
Abstract
Study design:
Three-dimensional kinematic analysis of car transfer (CT) movement in four adult males with C6 tetraplegia.
Objectives:
The aim of the present study was to assess the normal transfer technique movement from a wheelchair to a car (that is, CT) in subjects with tetraplegia. A better understanding of CT movement is invaluable knowledge for spinal cord injury rehabilitation. This type of knowledge will improve rehabilitation programs so that patients with tetraplegia will have greater societal participation.
Setting:
School of Comprehensive Rehabilitation, Osaka Prefecture University, Osaka, Japan.
Methods:
Four adult males with C6 tetraplegia, an impairment grade of A according to the American Spinal Injury Association guidelines, took part in the study. The subjects used their own wheelchair and car in our assessments of their CT movement technique. Movements were assessed using a three-dimensional video analysis system with six digital video cameras. CT data, which included lateral displacement of the head and buttocks, and angular displacement of neck flexion and trunk forward inclination, were collected and correlation coefficients were calculated.
Results:
All four subjects demonstrated negative correlations in lateral displacements greater than 0.70. As for correlation coefficients of angular displacement, two subjects demonstrated negative correlations (r=−0.98 and r=−0.77) and one subject demonstrated a positive correlation (r=0.75). The neck flexion and trunk forward inclination strategy was different among the four subjects.
Conclusions:
Each subject with C6 tetraplegia demonstrated different strategies during CT movement.
Similar content being viewed by others


Introduction
Transfer movement is one of the most important and meaningful skills of individuals with tetraplegia. This movement is widely performed in daily life and is an important prerequisite for acquisition of functional abilities. The ability to perform a transfer is also linked to societal participation. In particular, independence in transfer movement would encourage individuals with tetraplegia to participate more fully in the community through access to an automobile or car.1, 2, 3 It is therefore important to understand movement strategies observed during car transfer (CT) movements in individuals with tetraplegia, in order to maximize most patient rehabilitation.
No published study has specifically assessed CT in individuals with tetraplegia; however several studies have been conducted on transfer movement in individuals with spinal cord injury (SCI).4, 5, 6, 7, 8 Allison et al.4 investigated the movement patterns of a long sitting transfer in individuals with SCI (8 tetraplegics and 2 paraplegics with lesions from C5 to T10). Their report suggested that individuals with higher level lesions (C7 and higher) selected rotatory patterns that were characterized by an opposite direction movement between the head and pelvis.4, 5 Additionally, several other studies reported on the kinematic characteristics of posterior long sitting and sitting pivot transfers in individuals with SCI (C7 to L1).6, 7, 8, 9, 10 These studies indicated that the coordinated flexion movement between the head and trunk assist the buttocks to lift off the seat.
These earlier studies led us to hypothesize that individuals with tetraplegia would select not only a rotatory pattern of movement, but also a coordinated flexion movement between the head and trunk in CT. However, no studies on CT movement in individuals with C6 tetraplegia have yet been published. We believe that individuals with tetraplegia would have difficulty in performing CT movement under experimental conditions, as their wheelchairs and cars have different specifications. Thus, assessing and understanding the normal CT technique performed by individuals with tetraplegia in their natural environment may provide invaluable knowledge for SCI rehabilitation to promote motor performance in these individuals. Therefore, the purpose of the present study was to assess the normal CT technique performed by subjects with C6 tetraplegia who used their own wheelchair and car.
methods
Subjects
Four males with C6 tetraplegia took part in this study. All subjects had an impairment grade of A according to the American Spinal Injury Association (ASIA) guidelines,11, 12 and ASIA motor score ranged from 18 to 22. The time since injury was 12 to 20 years, respectively. The inclusion criteria for this study were as follows: (1) able to transfer from their wheelchair to a car independently with the use of a transfer board; (2) had neither a joint contracture nor fixed deformity in their elbow joints; (3) did not have pain in their shoulder joints; and (4) showed no restrictions after injury. Subject characteristics are presented in Table 1.
This study was approved by the Ethics Committee of the School of Comprehensive Rehabilitation, Osaka Prefecture University (09–102). The purpose of this study was explained to the subjects orally and in writing, and written consent was obtained.
Transfer movement from a wheelchair to a car
Subjects were instructed to perform a CT. In order to assess their normal technique of CT, they used their own wheelchair and car. All wheelchairs were manual-type wheelchairs, and their seating surfaces were backward-tilting. Additionally, all of their cars were station wagon-type vehicles, and their driver's seats were also backward-tilting. The difference between the height of the wheelchair and the driver's seat was less than 5 cm in all cases. Although each subject was able to position their wheelchair as they pleased, the wheelchair was positioned sideways at an angle of less than 40 degrees with respect to the target seat (Table 2).
Assessments of CT were conducted at a public parking area (Figure 1a). Once the wheelchair was positioned at the right side of the car, the subjects attempted to transfer themselves from the wheelchair into the driver's seat. The driver's side door was held open maximally (Figure 1). The starting position at each wheelchair was as follows: (1) trunk was extended as straight as possible, (2) both hands placed on the knees and (3) both feet placed on the footrest of their wheelchair. The end point of CT movement was sitting in each driver's seat. As the subjects had difficulty in lifting their buttocks, using their own supportive tool, such as a transfer board, was permitted to assist them. Each subject executed the CT movement twice, and there was no time restriction. Prior to initiating the transfers, subjects were instructed to perform their normal technique of CT. Moreover, the initial hand, foot and buttock positions were kept constant during all trials executed by each subject.

Methodology for recording transfer movement from a wheelchair to a car. Six digital video cameras were placed around the subject's car in a public parking area (a, b). Five of the six cameras (solid circles) were elevated to distinguish between the reflective markers attached on the subject's body (a). While the passenger's door was opened maximally (b), the other camera (dashed circle) was set up to the left of the car (a).
Kinematic assessments
Reflective markers were attached to the following body landmarks: top of crown, bilateral acromion processes, bilateral femoral greater trochanters and lateral epicondyles.
A three-dimensional video analysis system (ToMoCo VM; Toso System Inc, Saitama, Japan) was used to assess transfer movements, which were recorded on six digital video cameras (60 Hz) placed around the station wagons (Figure 1). Two cameras were placed at the left, front and right sides of the cars. Five of the six cameras (solid circles; Figure 1a) were elevated to distinguish the markers. While the passenger's door was opened maximally (Figure 1b), the other camera (dashed circle; Figure 1a) was set up to the left of the car. For the purpose of data analysis, the trial with the shortest duration was selected.
In this study, all cameras were not able to connect to a personal computer owing to the length of the cables. We therefore required synchronization of all cameras prior to recording. Cameras were positioned such that the study area could visualized by all the cameras and they were synchronized by having a research assistant stand within the common visual field and pop an air-filled balloon. All cameras were able to visualize the popping of the balloon simultaneously. Data collection was initiated once the cameras were synchronized.
The initial point of transfer was defined as the point at which the trunk started to move to laterally displace the buttocks. The end point of transfer was defined as the point at which the motion of the trunk stopped after sitting in the driver's seat. In addition, the x, y and z coordinates of each marker were digitized. In this study, the x, y and z axes were defined as the antero-posterior, medio-lateral and vertical direction, respectively. CT movement data, which included the total duration of the movement, that is, the lateral displacement of the head and buttocks, the angular displacement of neck flexion and trunk forward inclination, were collected. Based on Allison's study,4 lateral displacement of the buttocks was defined as lateral displacement (Y-displacement) of the midpoint between the bilateral great trochanter markers on the frontal plane. Similarly, the lateral distance of the head was defined as the lateral displacement of the top of the crown in this plane.
The approach used to compute the angular displacement of neck flexion and trunk forward inclination is presented in Figure 2. Neck flexion angle was defined as the angle between the top of the crown to the midpoint between the bilateral acromion process markers and the extended line from the midpoint between the bilateral great trochanter markers to the midpoint of the bilateral acromion process markers in the sagittal plane. Trunk forward inclination angle was defined as the angle from the midpoint between the bilateral acromion process markers to the midpoint between the bilateral great trochanter markers, and the vertical line (z-axis) through the midpoint between the bilateral great trochanter markers in this plane.

Angle (∠) (A) neck flexion angle. Angle (∠) (B) trunk forward flexion angle. • represents the reflective markers, and ○ represents the midpoints between the bilateral acromion process markers and the greater trochanter markers.
Data analysis
In general, transfer movement consists of three phases based on kinematic or kinetic parameters.4, 5, 6, 7, 8, 9, 10 However, we did not use these phases to classify transfer movement of our subjects, as they could not independently lift their buttocks off the wheelchair seat. Thus, in the present study, CT movement was assessed by focusing on the lateral displacement of the buttocks. Figure 3 shows lateral displacement of the buttocks in one representative trial. Specifically, two phases were categorized: a static phase and a dynamic phase. The static phase is when the buttocks were not moved, whereas the dynamic phase is when the buttocks were moved. These phases were repeated for all subjects; therefore, each phase was assigned a number in order (for example, static phase-I, dynamic phase-I, static phase-II, dynamic phase-II). As a result, several other phases were classified. Furthermore, according to this new classification, the distance and velocity of the lateral displacement of the buttocks were also calculated to clarify the kinematic characteristics. Finally, the ‘lift off’ phase was classified as the act of lifting the buttocks laterally off of the transfer board.

The phases of lateral displacement of the buttocks in a representative trial (that is, Subject-C). The static phase (S) is represented by no movement of the buttocks, whereas the dynamic phase (D) is represented by movement of the buttocks. Each phase was assigned a number in consecutive order (for example, SI, DI, SII, DII).
The kinematic data of each subject during the lift off phase were normalized to 100 data points for CT movement analysis. The correlation coefficient of the relationship between lateral displacement of the head and buttocks during the lift off phase was calculated to examine each subject's movement strategy. This analysis was similar to the one used by Allison et al.4 A translatory movement pattern was defined as a correlation greater than 0.70. A rotatory movement pattern was defined as a negative correlation, that is, the head moved in the opposite direction of the buttocks. A mixed pattern was any strategy that demonstrated poor-to-moderate positive correlations. Furthermore, the correlation coefficient of the relationship between angular displacement of neck flexion and trunk forward inclination during the lift off phase was also calculated to investigate each subject's movement strategy. Additionally, SPSS version 18 was used for statistical analysis. Significance level was set at P<0.05.
Results
Total duration of CT movement and the kinematic characteristics of each phase
The total duration of CT movement and the percentage of time spent in each phase are presented in Table 3. The mean time required for CT movement was 26.5±s.d. 9.1 s (range: 14.0–35.0 s). The total duration for subject-A was the longest among all subjects, whereas subject-C had the shortest duration.
Furthermore, each subject had different static and dynamic phase characteristics. Movement of subject-D consisted of three static phases, whereas all other subjects had two static phases. Conversely, subject-C had two dynamic phases, whereas the others had three dynamic phases. That is, movement of subject-C consisted of four phases, both subjects A and B had five phases, and subject-D had six phases. The percentages of time spent in the dynamic phase for subjects A and B were larger than those of the others.
The distances and velocities of lateral displacement of the buttocks are presented in Table 4. Subjects A and B had shorter distance than subjects C and D. Subject-C had the fastest dynamic phase-I. In dynamic phase-II, two subjects (that is, A and B) had shifted their buttocks laterally slower than the others. Moreover, subject-B shifted his buttocks laterally slower in dynamic phase-III.
Based on the scene of lifting their buttocks off of the transfer board, the lift off phase for each subject was defined as follows: two subjects (A and C) had achieved lift off in the final dynamic phase (II or III), and subjects B and D achieved lift off in dynamic phase-II.
Correlation between lateral displacement of the head and buttocks
Figure 4 shows the correlation coefficients for the relationship between lateral displacement of the head and buttocks during the lift off phase. All subjects demonstrated negative correlations greater than 0.70 during the lift off phase. In other words, all subjects selected a rotatory movement pattern where the head moved in the opposite direction of the buttocks.

Correlation coefficients of all subjects corresponding to the relationship between lateral displacement of the head and buttocks during the lift off phase. Movement patterns were defined by Allison et al.4 They are as follows: a translatory movement pattern is a correlation greater than 0.7 (high reliability); a rotatory movement pattern is a negative correlation, that is, the head moved in the opposite direction of the buttocks; and a mixed pattern is any strategy that demonstrated poor-to-moderate positive correlations.
Correlation between angle of neck flexion and trunk forward inclination
Two subjects (B and C) demonstrated negative correlations (r=−0.98 and r=−0.77), whereas subject-D demonstrated a positive correlation (r=0.75). Subject-A demonstrated no correlation (r=−0.36).
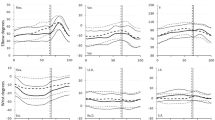
Figure 5 presents the angular displacements of neck flexion and trunk forward inclination during the lift off phase. Subject-D flexed his neck and trunk simultaneously in the lift off phase. The angular displacements of neck flexion and trunk forward inclination ranged from 30.4 to 47.2 degrees and 35.2 to 43.8 degrees, respectively. Subject-B forward inclined his trunk with extension of his neck. The angular displacements of his neck and trunk were in the range of 22.7–46.7 degrees and 37.6–45.2 degrees, respectively. Subject-C also flexed his trunk while extending his neck in the beginning of the lift off phase, and flexed his neck while extending his trunk at the end of the lift off phase. The ranges of neck flexion angle and trunk forward inclination angle for subject-C were 32.9–62.6 degrees and 18.1–26.7 degrees. In addition, subject-A showed the range of 34.1–58.5 degrees and 10.1–23.6 degrees.

The angular displacement of the neck flexion and trunk forward inclination during the lift off phase. An increased degree of neck and trunk angular displacement indicates flexion/forward inclination.
Discussion
Individuals with C6 tetraplegia have difficulty in performing a transfer movement, because of not only trunk paralysis but also upper extremity weakness and dysfunction.4, 5, 13 Additionally, CT movement requires various environmental supports, such as a transfer board for C6 tetraplegia. Individuals with tetraplegia should therefore select their own setting and use various compensatory patterns for accomplishing CT movement. We found no prior published study on the kinematic characteristics of CT movement in C6 tetraplegia. The present study, therefore, focused on the analysis of C6 tetraplegia CT movements in their natural environment.
By focusing on lateral displacement of the buttocks, it was possible to classify the CT movement of C6 tetraplegia into several static and dynamic phases. In the first and/or second dynamic phase, all subjects shifted their buttocks in their own wheelchair. That is, we assumed that these phases should be considered as a pre-lift off phase. The percentage of the pre-lift off phase was different for each subject. In other words, a longer percentage of the pre-lift off phase might suggest that some of the subjects (A and B) had a more severe impairment. This presumption could explain the shorter distance from their wheelchair to the driver's seat and the slow velocity of lateral displacement of their buttocks (Table 4). That is, a longer preparation period may be a compensatory strategy to avoid fatigue, and assure successful and safe transfer.
With respect to lateral displacement of the head and buttocks in CT movement, all four of the subjects selected a rotatory pattern of movement, where they shifted their buttocks from the wheelchair to the driver's seat, despite their different motor impairments (Figure 4). Although the movements observed in the present study are different from those of Allison et al.,4, 5 individuals with tetraplegia appear to prefer the rotatory pattern to lift and shift their buttocks in CT movement. However, the strategy of neck flexion and trunk forward inclination was different among the four subjects. Several researchers reported that individuals with thoracic SCI have coordinated flexion movement between the head and trunk so as to lift their buttocks.6, 7, 8, 9 In the present study, one subject (D) showed a similar coordinated flexion movement to lift his buttock. Only subject-D had a higher motor score for upper extremities (Table 1). We assumed that his greater upper extremity capacity contributed to his higher dynamic balance. Therefore, subject-D might be able to better coordinate flexion movement between the neck and trunk.
Conversely, two subjects (B and C) showed an opposite coordination of flexion movement between the head and trunk. Generally, subjects with tetraplegia have a lower dynamic balance capacity when compared with those with thoracic SCI.4, 5, 7, 14 Moreover, these two subjects (B and C) had lower capacity for upper extremities (Table 1). These subjects may, therefore, have difficulty in forward inclination of their trunk in order to shift their center of mass forward. Nevertheless, these subjects must incline their trunk more to shift their buttocks. In order to prevent the center of mass from shifting forward owing to their greater trunk inclination, two of the subjects (B and C) showed compensatory neck extension movements. Moreover, subject-B maintained his trunk forward inclination with his head putting on the door. Thus, subject-B had a greater angular displacement of trunk forward inclination than subject-C. We assumed that this compensation movement is one of the strategies of subjects with C6 tetraplegia to control their dynamic balance.
Subject-C performed CT movement with a different strategy from subject-B. Although subject-C also flexed his trunk with neck extension at the beginning of the lift off phase, he flexed his neck while extending his trunk at the end of the lift off phase. Subject-C had the fastest buttock lateral displacement velocity. Therefore, in order to keep his lower dynamic balance during the lift off phase, more complex control with the neck might be required. Thus, subject-C performed the movement of neck flexion and trunk forward inclination in two steps.
Subject-A had no correlation coefficient of the relationship between angular displacement of neck flexion and trunk forward inclination. That is, subject-A did not coordinate flexion movement between the neck and trunk fully (Figure 5). This incoordination might be attributed to a higher age when the injury occurred (Table 1). Several researchers reported that SCI patients with a higher age at the time of injury have overall had a poorer recovery of motor function and activities of daily living (ADL) capacity than those injured at a younger age.15, 16, 17 This may explain why subject-A did not coordinate flexion movement fully.
Finally, two subjects (B and D) demonstrated a motion phase to shift their body to the driver's seat after the lift off phase, whereas the others (A and C) did not demonstrate this type of motion. This finding suggests that these two subjects (A and C) have the lowest dynamic balance among the four subjects.
Based on our findings, individuals with C6 tetraplegia prefer the rotatory pattern of movement, where they lift and shift their buttocks. However, these individuals also showed different flexion movements between their neck and trunk. We believe that these different movement strategies are mainly attributed to their individual dynamic balance ability, which is impacted by upper extremities such as shoulder flexors, abductors. However, in this study, these muscle strengths could not be assessed. Understanding the kinematic characteristics of patients with C6 tetraplegia is important in order to eventually promote greater participation within the community.
The limitation of the present study is that the reproducibility of our findings was dependent on the equipment (that is, wheelchair and car) used. Moreover, the type of seat or cushions might affect the movement strategy. We did not fix the experimental conditions, thereby allowing the subjects to select their own strategy for CT movement.
Additionally, displacement of the buttocks in the horizontal plane does not strictly occur in the medio-lateral plane owing to change in the buttocks' movement direction during the transfer. Moreover, the model used in this study could not measure the complex mobility of the spine by multiple vertebras. It is very important for transfer movements among individuals with tetraplegia to consider the mobility of the spine. Therefore, the characteristics of CT movement in individuals with C6 tetraplegia have not been fully characterized. Future studies are warranted to increase our understanding of CT movement among individuals with tetraplegia.
Data Archiving
There was no data to deposit.
References
Carpenter C, Forwell SJ, Jongbloed LE, Backman CL . Community participation after spinal cord injury. Arch Phys Med Rehabil 2007; 88: 427–433.
Ku JH, Jang DP, Lee BS, Lee JH, Kim IY, Kim SI . Development and validation of virtual driving simulator for the spinal injury patient. Cyberpsycol Behav 2002; 5: 151–156.
Kiyono Y, Hashizume C, Matsui N, Ohtsuka K, Takaoka K . Car-driving abilities of people with tetraplegia. Arch Phys Med Rehabil 2001; 82: 1389–1392.
Allison GT, Singer KP, Marshall RN . Transfer movement strategies of individuals with spinal cord injuries. Disabil Rehabil 1996; 18: 35–41.
Allison GT, Singer KP, Marshall RN . Muscle activation patterns during transfer in individuals with spinal cord injury. Aust J Physiother 1995; 41: 169–176.
Gagnon D, Nadeau S, Gravel D, Noreau L, Lariviere C, Gagnon D . Biomechanical analysis of a posterior transfer maneuver on a level surface in individuals with high and low-level spinal cord injuries. Clin Biomech 2003; 18: 319–331.
Gagnon D, Nadeau S, Gravel D, Noreau L, Lariviere C, McFadyen B . Movement patterns and muscular demands during posterior transfers toward an elevated surface in individuals with spinal cord injury. Spinal Cord 2005; 43: 74–84.
Gagnon D, Nadeau S, Noreau L, Eng JJ, Gravel D . Trunk and upper extremity kinematics during sitting pivot transfers performed by individuals with spinal cord injury. Clin Biomech 2008; 23: 279–290.
Tanimoto Y, Nanba K, Tokuhiro A, Ukida H, Yamamoto H . Measurement system of transfer motion for patients with spinal cord injuries. IEEE Trans Instrum Meas 2008; 57: 213–219.
Gagnon D, Nadeau S, Noreau L, Dehail P, Gravel D . Quantification of reaction forces during sitting pivot transfers performed by individuals with spinal cord injury. J Rehabil Med 2008; 40: 468–476.
Dittuno JF, Young W, Donovan WH, Creasey G . The international standards booklet for neurological and functional classification of spinal cord injury. Paraplegia 1994; 32: 70–80.
Maynard FM, Bracken MB, Creasey G, Ditunno JF, Donovan WH, Ducker TB et al. International Standards for Neurological and Functional Classification of Spinal Cord Injury. Spinal Cord 1997; 35: 266–274.
Fujiwara T, Hara Y, Akaboshi K, Chino N . Relationship between shoulder muscle strength and functional independence measure (FIM) score among C6 tetraplegics. Spinal Cord 1999; 37: 58–61.
Gagnon D, Koontz AM, Murloy SJ, Nawoczenski DA, Forslund EB, Granstrom A et al. Biomechanics of sitting pivot transfers among individuals with a spinal cord injury: a review of the current knowledge. Top Spinal Cord Inj Rehabil 2009; 15: 33–58.
Jakob W, Wirz M, van Hedel HJA, Dietz V . Difficulty of elderly SCI subjects to translate motor recovery—‘Body Function’—into daily living activities. J Neurotrauma 2009; 26: 2037–2044.
Nyland J, Quigley P, Huang C, Lloyd J, Harrow J, Nelson A . Preserving transfer independence among individuals with spinal cord injury. Spinal Cord 2000; 38: 649–657.
Yarkony GM, Roth EJ, Heinemann AW, Lovell LL . Spinal cord injury rehabilitation outcome: the impact of age. J Clin Epidemiol 1988; 41: 173–177.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article
Cite this article
Kataoka, M., Yasuda, T., Kataoka, T. et al. Movement strategies during car transfers in individuals with tetraplegia: a preliminary study. Spinal Cord 50, 440–445 (2012). https://doi.org/10.1038/sc.2011.170
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2011.170
