
Abstract
The preoperative diagnosis of thyroid nodules now routinely includes BRAFV600E genetic testing in most provincial and municipal hospitals in China. This study identified the most suitable patients of thyroid nodule for BRAFV600E genetic testing. We retrospectively collected data of patients from the Hospital Information System that had undergone fine needle aspiration biopsy (FNAB) from May 2019 to December 2021. Data of FNAB, BRAFV600E genetic testing, and post-surgical pathological diagnosis were collected. A total of 12,392 patients were included in this study. Among them, 7,010 patients underwent solely FNAB, while 5,382 patients had both FNAB and BRAFV600E genetic testing. In the FNAB group, 2,065 thyroid nodules were surgically removed, with a 93.12% malignancy rate. In the FNAB + BRAF group, 2,005 nodules were dissected, and the malignancy rate was 98.20%. However, it was evident that in the subgroups, the combination of FNAB and BRAFV600E genetic testing only benefited Bethesda III (p < 0.001) and V (p = 0.001) nodules. Overall, the combination of FNAB with BRAFV600E genetic testing significantly improved the malignancy rate of surgical thyroid nodes at our hospital when compared to FNAB alone. The subgroup analysis showed that BRAFV600E genetic testing only benefited Bethesda III and V nodules. These findings provide a clinical reference for rationally selecting the most suitable population for BRAFV600E genetic testing.
Similar content being viewed by others

Introduction
The incidence of thyroid cancer has gradually increased worldwide over the past few decades. Thyroid cancer became the 11th most prevalent type of cancer in 2020, with 580,000 new cases being recorded globally1. The mortality of thyroid cancer has rarely changed, even though the incidence and new cases are both increasing. As previously mentioned, thyroid cancer may be overdiagnosed2,3. How to balance the diagnostic and therapeutic approaches such that benign thyroid nodules and lower-risk patients undergo minimal essential identification and treatment is an urgent challenge that has to be solved for doctors.
Papillary thyroid cancer (PTC) is the most common type of thyroid cancer, accounting for more than 90% of thyroid cancer cases4. The most common gene mutation in PTC is the BRAFT1799A mutation, which ultimately results in the BRAFV600E mutation5. B-type Raf kinase (BRAF) is a serine/threonine protein kinase, whose mutation helps to activate the mitogen-activated protein kinase (MAPK) signal transduction pathway6. BRAFV600E mutation is observed in about 43–88% PTC, 20–40% poorly differentiated thyroid cancer7,8,9,10,11, and 30–40% anaplastic thyroid cancer12. Clinically, the detection of preoperative or postoperative BRAF mutation exhibits a great impact on the diagnosis, prognostic stratification, and treatment of PTC. Nowadays, fine needle aspiration (FNA) can be done to obtain samples from the thyroid nodules for cytopathology and BRAF mutation detection. Many studies indicated that genetic testing of thyroid FNA samples greatly enhanced diagnostic accuracy and prognostication13,14. The final medical decision would be made by doctors and surgeons based on the features of medical imaging as well as the FNA cytopathological and genetic results.
The most suitable population of thyroid nodule for BRAF mutation detection must be identified to avoid overdiagnosis of thyroid cancer. The 2015 American thyroid association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer stated that molecular testing may be used to supplement malignancy risk assessment for nodules of atypia of undetermined significance (AUS)/ follicular lesion of undetermined significance (FLUS) (Bethesda III), follicular neoplasm (FN)/ suspicious for a follicular neoplasm (SFN) (Bethesda IV) and suspicious for malignancy (SFM) (Bethesda V)15,16. American Association of Clinical Endocrinologists/American College of Endocrinology/Associazione Medici Endocrinologi guidelines suggested that molecular testing could be performed for nodules that lacked established benign or malignant cytologic characteristics. Notably, BRAF mutation could guide to determine the scope of surgery17. According to European thyroid association guidelines, BRAF and RET/PTC mutations, as well as possibly PAX8/PPARG and RAS mutations, should be considered for cytologically indeterminate nodules, if available18. The Bethesda III and V nodules may benefit more from BRAF mutation detection because thyroid follicular neoplasm (Bethesda IV) cases with BRAF mutation are substantially less common19.
Since May 2019, we established BRAFV600E genetic testing based on fine-needle aspiration in Qilu Hospital, Shandong University. Here, we conducted a retrospective cohort study including 12,392 individuals who received FNA cytologic Bethesda grading with or without BRAFV600E genetic testing to determine the most suitable population for the test. We found that Bethesda III and V nodules were the only ones who benefited from BRAFV600E genetic testing as a supplement to FNA. Our findings provided a large database that may be used for rationally selecting the most suitable population for BRAF genetic testing. Additionally, our data provided a basis for avoiding overdiagnosis of thyroid nodule cases.
Methods
Study population
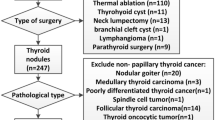
This study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committee of Qilu Hospital of Shandong University (ethical approval number KYLL-2018(KS)-226). The ethics committee of Qilu Hospital of Shandong University has approved that since only existing anonymized data were used in this study, it is not necessary to obtain the informed consent of each individual. We retrospectively collected data from all patients who underwent fine needle aspiration biopsy (FNAB), with or without BRAFV600E genetic testing, and post-surgical pathological diagnosis from the Hospital Information System of Qilu Hospital of Shandong University from May 2019 to December 2021. A total of 12,392 patients were included in this study. The BRAFV600E genetic testing and treatment plan were determined according to doctors' experience and patients' wishes. Among them, 7,010 patients underwent solely FNAB (FNAB group) and 5,382 patients underwent both FNAB and BRAFV600E genetic testing (FNAB + BRAF group). A total of 2,065 nodules in the FNAB group and 2,005 nodules in the FNAB + BRAF group were removed by surgery.
Cytology, BRAF V600E genetic testing and post-surgical pathological diagnosis
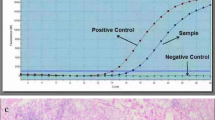
The procedure of FNAB was described in detail previously20. Cytological classification was based on The Bethesda System for Reporting Thyroid Cytopathology16. Real-time polymerase chain reaction (RT-PCR) was used for BRAFV600E genetic testing. The puncture tissue was stored in a 1.5 mL eppedorf tube containing 200µL lysate buffer and sent to the Department of Pathology for analysis. The BRAF p.V600E Mutations Detection Kit (Amoy Diagnostics Co., Ltd., Xiamen, China) was used for real-time PCR analysis. Primers and probes sequences are listed in Table 1. Post-surgical pathological diagnosis was based on the WHO Classification of Tumours of Endocrine Organs21.
Statistical analysis
Frequencies and percentages reported for categorical variables. Differences in frequencies were analyzed via the chi-square test. Two-tailed p < 0.05 was considered statistically significant. Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy were calculated for each detection method and combined methods, considering histology as the gold standard. All data were analyzed using SPSS 22.0 (SPSS Inc., Chicago, IL, USA) software.
Ethics approval
This study was approved by the ethics committee of Qilu Hospital of Shandong University (ethical approval number KYLL-2018(KS)-226).
Results
Characteristics of study participants
A total of 12,392 patients were included in this study. Among them, 7010 patients underwent only FNAB, while 5382 patients underwent both FNAB and BRAFV600E genetic testing. A total of 2065 thyroid nodules in the FNAB group underwent surgical removal, with a 93.12% malignancy rate. In the FNAB + BRAF group, 5469 nodules were aspirated for BRAFV600E genetic testing, and 3113 (56.92%) of them tested positive for the mutation, and a total of 2005 nodules were dissected with a malignancy rate of 98.20%. We analyzed the positive rates of BRAFV600E genetic testing in different cytology Bethesda groups (Table 2, demographic characteristics in Table S1).
Cytopathological examination and BRAF V600E analysis
The cytopathological results of the 5469 nodules that underwent BRAFV600E genetic testing are depicted in Fig. 1. The BRAFV600E mutation was identified in 3113/5469 nodules, and 2937 of these nodules were identified as malignant or SFM by cytology. In the remaining 176 BRAFV600E mutant nodules, cytology was consistent with 19 nondiagnostic, 17 benign, 139 AUS/FLUS, and 1 FN/SFN.

Cytology, BRAFV600E mutation and histology of thyroid nodules with BRAFV600E genetic testing.
The 7 BRAFV600E mutant patients out of the 19 patients who had nondiagnostic cytology underwent surgery in our hospital, and all of the post-surgical pathologies were determined as PTC. One BRAFV600E mutant patient with benign cytology underwent surgery and the pathology confirmed PTC. Out of the 139 BRAFV600E mutant patients with AUS/FLUS cytology, 67 underwent surgery, 66 were determined to be PTC, and the remaining patients had benign lesions. The only one BRAFV600E mutant patient of the 73 with FN/SFN cytology did not underwent thyroid surgery in our hospital.
Diagnostic value of cytology and BRAF V600E mutation analysis
We collected the post-surgical data to determine the diagnostic significance of cytology and BRAFV600E genetic testing. The overall malignancy rates of Bethesda I to VI were 75.00%, 35.29%, 91.76%, 10.00%, 98.68% and 99.77%. The malignancy rates of Bethesda I to VI in those BRAFV600E mutant patients were 100.00%, 100.00%, 98.51%, None, 100% and 99.94%. The malignancy rates of Bethesda I to VI in patients without BRAFV600E mutation were 40.00%, 31.25%, 66.67%, 10.00%, 94.12% and 97.89% (Table 3, demographic characteristics in Table S2). As shown in Table 4, patients in the FNAB + BRAF group who underwent surgical resection, either Cytology or BRAFV600E positive showed higher sensitivity (98.98%), NPV (59.18%) and accuracy (98.65%). Nevertheless, both cytology and BRAFV600E positive exhibited higher specificity (97.22%) and high PPV (99.94%).
Clinical benefits of the combination of cytology and BRAF V600E genetic testing
It is essential to better understand which patients can benefit from the combination of cytology and BRAFV600E genetic testing to reduce overdiagnosis of thyroid nodules. For all nodules, the combination enhanced the malignancy rate of the nodules that were destined to surgery(p < 0.001). However, in the subgroup analysis, the combination only benefited Bethesda III (p < 0.001) and V (p = 0.001) (Table 5, demographic characteristics in Table S3).
Discussion
The prevalence of thyroid cancer has increased significantly as people's health awareness and screening techniques have advanced22, yet mortality have remained consistently low23,24, indicating that there may be overdiagnosis and overtreatment of thyroid cancer25. Therefore, timely evidence of the epidemiological situation is needed to determine the magnitude of the problem and suggest workable solutions. The use of FNAB has significantly improved the accuracy of clinical diagnosis of thyroid nodules, and it is highly recommended as the gold standard for preoperative differentiation of benign and malignant thyroid nodules throughout the world15. Although most thyroid nodules can be accurately identified as benign or malignant by FNAB, 10%-30% of thyroid nodules are unable to be identified by FNAB and are classified as AUS/FLUS, FN/SFN or SFM16,26,27. Additionally, studies have shown that about 70–80% of these indeterminate nodules are eventually proven to be benign, allowing surgery to be avoided28. Uncertainty in cytology can lead to conflicting clinical decisions, which may result in unnecessary surgery or delay in the treatment of the disease.
With the rapid development of molecular biology, genetic tests have played an important role in the identification of benign and malignant thyroid nodules, and have gradually become the focus of researchers and clinicians29,30. The conventional basis for accurate diagnosis for FNAB will depend on certain experienced cytologists. While liquid based biopsy further improved the accuracy in comparison with crush cytology. Therefore, it will be expected that adding on genetic testing might further more increase the success rate of correct diagnosis pre-operatively. BRAF, a member of the MAPK pathway, is located on chromosome 7q34 and is a cytoplasmic serine-threonine protein kinase, which can cause phosphorylation and activation of the MAPK pathway, which is involved in cell metabolism, proliferation, differentiation, apoptosis, migration, and other processes31. BRAFV600E mutation is common in PTC, poorly differentiated thyroid cancer, and anaplastic thyroid cancer, and rare in follicular thyroid cancer, medullary thyroid cancer, benign thyroid adenoma, or hyperplasia32. According to research, BRAF mutations are found in roughly 43–88% of PTC7,8,9,10,11, making it the most frequent mutation in PTC. It is directly associated with aggressive tumor behavior and poor clinical outcome of PTC33. This phenomenon appears to be more pronounced in East Asian populations34. Due to the high frequency of BRAFV600E mutation in PTC, BRAFV600E mutation detection for diagnostic purposes has shown high sensitivity and specificity for determining the presence of tumor cells35. As a result, many provincial and municipal medical institutions in China have included BRAFV600E genetic testing as a routine item in the preoperative diagnosis of thyroid nodules in recent years, and overdiagnosis may be present3. However, it does not imply that all samples should be subjected to genetic testing. For specimens where a conclusive diagnosis can be made by cytology, genetic tests are not necessary. The latest version of The Bethesda System for Reporting Thyroid Cytology (TBSRTC) specifies that genetic tests should be used in FNA samples of thyroid nodules with an indeterminate diagnosis15,16. An important scientific question that needs to be seriously studied at the moment is how to prevent blindly following the trend in this surge and accomplish the sensible development and usage of genetic tests. Therefore, we conducted this study in an attempt to find a more suitable condition for the BRAFV600E genetic test to provide a basis for standardizing the diagnosis and treatment of thyroid nodules.
In this retrospective study, we determined the BRAFV600E mutation rate in thyroid nodules with different Bethesda grades of FNA cytology. The highest BRAFV600E mutation rate was found in Bethesda VI nodules, 90.74%; while the lowest BRAFV600E mutation rate was found in Bethesda II nodules, 1.28%. It was similar to the previous study by Chen et al. and correlated with the degree of benignity and malignancy of the nodules35. Additionally, very low (1.37%) of Bethesda IV nodules had BRAFV600E mutations, which was consistent with the characteristics of gene mutation in thyroid follicular tumors10. We analyzed 5469 thyroid nodules from patients that underwent both FNAB and BRAFV600E genetic testing, out of which 2005 underwent thyroid surgery at our institution, with a postoperative pathological malignancy rate of 98.20%, which was higher than that of patients who underwent FNAB alone and thyroid surgery during the same period (98.20% vs. 93.12%, p < 0.001), indicating that BRAFV600E genetic testing can assist the preoperative diagnosis of thyroid nodules. Especially for Bethesda III nodules, whether or not to perform thyroid lobectomy has become a vexing one for clinicians. Aggressive thyroid lobectomy may cause unnecessary trauma and increase the financial burden of the patient. This study showed that the postoperative pathological malignancy rate of Bethesda III nodules with positive BRAFV600E mutation reached 98.51%. Therefore, for Bethesda III nodules, combined with BRAFV600E genetic testing can provide a better basis for whether to perform a thyroid lobectomy.
We evaluated the diagnostic efficacy of cytology, BRAFV600E genetic testing, and their combination for the identification of benign and malignant thyroid nodules. BRAFV600E genetic testing alone performed better in terms of specificity and PPV for the identification of benign and malignant thyroid nodules, but it had lower sensitivity, NPV, and accuracy than cytology. This meant that in samples with an indeterminate diagnosis based on FNAB cytology, a positive BRAFV600E mutation suggested that the nodule was extremely likely to be PTC, but it was not sensitive enough in those with negative mutations to exclude the diagnosis of malignancy. When either cytology or BRAFV600E was positive, there was high sensitivity and NPV, which is a good diagnostic test for exclusion, and a negative result was accurate enough to ensure that the thyroid nodule was not malignant. When both cytology and BRAFV600E were positive, there was high specificity and PPV, indicating that the test is a solid confirmatory diagnostic test, and a positive result confirmed nodule malignancy.
It is widely accepted that enhancing the sensitivity and specificity of diagnostic methods for thyroid nodules is an effective way to minimize unnecessary surgery and overtreatment36. Overall, the combination of FNAB with the BRAFV600E genetic test at our hospital significantly improved the malignancy rate of surgical nodes compared to the FNAB alone. Because of the high sensitivity of cytology alone and the high specificity of BRAFV600E gene testing alone, there was a high sensitivity (98.98%) to identify the benign and malignant tumors by either cytological or BRAFV600E positivity, and high specificity (97.22%) by both cytological and BRAFV600E positivity. Clinically, we prefer high-sensitivity detection methods allow for early detection and removal of malignant nodules, resulting in a favorable prognosis for the patients.
However, a subgroup analysis of thyroid nodules of different Bethesda classifications revealed that the BRAFV600E genetic test was more appropriate for Bethesda III or V thyroid nodules and ineffective in Bethesda I, II, IV, and VI thyroid nodules. Therefore, expanding the detection of biomarkers of thyroid nodules blindly may lead to overtreatment and waste of medical resources. As a result, we recommend that patients with Bethesda III or V thyroid nodules perform FNA again to test BRAFv600E mutations, rather than conducting cytology combined with BRAFv600E gene testing for all patients. A recent study showed that the BRAFV600E mutation can be detected in FNA residual samples using a locked nucleic acid probe–based droplet digital polymerase chain reaction without using fresh puncture samples27. Therefore, BRAFV600E mutation may be detected in FNA residual samples for thyroid nodules with cytologically determined Bethesda III or V in the future.
In addition to the diagnosis of thyroid cancer, the BRAFV600E genetic test can aid in the development of treatment strategies for thyroid cancer patients37. If the BRAFV600E mutation is detected before treatment, it suggests a more aggressive tumor that requires a more extensive surgical option38,39,40. However, given the low-risk characteristics of most PTC in the clinic, genetic testing is expected to influence diagnosis and treatment decisions, but it cannot provide predictive power beyond Tumor Node Metastasis staging. The development of an American Thyroid Association risk stratification system remains the best way to predict the future recurrence of disease after initial treatment15. The future of genetic testing in thyroid pathology remains extremely promising and it has the potential to affect not just thyroid nodule diagnosis and surgery, but also the role of radioiodine therapy in the treatment and other possible systemic therapies.
Our study had the following limitations. Only the malignant rate of surgical pathology was analyzed, without subdivision of surgical methods, thyroid cancer classification, size, and number of lesions, cervical lymph nodes, or distant metastases. The enrolled samples had a high rate of postoperative histopathological malignancy. However, we enrolled all patients with FNAB + BRAF from May 2019 to December 2021, which to some extent avoided sample selection bias and also reflected the high accuracy of our hospital (as the largest general hospital in Shandong Province) in the diagnosis of thyroid nodules. We only counted the post-surgical pathological diagnosis of patients who underwent surgery at our hospital. Since our hospital is a regional medical center, patients are willing to come to our hospital to clarify the diagnosis and determine the treatment plan. But due to the limited medical resources of our hospital, some patients will go to other hospitals for surgery after clarifying the diagnosis and treatment plan, and the post-surgical pathological diagnosis of these patients were not included in this study.
We performed a retrospective cohort study including 12,392 patients who had FNA cytologic Bethesda grading with or without BRAFV600E genetic testing. This is a real-world study, which can reflect the application value of BRAFV600E genetic testing for the identification of benign and malignant thyroid nodules before surgery. We found that the addition of BRAFV600E genetic testing benefited only Bethesda III and V nodules. Our findings provided a large database that may be used for rationally selecting the most suitable population for BRAFV600E genetic testing. Additionally, our data provided a basis for avoiding overdiagnosis in thyroid nodule patients.
Data availability
De-identified individual data might be available following publication by reasonable request to the corresponding author accompanied by research proposal.
References
Sung, H. et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 71(3), 209–249. https://doi.org/10.3322/caac.21660 (2021).
Li, M., Dal Maso, L. & Vaccarella, S. Global trends in thyroid cancer incidence and the impact of overdiagnosis. Lancet Diabetes Endocrinol. 8(6), 468–470. https://doi.org/10.1016/S2213-8587(20)30115-7 (2020).
Ahn, H. S., Kim, H. J. & Welch, H. G. Korea’s thyroid-cancer “epidemic”–screening and overdiagnosis. N Engl J Med. 371(19), 1765–1767. https://doi.org/10.1056/NEJMp1409841 (2014).
Davies, L. & Hoang, J. K. Thyroid cancer in the USA: Current trends and outstanding questions. Lancet Diabetes Endocrinol. 9(1), 11–12. https://doi.org/10.1016/S2213-8587(20)30372-7 (2021).
Cancer Genome Atlas Research Network. Integrated genomic characterization of papillary thyroid carcinoma. Cell. 159(3), 676–690. https://doi.org/10.1016/j.cell.2014.09.050 (2014).
Puxeddu, E., Durante, C., Avenia, N., Filetti, S. & Russo, D. Clinical implications of BRAF mutation in thyroid carcinoma. Trends Endocrinol Metab. 19(4), 138–145. https://doi.org/10.1016/j.tem.2007.12.003 (2008).
Nikiforova, M. N. et al. BRAF mutations in thyroid tumors are restricted to papillary carcinomas and anaplastic or poorly differentiated carcinomas arising from papillary carcinomas. J. Clin. Endocrinol. Metab. 88(11), 5399–5404. https://doi.org/10.1210/jc.2003-030838 (2003).
Cohen, Y. et al. BRAF mutation in papillary thyroid carcinoma. J. Natl. Cancer Inst. 95(8), 625–627. https://doi.org/10.1093/jnci/95.8.625 (2003).
Kimura, E. T. et al. High prevalence of BRAF mutations in thyroid cancer: genetic evidence for constitutive activation of the RET/PTC-RAS-BRAF signaling pathway in papillary thyroid carcinoma. Cancer Res. 63(7), 1454–1457 (2003).
Kebebew, E. et al. The prevalence and prognostic value of BRAF mutation in thyroid cancer. Ann Surg. 246(3), 466–471. https://doi.org/10.1097/SLA.0b013e318148563d (2007).
Mathur, A. et al. Higher rate of BRAF mutation in papillary thyroid cancer over time: a single-institution study. Cancer. 117(19), 4390–4395. https://doi.org/10.1002/cncr.26072 (2011).
Begum, S. et al. BRAF mutations in anaplastic thyroid carcinoma: implications for tumor origin, diagnosis and treatment. Mod Pathol. 17(11), 1359–1363. https://doi.org/10.1038/modpathol.3800198 (2004).
Nikiforova, M. N. & Nikiforov, Y. E. Molecular diagnostics and predictors in thyroid cancer. Thyroid. 19(12), 1351–1361. https://doi.org/10.1089/thy.2009.0240 (2009).
Kim, S. W. et al. BRAFV600E mutation analysis in fine-needle aspiration cytology specimens for evaluation of thyroid nodule: a large series in a BRAFV600E-prevalent population. J. Clin. Endocrinol. Metab. 95(8), 3693–3700. https://doi.org/10.1210/jc.2009-2795 (2010).
Haugen, B. R. et al. 2015 American thyroid association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: The American thyroid association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid. 26(1), 1–133. https://doi.org/10.1089/thy.2015.0020 (2016).
Cibas, E. S. & Ali, S. Z. The 2017 bethesda system for reporting thyroid cytopathology. Thyroid. 27(11), 1341–1346. https://doi.org/10.1089/thy.2017.0500 (2017).
Gharib, H. et al. AACE/ACE/AME task force on thyroid nodules. American association of clinical endocrinologists, American college of endocrinology, and associazione medici endocrinologi medical guidelines for clinical practice for the diagnosis and management of thyroid nodules-2016 update. Endocr. Pract. 22(5), 622–639. https://doi.org/10.4158/EP161208.GL (2016).
Paschke, R. et al. European thyroid association guidelines regarding thyroid nodule molecular fine-needle aspiration cytology diagnostics. Eur. Thyroid. J. 6(3), 115–129. https://doi.org/10.1159/000468519 (2017).
Carty, S. E. et al. The clinical utility of molecular testing in the management of thyroid follicular neoplasms (Bethesda IV Nodules). Ann. Surg. 272(4), 621–627. https://doi.org/10.1097/SLA.0000000000004130 (2020).
Gong, L. et al. BRAF pV600E genetic testing based on ultrasound-guided fine-needle biopsy improves the malignancy rate in thyroid surgery: Our single-center experience in the past 10 years. J. Cancer Res. Clin. Oncol. https://doi.org/10.1007/s00432-022-04235-3 (2022).
Lloyd, R. V., Osamura, R. Y., Kioppel, G. & Rosai, J. International Agency for Research on Cancer. WHO Classifcation of Tumours of Endocrine Organs. IARC Who Classifcation of Tumours, Lyon (2017)
Shao, C. et al. Optical diagnostic imaging and therapy for thyroid cancer. Mater. Today Bio. 17, 100441. https://doi.org/10.1016/j.mtbio.2022.100441 (2022).
La Vecchia, C. et al. Thyroid cancer mortality and incidence: A global overview. Int. J. Cancer. 136(9), 2187–2195. https://doi.org/10.1002/ijc.29251 (2015).
Li, M., Brito, J. P. & Vaccarella, S. Long-term declines of thyroid cancer mortality: An international age-period-cohort analysis. Thyroid. 30(6), 838–846. https://doi.org/10.1089/thy.2019.0684 (2020).
Pizzato, M. et al. The epidemiological landscape of thyroid cancer worldwide: GLOBOCAN estimates for incidence and mortality rates in 2020. Lancet Diabetes Endocrinol. 10(4), 264–272. https://doi.org/10.1016/S2213-8587(22)00035-3 (2022).
Rossi, E. D., Pantanowitz, L. & Faquin, W. C. The role of molecular testing for the indeterminate thyroid FNA. Genes 10(10), 736. https://doi.org/10.3390/genes10100736 (2019).
Fu, G., Chazen, R. S., MacMillan, C., Witterick, I. J. Development of a Molecular Assay for Detection and Quantification of the BRAF Variation in Residual Tissue From Thyroid Nodule Fine-Needle Aspiration Biopsy Specimens [published correction appears in JAMA Netw Open. 2022 Mar 1;5(3):e225698]. JAMA Netw. Open. 4(10), e2127243. https://doi.org/10.1001/jamanetworkopen.2021.27243. (2021)
American Thyroid Association (ATA) Guidelines Taskforce on Thyroid Nodules and Differentiated Thyroid Cancer; Cooper, D.S., et al. Revised American thyroid association management guidelines for patients with thyroid nodules and differentiated thyroid cancer [published correction appears in Thyroid. 2010;20(8):942. Hauger, Bryan R [corrected to Haugen, Bryan R]] [published correction appears in Thyroid. 2010 Jun;20(6):674–5]. Thyroid. 19(11), 1167–1214. https://doi.org/10.1089/thy.2009.0110. (2009)
Labourier, E. et al. Molecular testing for miRNA, mRNA, and DNA on fine-needle aspiration improves the preoperative diagnosis of thyroid nodules with indeterminate cytology. J. Clin. Endocrinol. Metab. 100(7), 2743–2750. https://doi.org/10.1210/jc.2015-1158 (2015).
Fuller, M. Y. et al. Next-generation sequencing identifies gene mutations that are predictive of malignancy in residual needle rinses collected from fine-needle aspirations of thyroid nodules. Arch. Pathol. Lab. Med. 142(2), 178–183. https://doi.org/10.5858/arpa.2017-0136-OA (2018).
Kciuk, M., Gielecińska, A., Budzinska, A., Mojzych, M. & Kontek, R. Metastasis and MAPK Pathways. Int. J. Mol. Sci. 23(7), 3847. https://doi.org/10.3390/ijms23073847 (2022).
Xing, M. BRAF mutation in thyroid cancer. Endocr Relat Cancer. 12(2), 245–262. https://doi.org/10.1677/erc.1.0978 (2005).
Caronia, L. M., Phay, J. E. & Shah, M. H. Role of BRAF in thyroid oncogenesis. Clin. Cancer Res. 17(24), 7511–7517. https://doi.org/10.1158/1078-0432.CCR-11-1155 (2011).
Liang, J. et al. Genetic landscape of papillary thyroid carcinoma in the Chinese population. J. Pathol. 244(2), 215–226. https://doi.org/10.1002/path.5005 (2018).
Chen, H. et al. BRAFV600E mutation test on fine-needle aspiration specimens of thyroid nodules: Clinical correlations for 4600 patients. Cancer Med. 11(1), 40–49. https://doi.org/10.1002/cam4.4419 (2022).
Nikiforov, Y. E. et al. Nomenclature revision for encapsulated follicular variant of papillary thyroid carcinoma: A paradigm shift to reduce overtreatment of indolent tumors. JAMA Oncol. 2(8), 1023–1029. https://doi.org/10.1001/jamaoncol.2016.0386 (2016).
Tao, Y. et al. BRAF V600E status sharply differentiates lymph node metastasis-associated mortality risk in papillary thyroid cancer. J. Clin. Endocrinol. Metab. 106(11), 3228–3238. https://doi.org/10.1210/clinem/dgab286 (2021).
Yip, L. et al. Tumor genotype determines phenotype and disease-related outcomes in thyroid cancer: A study of 1510 patients. Ann. Surg. 262(3), 519–525. https://doi.org/10.1097/SLA.0000000000001420 (2015).
Krasner, J. R. et al. Molecular mutations as a possible factor for determining extent of thyroid surgery. J. Otolaryngol. Head Neck Surg. 48(1), 51. https://doi.org/10.1186/s40463-019-0372-5 (2019).
Kim, S. K. et al. Role of BRAF V600E mutation as an indicator of the extent of thyroidectomy and lymph node dissection in conventional papillary thyroid carcinoma. Surgery 158(6), 1500–1511. https://doi.org/10.1016/j.surg.2015.05.016 (2015).
Acknowledgements
We thank Jinan Clinical Research Center for Endocrine and Metabolic Diseases for its support.
Funding
This study was funded by the National Natural Science Foundation of China (Grant No. 81900756, 82070800, 82270845), a Special fund for Taishan industrial leading talent project, and supported by Jinan Clinical Research Center for Endocrine and Metabolic Diseases.
Author information
Authors and Affiliations
Contributions
K.L. and L.C. contributed to the design of the study. Y.L., X.G., M.Y., K.W., G.C., Y.L., X.H. organized the database. K.L. performed the statistical analysis. Y.L. and X.G. wrote the draft of the manuscript. K.L. and L.C. revised the manuscript. All authors contributed to manuscript revision, read, and approved the submitted version.
Corresponding authors
Ethics declarations
Competing interests
The authors have no relevant financial or nonfinancial interests to disclose.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Lu, Y., Guo, X., Yang, M. et al. BRAFV600E genetic testing should be recommended for Bethesda III or V thyroid nodules based on fine-needle aspiration. Sci Rep 13, 17129 (2023). https://doi.org/10.1038/s41598-023-44464-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-44464-1
This article is cited by
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
