 0.6 kg) used with the ARGO was developed to combine FES with reciprocating orthoses. It is a four channel stimulator which allows the contemporary stimulation of the hip flexor muscles of one leg and of the hip extensor muscles of the controlateral leg during locomotion.9 The stimulation is activated manually by the subject by pushing a button on the handles of the walker. The FES parameters were: biphasic rectangular waves, 20 Hz frequency, 280 μs of pulse width and 160 mA of max current amplitude.
The Parastep system
The Parastep system (Sigmedics Inc., Northfield, IL, USA, Parastep+AFO=weight 1.3 kg),23 is the only FES ambulation system actually approved by FDA. The device is a six-channel stimulator, controlled by a microprocessor and powered by a battery. The FES parameters were: monophasic rectangular waves, 24 Hz current frequency, 150 μs pulse width and current amplitude that can be varied manually from 0 mA to 300 mA. In our case the electrodes were placed on quadriceps to sustain the knee, in order to reach and maintain the standing posture. They were also placed laterally at the knee, to produce a flexion withdrawal reflex of the leg, triggering the stepping action. Despite the suggestion of Graupe and Kohn,23 the electrodes were not applied on the gluteus maximus, because the patient, even with the high lesion level, was able to bear the body mass on the upper limb and to adequately control the trunk equilibrium. Moreover, the stimulation on the gluteus was quite uncomfortable for the subject, and a source of instability during gait. The patient was able to put the electrodes on the quadriceps and the peroneal nerve alone and to wear the whole system within 10 min, while he could not put the electrodes on the back without assistance.
The stimulation unit was connected to a standard aluminium frame walker that has push-button switches mounted on the handles, to allow the user to control the stand and sit functions, the step activation and the stimulation intensity.
During walking the subject wore a standard ankle-foot orthosis to increase ankle stability and to avoid foot drop.
Training program
The patient was recruited for a rehabilitation program aimed at restoration of walking with a hybrid system (ARGO combined with FES), and then with the Parastep system. The subject carried out a dedicated training for each walking system with a resting period of about 1 month between each other, in order to limit any inter-training influence.
Training for muscle conditioning
Before beginning the gait training, the patient was enrolled in a muscle strengthening program through the FES-WeR system.25 This system was designed and developed for quadriceps muscles' re-strength during movements of standing up–sitting down, induced by FES and supported by a mechanical device for weight relief. The training of muscle conditioning consisted of 3 to 4 sessions/week of 90 min, and lasted 30 sessions. By means of the FES-WeR, we managed to reach a good level of quadriceps strength and an optimal balance of the trunk. At the end of the training, the patient was able to perform the sit to stand movements and maintaining knee locking under FES.26
Training with ARGO and FES
After the muscle conditioning, the subject started using the ARGO (with and without FES). The training lasted 50 sessions and consisted of 2/3 sessions/week of 90 min, according to a protocol also adopted by other authors.27
After the training with the ARGO, the patient began the training with the Parastep system.
Training with the Parastep system
This rehabilitation program has been divided into three phases. The first phase, performed at the parallel bars, was dedicated to training the standing-up movement and maintaining the standing posture. This period has been useful to the patient to maintain a sufficient strength of the quadriceps and to carry out exercises for the trunk balance.
In the second phase, the patient began to walk with the Parastep into the parallel bars. At the end of this period, the subject was able to walk backwards and forwards inside the parallels for several times and to control the movements of the trunk and pelvis to facilitate the swing phase of the leg. When the patient was confident enough with the system, the third phase of the training began in which he walked out of the parallel bars.
The whole training with Parastep lasted 50 sessions and consisted of 2/3 sessions/week of 90 min, as also done by other authors.20
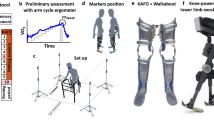
Measurements and data collection
Muscle training tests
The following measurements have been performed at the end of the training for muscle conditioning:
-
thigh circumference (cm) of both legs, measured at the distance of 15 cm from patellae with the legs extended;
-
maximum isometric knee torque (Nm), measured at 60° from the complete extension of the knee by means of a bench equipped with strain gauge;
-
fatigue index according to Kralj & Bajd,26 in order to verify the decrease of force during 30 s of continuous stimulation;
-
degree of spasticity, measured by means of the Computerised Pendulum, an experimental procedure previously described by Ferrarin et al;28
-
femoral bone density by means of a computerised mineralometry (HOLOGIC QDR 1000 WB, Hologic Inc.).
Energy consumption measurement
The energy consumption measurements have been performed in the following locomotion conditions:
-
1)
WHCH locomotion: (a) at rest; (b) during locomotion on a wheelchair-adapted rolling ergometer (Ergotronic 4000, Sopur, Germany) at two incremental speeds, for 7 min each speed, until muscular exhaustion;
-
2)
ARGO and ARGO+FES: (a) at rest, both sitting on a chair and standing with orthosis, (b) during orthosis-assisted ambulation, maintaining two different velocities chosen by the subject (self-selected speed and maximum speed) for at least 2 min:
-
3)
Parastep system: (a) at rest, both sitting on a chair and standing; (b) during Parastep assisted ambulation, maintaining the only possible speed for our patient for 4 min.
Both tests (2) and (3) have been performed at the end of the training for the specific locomotion system.
During the tests (1) and (2) the patient was allowed to rest for about 10 min between each test at different speeds.
The measured parameters were:
-
heart rate (HR, beats min−1) measured by a continuous electrocardiographic recording in V5 lead (Cardioline Delta 1 Plus, Italy);
-
pulmonary ventilation (V̇E, 1 min−1);
-
oxygen consumption (V̇O2, 1 min−1 and ml kg−1 min−1) measured by an open circuit standard method during the last minute of walking at each speed.
The calculated parameter was:
-
the metabolic cost of locomotion, ie the amount of oxygen required to cover 1 m distance;
-
the net cost of locomotion (C, ml kg−1 m−1), corresponding to the energy required to cover 1 m per unit of transported mass (body+WHCH or orthosis or Parastep).
Results
Training efficacy assessment
The thigh circumference increased from 42 to 44 cm after the training for muscular conditioning, and remained constant during the whole period of assisted gait.
The force values, expressed as maximum isometric knee torques, increased in both legs from 20 Nm at the beginning to 40 Nm at the end of the muscle conditioning training, and it was further doubled at the end of the training with all walking systems.
The fatigue index decreased from 30% at the beginning to 28% at the end of the muscle conditioning training, and it was reduced further to 22% at the end of the training with all walking systems.
Finally, according to the Pendulum Test results, the low initial level of spasticity (Relaxation Index=1.63, normal value⩾1.7) was found to be unchanged during the training period.
The average value between the two legs of the pre-training period of the bone mass density (BMD=0.69 gr cm−2) was just below the minimum level of the normative range (BMD between 0.75 and 1.1 gr cm−2), and remained constant after the training (BMD=0.70 gr cm−2).
Energy expenditure
The speed of orthosis assisted gait was much lower than the WHCH locomotion. The velocity of locomotion was comparable between ARGO and ARGO+FES, and was significantly faster than with the Parastep (Table 1). Moreover, the patient was able to walk at only one velocity with Parastep.
V̇O2 values were 0.36, 0.35 and 0.62 1 m−1 during orthosis standing and 0.79, 0.94 and 1.33 l m−1 during locomotion at the self-selected speed with ARGO, ARGO+FES and Parastep, respectively (Table 1). Figure 1 shows the aerobic energy expenditure per kg of body mass which occurs from sitting to standing and during locomotion with each walking system. V̇O2 was similar during the transition from sitting to standing with ARGO and ARGO+FES, whereas it increased dramatically with Parastep. V̇O2 value was higher during the locomotion with Parastep than with ARGO and ARGO+FES, at any speed.

V̇O2/BW for ARGO, ARGO+FES and Parastep in sitting and standing, during gait at self-selected speed and maximal speed. Note that with the Parastep the subject could walk at only one speed
HR increased linearly during ambulation with ARGO, ARGO+FES and Parastep. However, HR did not rise over 124 bpm during Parastep gait (Table 1). Figure 2 shows the effects of the assisted gait with each walking system on the heart rate, expressed as per cent of the maximal theoretical heart rate (computed as 220 – age). During gait at self selected speed, HR was 74, 56 and 65% for ARGO, ARGO+FES and Parastep respectively. Figure 3 shows the HR/V̇O2 relationship for all the locomotion systems: the r2 slope of each curve is reported in Table 2. The slope difference Δs1 HR/V̇O2 [bl−1] refers to the increase in heart beats for litre of O2 consumed when changing from WHCH to orthosis ambulation: the higher values were observed from the ARGO locomotion.

HR/HR max [%] for ARGO, ARGO+FES and Parastep in standing and during gait at self selected speed and maximal speed (only for mechanical orthosis). HR max was the maximal theoretical heart rate computed as 220−age

HR/V̇O2 relationship for each walking system is presented. Filled square, unfilled square and unfilled triangles correspond to ARGO, ARGO+FES and Parastep values respectively. The equations of the linear regression are reported in Table 2
Figure 4 shows the pulmonary ventilation. V̇E values were much higher in standing with Parastep than ARGO (with and without FES). Even during locomotion at self-selected speed V̇E was higher with Parastep than with ARGO and ARGO+FES.

V̇E for ARGO, ARGO+FES and Parastep in standing and during gait at self selected speed and maximal speed (only for mechanical orthosis) is presented
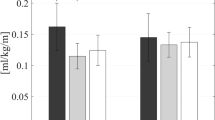
In Figure 5 the oxygen required by the subject to cover 1 m distance is presented. The value is higher for Parastep than for ARGO and ARGO+FES.

The cost of locomotion required to cover 1 m distance for WHCH and walking systems
Functional results
At the end of each training the patient was able to don and doff and to use each system without assistance. He was able to wear the Parastep in a shorter time than the reciprocating orthosis and to manually self-activate the stimulation for both systems. At the end of the training with ARGO, the patient was able to walk independently without rest for about 200 m both indoor and outdoor. On the other hand, he could walk for about 15 m, only indoor, using the Parastep system. According to his opinion, Parastep was less complicated to use; nevertheless, it was rather fatiguing. The results obtained with ARGO are in agreement with a previous study,29 whereas with the Parastep our patient walked slower as reported in another study.30
Discussion
Training efficacy and safety
The different training performed for the different systems, each including muscle conditioning and walking, were effective in our patient, as demonstrated by the induced morphometric variations in the circumference of the legs, by the positive results of the force tests and by the decreased fatigue index. In addition, spasticity was not affected by training, as can be argued by the results of the Computerised Pendulum Test. No significant changes were found in bone mineral density, in agreement with previous studies.31 Hence, it can be concluded that training procedures with FES were both effective and safe in our patient. The training did not produce adverse effects on the musculo-skeletal trophism and did not worsen spasticity. These results are in agreement with previous observations on the physiological effects of muscular training induced by FES in paraplegic patients.1,2,9,20,32
Energy expenditure during assisted walking
Standing
In a previous work33 in paraplegic subjects the muscular pump in lower limbs and the vasomotor control in the splanchnic area were shown to be impaired, thus leading to an inadequate venous return during exercise. Such impairment is overemphasized in standing posture because of the gravitational effect. The significant increase in HR found in standing, which counteracts the increased stroke volume, seems to confirm this observation.33 In addition, in the present study it was shown that the energy requirement during standing, in terms of V̇O2 consumption and V̇E, is higher with Parastep than with ARGO (with and without FES) (Figures 1 and 4). Indeed, during standing with ARGO (with and without FES), the patient did not make any muscle effort to maintain the standing posture, provided by the mechanical structure. On the contrary, standing with Parastep requires the continuous electrical stimulation of the quadriceps in order to lock the knee joint and the consistent contraction of upper limb muscles to maintain the equilibrium. This may account for the elevated V̇O2, V̇E, and HR increases during the transition from sitting to standing, observed only with Parastep (Table 1).
Assisted ambulation
During orthotic ambulation the gravitational effect decreases stroke volume and impairs blood redistribution to upper limbs, leading to early fatigability.33 Merati et al13 have demonstrated that, compared to WHCH ambulation, during orthosis locomotion the HR/V̇O2 slope increases, ie HR increase is higher at a given V̇O2 increase. On the contrary, HR/V̇O2 slope was similar between WHCH and orthosis with FES.13 Accordingly, the results of this study show that the addition of FES to ARGO decreased the HR/V̇O2 slope to the value found in WHCH locomotion, probably because it improved the venous return and hence the stroke volume.
In spite of observations during ARGO+FES assisted gait, where HR increased to 165 bpm (corresponding to 98% of the subject's theoretical maximal HR), during walking with Parastep HR did not rise over 124 bpm (65% of HR max). This value is lower than the value obtained by Brissot et al and Jacobs et al during FES assisted gait,34,35 probably due to an increased blood pressure during Parastep ambulation. Unfortunately, we could not measure blood pressure during Parastep gait, as in our experimental protocol such procedure would have been carried out only with an invasive approach, because of the high level of the isometric contraction in upper limbs. However, a linear increase in blood pressure associated with an increase in HR not beyond 127 bpm in paraplegics during isometric exercise induced by electrical stimulation was recently found by Petrofsky.36 We suggest that, whereas during ARGO+FES walking the muscular contractions were isotonic and intermittent, during the Parastep ambulation the contraction of quadriceps had a large isometric component and that the trunk and arm muscles were activated continuously and isometrically. The consequent baroreflex modulation of HR, whose anatomical pathways are almost completely preserved in a T5–T6 lesion, leads to a bradycardic response.
The influence of room temperature on HR can be ruled out, as all experiments were carried out at the same comfortable room temperature.
Cost of locomotion
In a previous study, FES was found to increase the cost of locomotion (C) at low and self-selected speed.13 The present results showed a similar behavior: a higher C value with ARGO+FES than with ARGO alone at low speed (v<0.8 Km h−1). Probably faster speeds with FES would result in lower energy expenditure, as a consequence of a lower amount of energy required by the stance.16 Moreover, a much higher C value (see Figure 5) was found with Parastep than with ARGO (with and without FES). This is clearly due to the high energy consumption required (see Figure 1) and the extremely low speed obtained (v=0.2 Km h−1). It can be argued that the addition of the electrodes on the gluteus maximus or on the low back muscles, not suitable in the considered patient despite the high lesional level, would improve gait performance by means of a better trunk control and a smaller involvement of upper limb muscles. This may suggest that the intolerability of FES on the lower back of a high level paraplegic subject, should be critically considered.
Conclusions
FES can improve ambulation with orthosis, as it facilitates the venous return and the stroke volume. Nevertheless, the energy expenditure of the assisted ambulation remains very high, even during the locomotion at the self-selected speed. In our subject, Parastep assisted gait was found to require a higher energy expenditure with respect to other orthoses (either with or without stimulation), in terms of oxygen consumption and cost of locomotion. This is probably due to the slower speed of locomotion the subject could achieve with this walking system, which determines a continuous effort of the stimulated muscles, and a large isometric contraction of the trunk and arm muscles to maintain the equilibrium of the body, in particular when back muscles of a high level lesion patient are not stimulated.
These results suggest that by improving the control efficiency of stimulation, in order to obtain a muscular recruitment more similar to the natural one, could lead to a smoother and faster gait where the isometric components would probably decrease. Since the Parastep system proved to be very comfortable to don and doff autonomously in a short time, very light to wear and less cumbersome to use indoors, further studies should be performed to investigate new algorithms (like neural networks and adaptive control rules) in order to improve the control strategies. Whether such a goal could be reached by surface or implanted electrodes remains an open question.
References
Glaser RM . Functional neuromuscolar stimulation. Exercise conditioning of spinal cord injured patients. Int J Sports Med 1994; 15: 142–148.
Solomonow M, Reisin E, Aguilar E, Baratta RV, Best R & D'Ambrosia R . Reciprocating gait orthosis powered with electrical muscle stimulation (RGO II). Part II: medical evaluation of 70 paraplegic patients. Orthopedics 1997; 20: 411–418.
Cerny K, Waters R, Hislop H & Perry J . Walking and wheelchair energetics in persons with paraplegia. Physical Therapy 1980; 60: 1133–1139.
Merkel KD, Miller NE, Westbrook PR & Merrit JL . Energy expenditure of paraplegic patients standing and walking with two knee-ankle-foot-orthoses. Arch Phys Med Rehabil 1984; 65: 121–124.
Beckman J . The Louisiana State University reciprocating gait orthosis. Physiotherapy 1987; 73: 386–392.
Butler PB & Major R . The ParaWalker. A rational approach to the provision of reciprocal ambulation for paraplegic patients. Physiotherapy 1987; 73: 393–397.
Marsolais EB, Kobetic R, Chizeck HJ & Jacobs JL . Orthoses and electrical stimulation for walking in complete paraplegia. J NeuroRehab 1991; 5: 13–22.
Mechanical orthoses FES for patient with complete thoracic lesionsIn: Pedotti A, Ferrarin M, Quintern J, Riener R (eds). Neuroprosthetics: from basic research to clinical applications. Berlin: Springer-Verlag, 1996;
Solomonow M, Baratta R, Hirokawa S, Rightor N, Walker W, Beaudette P, Shoji H & D'Ambrosia R . The RGO generation II: muscle stimulation powered orthosis as a practical walking system for thoracic paraplegics. Orthopedics 1989; 12: 1309–1315.
Pedotti A, Ferrarin M, Quintern J & Riener R. (eds). Neuroprosthetics: from basic research to clinical applications. Berlin: Springer Verlag. 1996.
Beillot J, Carré F, Le Claire G, Thoumie P, Perruoin-Verbe B, Cormerais A, Courtillon A, Tanguy E, Nadeau G, Rochocongar P & Dassonville J . Energy consumption of paraplegic locomotion using reciprocating gait orthosis. Eur J Appl Physiol 1996; 73: 376–381.
Lotta S, Fiocchi A, Giovannini R, Silvestrin R, Tesio L, Raschi A, Macchia L, Chiapatti V, Zambelli M, Tosi C, Baratta S & Franceschini M . Restoration of gait with orthoses in thoracic paraplegia: a multicentric investigation. Paraplegia 1994; 32: 608–615.
Merati G, Sarchi P, Ferrarin M, Pedotti A & Veicsteinas A . Paraplegic adaptation to assisted-walking: energy expenditure during wheelchair versus orthosis use. Spinal Cord 2000; 38: 37–44.
Patrick JH & McClelland MR . Low energy cost reciprocal walking for the adult paraplegic. Paraplegia 1985; 23: 113–117.
Isakov E, Douglas R & Berns P . Ambulation using the reciprocating gait orthosis and functional electrical stimulation. Paraplegia 1992; 30: 239–245.
Marsolais EB & Edwards BG . Energy cost of walking and standing with functional neuromuscular stimulation and long leg braces. Arch Phys Med Rehabil 1988; 69: 243–249.
Hirokawa S, Grimm M, Le Thanh, Solomonov M, Baratta RV, Shoji H & D'Ambrosia RD . Energy consumption in paraplegic ambulation using the Reciprocating Gait Orthosis and electric stimulation on the thigh muscles. Arch Phys Med Rehabil 1990; 71: 687–694.
Nene AV & Patrick JH . Energy cost of paraplegic locomotion with the ORLAU ParaWalker. Paraplegia 1989; 27: 5–18.
Winchester P, Carollo JJ & Habasevich MS . Physiologic costs of reciprocal gait in FES assisted walking. Paraplegia 1994; 32: 680–686.
Gallien P, Brissot R, Eyssette M, Tell L, Barat M, Wiart L & Petit H . Restoration of gait by functional electrical stimulation for spinal cord injured patients. Paraplegia 1995; 33: 660–664.
Ditunno JF, Young W, Donovan WH & Creasey G . The international standards booklet for neurological and functional classification of spinal cord injury. Paraplegia 1994; 32: 70–80.
Graupe D & Kohn KH . Transcutaneous functional neuromuscolar stimulation of certain traumatic complete thoracic paraplegics for independent short-distance ambulation. Neurological Res 1997; 19: 323–333.
Graupe D & Kohn KH (eds.)Functional electrical stimulation for ambulation by paraplegics–Twelve years of clinical observations and system studies. Malabar: Krieger Publishing Company 1994.
Lissene MA, Peeraer L, Goditiabois F & Lysens R . Advanced reciprocating gait orthosis in paraplegic patients. [abstract]. In: Zupko JK (ed). Proceedings of the 7th World Congress International Society for Prosthetics and Orthotics (ISPO), Chicago, 1992.
Ferrarin M, Pavan EE, Spadone R, Cardini R & Frigo C . Standing up exerciser based on functional electrical stimulation and body weight relief. Med Biol Eng Comp 2002; 40: 282–289.
Kralj A & Bajd T . (eds.) Functional electrical stimulation: standing and walking after spinal cord injury. Boca Raton: CRC Press Inc. 1989.
Thoumie P, Le Claire G, Beillot J, Dassonville J, Chevalier T, Perrouin-Verbe B, Bedoiseau M, Busnel M, Cormerais A, Courtillon A, Mathe JF, Moutet F, Nadeau G & Tanguy E . Restoration of gait in paraplegic patients with RGO-II hybrid orthosis. A multicenter controlled study. II: physiological evaluation. Paraplegia 1995; 33: 654–659.
Ferrarin M, Osio M & Abello G . A new mechanical approach to Pendulum Test for spasticity evaluation. In: Pedotti A, Ferrarin M, Quintern J and Riener R. (eds.). Neuroprosthetics: from basic research to clinical applications. Berlin: Springer-Verlag, 1996.
Solomonow M, Aguilar E, Reisin E, Baratta RV, Best R, Coetzee T & D'Ambrosia R . Reciprocating gait orthosis powered with electrical muscle stimulation (RGO II). Part I: performance evaluation of 70 paraplegic patients. Orthopedics 1997; 20: 315–324.
Klose KJ, Jacobs PL, Broton JG, Guest RS, Needham-Shropshire BM, Lebwohl N, Nash MS & Green BA . Evaluation of a training program for persons with SCI paraplegia using the Parastep® 1 ambulation system: part 1. Ambulation performance and anthropometric measures. Arch Phys Med Rehabil 1997; 78: 789–793.
Ogilvie C, Bowker P & Rowley DI . The physiological benefits of paraplegic orthotically aided walking. Paraplegia 1993; 31: 111–115.
Graupe D & Kohn KH . Functional neuromuscolar stimulator for short-distance ambulation by certain thoracic-level spinal-cord-injured paraplegics. Surg Neurol 1998; 50: 202–207.
Hopman MTE, Oeseburg B & Binkhorst RA . Cardiovascular responses in paraplegic subjects during arm exercise. Eur J Appl Physiol 1992; 65: 73–78.
Brissot R, Gallien P, Le Bot MP, Beaubras A, Laisné D, Beillot J & Dassonville J . Clinical experience with functional electrical stimulation-assisted gait with parastep in spinal cord-injured patients. Spine 2000; 25: 501–508.
Jacobs PL, Klose KJ, Guest R, Needham-Shropshire B, Broton JG & Green BA . Relationships of oxygen uptake, heart rate, and ratings of perceived exertion in persons with paraplegia during functional neuromuscolar stimulation assisted ambulation. Spinal Cord 1997; 35: 292–298.
Petrofsky JS . Blood pressure and heart rate response to isometric exercise: the effect of spinal cord injury in humans. Eur J Appl Physiol 2001; 85: 521–526.
Acknowledgements
The authors wish to thank the patient who participated in this study, for his collaboration, helpfulness and enthusiasm.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Spadone, R., Merati, G., Bertocchi, E. et al. Energy consumption of locomotion with orthosis versus Parastep-assisted gait: a single case study. Spinal Cord 41, 97–104 (2003). https://doi.org/10.1038/sj.sc.3101420
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.sc.3101420
Keywords
This article is cited by
-
The influence of orthosis options on walking parameters in spinal cord-injured patients: a literature review
Spinal Cord (2016)
-
The efficiency of orthotic interventions on energy consumption in paraplegic patients: a literature review
Spinal Cord (2015)
-
Benefits of FES gait in a spinal cord injured population
Spinal Cord (2007)
