
Abstract
Study design
Randomised controlled three-arm parallel clinical trial set in general dental practice.
Intervention
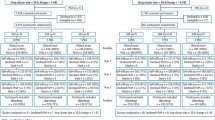
Three hundred and sixty-nine patients were recruited to the trial. To be included patients had to be regular attenders aged 18 to 60 years with 20 or more teeth and BPE codes <3 and DT<4. They were excluded if they wore an intra-oral applicance or had systemic conditions or used medication that could predispose to periodontal disease. Participants were randomised to have single-visit scale and polish at 6 month, 12 month or 24 month intervals and treatment was carried out by nine hygienists and therapists. Randomisation was performed centrally at a distant site by the trial manager and participants were not informed for their treatment allocation until they returned for their 6-month recall. Allocation was not explicitly revealed to the dentist, and participants were asked not to reveal their allocation group to the dentist or the outcome examiner.
Outcome measure
The primary outcome measure was presence of gingival bleeding. Secondary outcome measures were presence of plaque and presence and amount of calculus.
Results
Data were collected for 83.5% of the original participants and 76.2% attended all five appointments. There were no statistically significant differences in prevalence of gingival bleeding at follow-up for each group: 6-month recall group 78.5%; 12-month group 78% and 24-month group 82% (p=0.746). There were also no differences between groups at follow-up for prevalence of plaque and calculus.
Conclusions
This trial did not identify any differences in gingival health associated outcomes for single-visit scale and polish provided at 6-, 12- and 24-month frequencies for healthy patients. However, the results are not conclusive and larger trials with more comprehensive measurements are needed.
Similar content being viewed by others


Commentary
Jones et al. investigated one of the most common dental procedures provided to our patients, namely ‘Scale and Polish’ or ‘Oral Prophylaxis’. They highlighted that ‘in 2009/10, 12 million (44.1% of total) courses of treatment carried out on adult National Health Service (NHS) patients in England included a scale and polish’.1 It is commonly accepted that some of the most basic treatments that we provide as dental professionals lack a robust evidence base. To ensure the most effective use of resources it is important that the profession seeks to provide this evidence base in order to inform our patients and policy makers.
Since most dental treatment is provided in primary care, this pragmatic clinical trial was carried out in this setting. Jones et al. investigated three different Scale & Polish intervals for periodontally healthy patients (exclusion criteria BPE 3/4/*) over a period of 24 months. The results did not demonstrate any differences in outcomes (gingival bleeding, presence of plaque, presence and amount of calculus) for single-visit scale and polish provided at 6-, 12- and 24-month frequencies.
The authors note that only limited data had been available to inform their sample size calculation, and indeed ultimately they state that a larger trial over a longer period could have resulted in more conclusive results.
This trial demonstrates that research in primary dental care in the United Kingdom is feasible. No one randomised control trial can be expected to conclusively answer any research question for all patients. Combining the results of RCTs from different settings with similar participants in meta-analyses can provide more robust evidence that can inform patients, clinicians and policy-makers decisions. In addition, trials of effectiveness (observational and other designs) as well as trials looking at the efficacy of treatments such as this are needed to ensure that when the results are applied to day-to-day practice they do actually have success rates similar to those indicated by the trials.
The National Institute for Health Research Health Technology Assessment programme (NIHR HTA) are currently funding the Improving the Quality of Dentistry (IQuaD) trial in primary dental care in Scotland and the North East of England (http://www.hta.ac.uk/2300). IQuaD is comparing oral hygiene advice and periodontal instrumentation for the prevention and management of periodontal disease in dentate adults attending dental primary care.
These studies can aid the design of future trials in this setting, hopefully providing sufficient data to inform future sample size calculations.
References
The NHS Information Centre Dental and Eye Care Team: Clinical Dental Report, England and Wales: 2009/10 – Experimental Statistics. 2010, 1.0.
Author information
Authors and Affiliations
Additional information
Address for correspondence: Clare L Jones, School of Dentistry, The University of Manchester, Oxford Road, Manchester, M13 9PL, UK. E-mail: clare.jones-2@manchester.ac.uk
Jones CL, Milsom KM, Ratcliff P, Wyllie A, Macfarlane TV, Tickle M. Clinical outcomes of single-visit oral prophylaxis: a practice-based randomised controlled trial. BMC Oral Health 2011; 11: 35.
Rights and permissions
About this article
Cite this article
Lamont, T. No differences in gingival health associated outcomes following single-visit scale and polish. Evid Based Dent 13, 114 (2012). https://doi.org/10.1038/sj.ebd.6400897
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ebd.6400897
