
Abstract
The aim of this meta-analysis was to assess the association of general anesthesia (GA) exposure with the risk of POD in this patient population. Databases including Medline, EMBASE, Cochrane library, and Google Scholar were searched from inception to December 2022. Analysis of 17 studies published between 2015 and 2021 involving 10,678 individuals revealed an association of GA exposure with an elevated risk of POD [odd ratio (OR) = 1.846, 95% CI 1.329 to 2.563, p = 0.0003, I2 = 68.4%, 10,678 patients]. Subgroup analysis of the diagnostic methods also demonstrated a positive correlation between GA exposure and POD risk when validated methods were used for POD diagnosis (OR = 2.199, 95% CI 1.46 to 3.31, p = 0.0002). Meta-regression analyses showed no significant impact of age, male proportion, and sample size on the correlation between GA and the risk of POD. The reported overall incidence of POD from the included studies regardless of the type of anesthesia was between 0.8 and 27%. Our meta-analysis showed a pooled incidence of 10.3% (95% CI 7% to 15%). This meta-analysis suggested an association of general anesthesia with an elevated risk of postoperative delirium, implying the necessity of implementing appropriate prophylactic strategies against this complication when general anesthesia was used in this clinical setting.
Similar content being viewed by others

Introduction
Transcatheter aortic valve replacement (TAVR), which is a minimally invasive therapeutic procedure for aortic stenosis1, is typically performed in patients who are considered high-risk for traditional open-heart surgery1. TAVR has become increasingly popular in recent years due to its minimally invasive nature and high success rate2,3. Although it is conventionally conducted under general anesthesia (GA) with most patients being discharged from the hospital within a few days after the procedure4, postoperative delirium (POD) characterized by a fluctuation in mental status may occur5,6. POD occurs most commonly between postoperative days 1 and 3 when patients may present with confusion, a reduced awareness of the environment, disorientation, a disturbance of attention, and changes in behavior7,8,9. Following TAVR, the pooled incidence of POD was reportedly up to 8.1–9.8% in previous meta-analyses10,11. Not only may POD significantly prolong hospitalization and increase medical expenditure12,13,14,15, but it has also been shown to be an independent risk factor for mortality in patients undergoing TAVR14,15,16,17. Therefore, prevention of POD through pre-procedural identification of its risk factors may help in timely implementation of appropriate prophylactic and management strategies to improve the quality of patient care12.
The reported risk factors for POD following TAVR include advanced age, non-transfemoral (i.e., transapical/transaortic) access, the presence of carotid artery disease, male gender, stroke, current smoking, and history of atrial fibrillation14,15. Besides, GA exposure has been shown to be a potential risk factor for POD in this patient population11. Although avoidance of GA exposure is believed to prevent POD, findings from current literature remain inconclusive18,19,20,21,22,23. Two recent randomized controlled trials (RCTs) demonstrated no significant difference in the occurrence of POD between patients undergoing regional anesthesia and those receiving GA for orthopedic surgeries24,25. For patients undergoing TAVR, several retrospective studies reported the association of GA exposure with an elevated risk of POD14,15,26,27, while evidence from a RCT involving 438 patients indicated no increased risk of POD with the use of GA compared to local anesthesia/conscious sedation28.
Although a recent updated meta-analysis attempted to explore the relationship between GA exposure and POD risk11, inclusion of a limited number of patients (e.g., unadjusted data from 3555 patients and adjusted data from 1537 patients) may bias their results. Through focusing on general anesthesia and adopting a more comprehensive analytical approach, the current meta-analysis aimed at elucidating the association of GA exposure with the risk of POD in those undergoing TAVR.
Methods
The protocol of the present meta-analysis was registered in PROSPERO (CRD42023398788). The presentation of the current study followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement.
Database search strategy
We searched four databases including Medline, Google Scholar, Embase, and Cochrane library for relevant studies from inception to February 10, 2023. The key words used for screening included: (“transcatheter aortic valve replacement” or “transcatheter aortic valve implantation” or “TAVR” or “TAVI” or “Aortic valve stenosis”) and (“general anesthesia” or “anesthesia” or “endotracheal intubation” or “inhalation agents”) and (“delirium” or “postoperative delirium” or “Confusion Assessment Method” or “acute brain failure” or “cognitive decline” or “altered mental status” or “cognitive dysfunction” or “organic brain syndrome” or “cognition impairment” or ”acute brain dysfunction”). There was no restriction on publication year or language when searching the databases. Reference lists of the retrieved studies were examined to identify potentially eligible articles that were not included on initial literature search. Supplementary Table 1 summarized the details on search strategies used in one of the databases (i.e., Medline).
Studies selection and inclusion criteria
Two authors independently screened the titles and abstracts of the acquired articles based on predefined criteria before reading the full texts to make the final decision. Any disagreement on studies selection was resolved through discussion. Eligible articles must meet the following criteria: (1) Population: adults undergoing TAVR regardless of its site of access; (2) Intervention: GA was used for TAVR without restriction on the strategy of airway management (e.g., supraglottic airway devices or endotracheal intubation) or the anesthetics used (e.g., inhalation agents or intravenous anesthetics); (3) Comparison: local anesthesia or/and conscious sedation/monitored anesthesia care; (4) Outcomes: risk of POD, and (5) Type of article: RCTs or retrospective cohort studies considered eligible for the current meta-analysis.
Studies were excluded if they (1) recruited surgical or pediatric population; (2) did not report relevant details for risk calculation (e.g., events and total number); and (3) were published as letters, reviews, case reports, or conference abstracts.
Data extraction, quality assessment, and certainty of evidence
Two independent authors extracted relevant details from the eligible articles, including the patient characteristics (i.e., age, male proportion, and body mass index), first author, year of publication, sample size, methods for diagnosing POD, incidence of delirium, ejection fraction, and country. A third author was involved for any disagreement on data extraction. When there was an overlap of patient populations between different studies, the study with a complete data set and/or with the largest estimated population was selected. If necessary, we emailed the authors of the included studies for missing information. The quality of individual studies was appraised with Newcastle–Ottawa Scale (NOS) for observational studies or the Cochrane Collaboration’s risk of bias tool (ROB 2.0) for RCTs. When using NOS, cohort studies being assigned more than seven points were considered low risk of bias. The overall certainty of evidence was assessed with the Grading of Recommendations Assessment, Development and Evaluation (GRADE) framework.
Outcomes and subgroup analysis
The primary outcome of this study was the correlation of GA exposure with the risk of POD, while the pooled incidence of POD among patients receiving TAVR was the secondary outcome. Subgroup analysis was performed based on the methods for diagnosis of POD. Validated methods referred to the use of standardized tools designed specifically for diagnosing delirium, such as the Confusion Assessment Method (CAM), Confusion Assessment Method for the Intensive Care Unit (CAM-ICU), Nursing Delirium Screening Scale (NU-DESC), and criteria from the Diagnostic and Statistical Manual of Mental Disorders (DSM). Non-validated methods referred to diagnosis of POD based on non-standardized approaches, such as symptom evaluation or use of a chart-based delirium identification instrument.
Statistical analysis
The primary outcome was presented as odds ratios (ORs) with 95% confidence intervals (CI). The heterogeneity among the included studies was examined with I2 statistics with I2 < 50% signifying homogeneity. Taking into account the heterogeneity in patient population and study design, all analyses were conducted based on the Mantel–Haenszel random-effects model. Meta-regression analysis was used to explore the source of heterogeneity as previously reported29,30. The likeliness of publication bias was assessed by funnel plots for outcomes reported in 10 or more studies. To examine the robustness of the results and identify the source of heterogeneity, sensitivity analysis was performed through a leave-one-out approach. The comprehensive Meta-Analysis (CMA) V3 software (Biostat, Englewood, NJ, USA) was adopted for all statistical analyses, in which significance referred to a probability value (p) less than 0.05.
Results
Study selection and quality
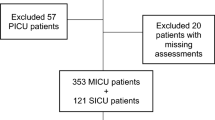
Of the 260 records initially identified through a comprehensive search of the four different databases, 46 were duplicate publications and 182 did not meet the criteria for full-text reading. Reviewing the full text of the remaining 32 studies further excluded 15 publications based on a variety of reasons (Fig. 1). Finally, 17 articles published between 2015 and 2021 were deemed eligible for the current meta-analysis14,15,26,27,28,31,32,33,34,35,36,37,38,39,40,41,42. Figure 1 summarized the process to identify studies.

Selection process of studies based on search strategies.
Characteristics of the 17 included studies with a total of 10,678 patients receiving TAVR are shown in Table 1. Of the 17 studies, 13 adopted a retrospective design14,26,31,32,33,34,35,36,37,38,39,40,42, three used a prospective design15,27,41, and one was a RCT28. The mean age of the patients ranged from 74.68 to 85 years, with a male gender distribution ranging from 36.9 to 65%. There was a wide variation in sample size across the included studies (range: 78 to 5248 patients). The information on body mass index (range: 23.18 to 28.4 kg/m2) was available in 12 studies, while it was unavailable in the other five studies15,26,38,39,41. Of 17 studies, 10 used validated methods for POD diagnosis14,15,26,27,28,31,38,39,40,41, namely the CAM, CAM-ICU, NU-DESC, DSM IV, and DSM V. Five studies did not report the diagnostic measures for POD32,33,34,36,42, and the two remaining studies based their diagnosis of POD on clinical symptoms (e.g., any acute disturbance of consciousness with decreased attention)35 or chart-based delirium identification instrument37, respectively.
The quality of cohort studies (n = 13) is summarized in Table 1. In brief, all 17 studies were considered to be of high quality (range of NOS: 7–9). For the only RCT28, the risk of bias is deemed low.
Outcomes
Primary outcome: association of GA exposure with risk of POD
Meta-analysis of 17 studies revealed an association of GA with an elevated risk of POD (OR = 1.846, 95% CI 1.329 to 2.563, p = 0.0003, I2 = 68.4%, 10,678 patients) (Fig. 2)14,15,26,27,28,31,32,33,34,35,36,37,38,39,40,41,42. Sensitivity analysis confirmed the robustness of evidence (Supplemental Fig. 1). Subgroup analysis of the diagnostic methods also demonstrated a positive correlation between GA exposure and POD risk when the validated methods were used for POD diagnosis (OR = 2.199, 95% CI 1.46 to 3.31, p = 0.0002)14,15,26,27,28,31,38,39,40,41 (Fig. 3). However, there was no significant link between GA and the risk of POD when non-validated diagnostic methods were used (OR = 1.145, 95% CI 0.83 to 1.581, p = 0.4092) (Fig. 3)32,33,34,35,36,37,42. Publication bias was deemed low on funnel plot examination (Supplemental Fig.2).

Forest plot showing the risk of postoperative delirium among patients with general anesthesia and those without.

Subgroup analysis demonstrating the association of general anesthesia with the risk of postoperative delirium focusing on the use of validated versus non-validated diagnostic methods.
Meta-regression analyses showed no significant impact of age on the association between GA exposure and the risk of POD (coefficient: − 0.028, p = 0.742) (Fig. 4). There were also no significant influences of other covariates including male proportion (coefficient: 0.019, p = 0.53) (Fig. 5) and sample size (coefficient: -0.0002, p = 0.149) (Fig. 6) on the correlation between GA and POD risk.

Meta-regression analysis showing non-significant correlation between patient age and study outcome.

Meta-regression analysis indicating non-significant association between male proportion and study outcome.

Meta-regression analysis demonstrating non-significant correlation between sample size and study outcome.
Secondary outcome: incidence of postoperative delirium
The reported overall incidence of POD from the included studies regardless of the type of anesthesia was between 0.8 and 27% (Table 1). Our meta-analysis showed a pooled incidence of 10.3% (95% CI 7% to 15%) (Figure not shown). Subgroup analysis revealed a pooled incidence of 13.3% when focusing on validated methods for POD diagnosis, while it was 6.4% if non-validated methods were used (Fig. 7).

Forest plot showing the pooled incidence of postoperative delirium based on validated or non-validated methods for postoperative delirium (POD) diagnosis. CI: confidence interval.
Certainty of evidence
The certainty of evidence, which was downgraded due to a high heterogeneity (I2 = 68.4%), was considered very low for the primary outcome.
Discussion
Through a meta-analysis of 17 studies involving 10,678 patients, the current study revealed a statistically significant association of GA exposure with an increased risk of POD in individuals undergoing TAVR. Sensitivity analysis demonstrated consistency of our result. Subgroup analysis based on studies that used validated tools for POD diagnosis also supported the finding. In addition, there was a low risk of publication bias in the current meta-analysis, indicating the robustness of our results. Furthermore, age, sample size, and male proportion had no significant influence on the correlation between GA exposure and POD risk according to meta-regression analysis. To our best knowledge, the present meta-analysis is the first extensive review to focus on the relationship between GA exposure and the risk of POD following TAVR.
Our analysis showed a pooled POD incidence of 10.3% after TAVR. The incidence of POD varies among different surgical populations. In patients receiving surgery for hip fracture, the incidence has been reported to be 16–62%43. For those receiving cardiac surgery, POD occurs in 8–31% of patients, ranging from 25 to 52% in those aged 60 or above and 31–66% in those aged over 7014. The etiology of POD comprises a complex combination of predisposing factors, including advanced age, pre-existing cognitive impairment, depression, vision impairment, previous stroke, and precipitating factors such as surgery, acute pain, malnutrition, and hospitalization7. The reduced incidence of POD in our patients undergoing TAVR could be attributed to the absence of factors associated with surgery or pain that might trigger it.
Besides inflammatory response that has been proposed to be a contributor to POD7, several modifiable and non-modifiable risk factors were identified in a recent large-scale meta-analysis of 69 studies focusing on patients undergoing TAVR without exposure to surgery-induced inflammatory response11. Non-modifiable predisposing factors included advanced age, prior stroke/transient ischemic attack, male gender, and postoperative acute kidney injury, atrial fibrillation/flutter, and impaired Instrumental Activities of Daily Living11, while modifiable risk factors consisted of GA exposure, weight loss, electrolyte imbalance, and techniques of TAVR (e.g., non-transfemoral Access)11. Despite the inclusion of up to 69 studies in that meta-analysis, it involved only nine studies with 3,555 patients when assessing the impact of GA on the risk POD11. In contrast, our investigation included 17 studies involving 10,678 patients. In addition, we conducted meta-regression analysis to explore the source of heterogeneity.
In our meta-regression analysis, the absence of age and sex influences on the GA-POD link is interesting. Advanced age and male sex are well-established risk factors for POD based on previous research11. The lack of association in this meta-regression analysis suggests that GA exposure may increase the risk of POD regardless of age and sex in patients undergoing TAVR. However, it should be noted that uncontrolled confounding factors (e.g., frailty) could have obscured any potential effects of age and gender on the GA-POD association. In addition, the lack of an association between age/sex and GA-POD risk may be due to insufficient heterogeneity in these covariates rather than a true lack of effect. More research is needed to control for relevant confounders to determine whether age or sex interacts with GA to modify POD risk after TAVR.
Although the correlation between GA exposure and an elevated risk of POD remains controversial18,19,20,21,22,23, it is generally believed that GA exposure would lead to an increased risk of POD; however, a large-scale RCT that randomly assigned patients to either GA or spinal anesthesia did not find any difference in the incidence of POD between the two groups44, suggesting no causality between GA exposure and the subsequent POD. On the other hand, several studies reported an association of a proinflammatory state with the development of POD45,46,47, highlighting inflammation as a potential underlying mechanism. Consistently, a previous meta-analysis of 54 observational studies revealed significantly increased circulating C-reactive protein and interleukin-6 concentrations in patients with POD48. Furthermore, intrinsic immune response activation has recently been proposed to be a mechanism underlying the occurrence of POD49,50. Such neuroinflammation, which can be triggered by surgical trauma or systemic diseases51, could result in neuronal dysfunction and death52.
There may be several possible explanations for the association between GA exposure and an elevated POD risk in the current meta-analysis (i.e., OR = 1.846). First, old age is a known risk factor for POD11. A previous study reported a positive correlation between an increasing age and the occurrence of POD with the incidence of POD being 22% in patients aged 50–59 but up to 92% in those aged 80–8953. Therefore, our inclusion of individuals undergoing TAVR, who are frequently elderly (i.e., age range: 74.68–85), may increase their susceptibility to POD. Second, compared to other anesthetic techniques (e.g., sedation or local anesthesia), the use of GA may lead to a higher risk of peri-procedural hypotension54, which is a potential risk factor for POD55,56,57. Third, a previous meta-analysis has reported that GA exposure may significantly increase the risk of prolonged mechanical ventilation and acute kidney injury54, which are also known risk factors for POD58,59. Fourth, besides advanced age, patients receiving TAVR are characterized by frailty, malnutrition, and extensive comorbidities15, which may render this population particularly vulnerable to the development of POD following GA exposure. In summary, the increased risk of POD in this patient population may be attributed to the interaction between GA exposure, advanced age, comorbidities, malnutrition as well as GA-related complications.
A significant association between GA and elevated risk of POD was observed in studies employing validated diagnostic tools, whereas studies utilizing non-validated methods did not show a significant correlation. We suggest that validated diagnostic tools specifically designed to identify delirium (e.g., CAM) may be more accurate and sensitive for detecting POD than non-standardized symptom-based evaluations. Therefore, studies using validated tools may identify a greater proportion of POD cases, strengthening the observed association between GA and POD risk. In contrast, non-validated chart-based screening methods are likely to have a lower sensitivity for POD diagnosis. Consequently, studies relying on these approaches may fail to identify all POD cases, underestimate the true incidence, and dilute the correlation between GA and risk of POD.
With accumulating evidence suggesting the feasibility of TAVR as a relatively low-risk therapeutic alternative to conventional surgery for patients diagnosed with severe symptomatic aortic valve stenosis60,61,62, TAVR is expected to gain increasing popularity among those who are at high risk for surgical repair. Although GA may be preferred over sedation/local anesthesia due to its ability to facilitate timely surgical correction and enable real-time monitoring through transesophageal echocardiography during the early learning curve development for TAVR, sedation/local anesthesia may be an optimal choice for patients receiving TAVR based on the finding of the current meta-analysis, especially for those at high risk of POD (e.g., anticipated prolonged mechanical ventilation). On the other hand, if GA is indicated (e.g., at the early stage of the learning curve), implementation of appropriate preventive strategies may be indicated. Non-pharmacological strategies including multicomponent interventions, avoidance of peri-operative benzodiazepines, minimizing precipitating events, using processed electroencephalogram monitoring (e.g., bispectral index) to guide anesthetics titration may be beneficial63,64,65, while strategies for pharmacological prophylaxis such as the use of antipsychotics and peri-procedural dexmedetomidine as well as optimizing postoperative pain control have also been reported63,64,66. Besides, a previous meta-analysis of six studies reported that perioperative melatonin, a natural hormone known to regulate sleep–wake cycles, could be effective for preventing POD in older patients66.
There were several limitations in the current study. First, because we mostly included retrospective studies, the causality relationship between GA exposure and POD risk could not be definitely established. Second, although confounding factors such as peri-procedural hypotension or history of cognitive impairment may contribute to this cognitive dysfunction, they were not investigated due to unavailable information. Third, the effects of other predisposing factors including advanced age, gender, and technique of TAVR, which have been well-described in a recent meta-analysis11, were not investigated in the present study. Third, our results, which were derived mostly from patients aged more than 80 years, may not be extrapolated to younger populations. Finally, we did not evaluate the long-term influence of POD as this information was not available in most studies.
Conclusion
Our analysis of 10,678 patients over 75 years of age receiving TAVR showed an elevated risk of postoperative delirium following general anesthesia exposure with a low risk of publication bias and consistency of result on sensitivity analysis. The inclusion of mostly observational studies in the current study warrants further randomized controlled clinical investigations to support our findings and to elucidate the efficacy of possible preventive strategies (e.g., dexmedetomidine administration) against postoperative delirium in this clinical setting.
Data availability
The original contributions presented in this study are included in this article/Supplementary material, further inquiries can be directed to the corresponding author.
References
Vahanian, A. et al. Guidelines on the management of valvular heart disease (version 2012). Eur. Heart J. 33, 2451–2496 (2012).
Abdel-Wahab, M., El-Mawardy, M. & Richardt, G. Update on transcatheter aortic valve replacement. Trends Cardiovasc. Med. 25, 154–161 (2015).
Agarwal, S. et al. Transcatheter aortic valve replacement: Current perspectives and future implications. Heart (Br. Cardiac. Soc.) 101, 169–177 (2015).
Neuburger, P. J. & Patel, P. A. Anesthetic techniques in transcatheter aortic valve replacement and the evolving role of the anesthesiologist. J. Cardiothorac. Vasc. Anesth. 31, 2175–2182 (2017).
Tse, L. et al. Postoperative delirium following transcatheter aortic valve implantation: A historical cohort study. Can. J. Anaesth. 62, 22–30 (2015).
Strike, E. et al. Postoperative pain management strategies and delirium after transapical aortic valve replacement: A randomized controlled trial. J. Cardiothorac. Vasc. Anesth. 33, 1668–1672 (2019).
Deiner, S. & Silverstein, J. H. Postoperative delirium and cognitive dysfunction. Br. J. Anaesth. 103(Suppl 1), i41–i46 (2009).
Curtis, M. S., Forman, N. A., Donovan, A. L. & Whitlock, E. L. Postoperative delirium: Why, what, and how to confront it at your institution. Curr. Opin. Anaesthesiol. 33, 668–673 (2020).
Bilotta, F., Lauretta, M. P., Borozdina, A., Mizikov, V. M. & Rosa, G. Postoperative delirium: Risk factors, diagnosis and perioperative care. Minerva Anestesiol. 79, 1066–1076 (2013).
Abawi, M. et al. Postoperative delirium in individuals undergoing transcatheter aortic valve replacement: A systematic review and meta-analysis. J. Am. Geriatr. Soc. 66, 2417–2424 (2018).
Ma, X. et al. Postoperative delirium after transcatheter aortic valve replacement: An updated systematic review and meta-analysis. J. Am. Geriatr. Soc. 71(2), 646–660 (2023).
Ashley, K. E. & Hillegass, W. B. Costs of postoperative delirium with transcatheter aortic valve replacement: Improved yet still present. Catheter. Cardiovasc. Interv. 93, 1137 (2019).
Potter, B. J., Thompson, C., Green, P. & Clancy, S. Incremental cost and length of stay associated with postprocedure delirium in transcatheter and surgical aortic valve replacement patients in the United States. Catheter. Cardiovasc. Interv. 93, 1132–1136 (2019).
Abawi, M. et al. Incidence, predictive factors, and effect of delirium after transcatheter aortic valve replacement. JACC Cardiovasc. Interv. 9, 160–168 (2016).
Mauri, V. et al. Incidence, risk factors and impact on long-term outcome of postoperative delirium after transcatheter aortic valve replacement. Front. Cardiovasc. Med. 8, 645724 (2021).
Huded, C. P. et al. The impact of delirium on healthcare utilization and survival after transcatheter aortic valve replacement. Catheter. Cardiovasc. Interv. 89, 1286–1291 (2017).
Maniar, H. S. et al. Delirium after surgical and transcatheter aortic valve replacement is associated with increased mortality. J. Thorac. Cardiovasc. Surg. 151, 815–23.e2 (2016).
Ahn, E. J. et al. Comparison of general anaesthesia and regional anaesthesia in terms of mortality and complications in elderly patients with hip fracture: A nationwide population-based study. BMJ Open 9, e029245 (2019).
Chen, D. X. et al. Perioperative outcomes in geriatric patients undergoing hip fracture surgery with different anesthesia techniques: A systematic review and meta-analysis. Medicine 98, e18220 (2019).
Bhushan, S., Huang, X., Duan, Y. & Xiao, Z. The impact of regional versus general anesthesia on postoperative neurocognitive outcomes in elderly patients undergoing hip fracture surgery: A systematic review and meta-analysis. Int. J. Surg. (Lond. Engl.) 105, 106854 (2022).
Wang, J. et al. Risk factors contributing to postoperative delirium in geriatric patients postorthopedic surgery. Asia Pac. Psychiatry. 7, 375–382 (2015).
Slor, C. J. et al. Anesthesia and postoperative delirium in older adults undergoing hip surgery. J. Am. Geriatr. Soc. 59, 1313–1319 (2011).
Weinstein, S. et al. Postoperative delirium in total knee and hip arthroplasty patients: A study of perioperative modifiable risk factors. Br. J. Anaesth. 120, 999–1008 (2018).
Li, T. et al. Effect of regional vs general anesthesia on incidence of postoperative delirium in older patients undergoing hip fracture surgery: the RAGA Randomized Trial. JAMA 327, 50–58 (2022).
Brown, C. H. et al. Spinal anesthesia with targeted sedation based on bispectral index values compared with general anesthesia with masked bispectral index values to reduce delirium: The SHARP Randomized Controlled Trial. Anesthesiology 135, 992–1003 (2021).
Wesselink, E. M. et al. Intraoperative hypotension and delirium among older adults undergoing transcatheter aortic valve replacement. J. Am. Geriatr. Soc. 69, 3177–3185 (2021).
Goudzwaard, J. A. et al. Incidence, determinants and consequences of delirium in older patients after transcatheter aortic valve implantation. Age Ageing. 49, 389–394 (2020).
Thiele, H. et al. General versus local anesthesia with conscious sedation in transcatheter aortic valve implantation: The randomized SOLVE-TAVI Trial. Circulation 142, 1437–1447 (2020).
Hung, K.-C. et al. The impact of esophageal device insertion on cuff pressure of endotracheal tube: A literature review and meta-analysis. Sci. Rep. 12, 18192 (2022).
Lin, H.-M. et al. Impact of cognitive behavior therapy on osteoarthritis-associated pain, insomnia, depression, fatigue, and physical function in patients with knee/hip osteoarthritis: A systematic review and meta-analysis of randomized controlled trials. Front. Med. 9, 1083095 (2022).
Lee, S. W., Lee, S. & Hahm, K. D. Postoperative pulmonary complications after transcatheter aortic valve implantation under monitored anesthesia care versus general anesthesia: retrospective analysis at a single large volume center. J. Clin. Med. 10, 5365 (2021).
Musuku, S. R. et al. Outcomes of transfemoral transcatheter aortic valve replacement performed with general anesthesia using a supraglottic airway versus monitored anesthesia care. J. Cardiothorac. Vasc. Anesth. 35, 1760–1768 (2021).
Mosleh, W. et al. Propensity matched analysis comparing conscious sedation versus general anesthesia in transcatheter aortic valve implantation. Am J Cardiol. 124, 70–77 (2019).
He, W. et al. Bispectral index-guided sedation in transfemoral transcatheter aortic valve implantation: A retrospective control study. J. Zhejiang Univ. Sci. B 18, 353–359 (2017).
Gauthier, C. et al. Mid-term survival after transcatheter aortic valve implantation: Results with respect to the anesthetic management and to the access route (transfemoral versus transapical). Ann. Cardiac. Anaest. 18, 343–351 (2015).
Renner, J. et al. A retrospective study of conscious sedation versus general anaesthesia in patients scheduled for transfemoral aortic valve implantation: A single center experience. Health Sci. Rep. 2(1), e95 (2019).
Bagienski, M. et al. Incidence of postoperative delirium and its impact on outcomes after transcatheter aortic valve implantation. Am. J. Cardiol. 120, 1187–1192 (2017).
Maier, A. et al. A logistic regression analysis comparing minimalistic approach and intubation anaesthesia in patients undergoing transfemoral transcatheter aortic valve replacement. PloS one. 15, e0227345 (2020).
Kalyoncuoğlu, M., Biter, H., Durmuş, G., Baştan, B. & Can, M. M. C-reactive protein to albumin ratio as a novel inflammatory biomarker for postoperative delirium in patients undergoing transcatheter aortic valve replacement. Med. Bull. Haseki/Haseki Tip Bulteni. 58, 183–192 (2020).
Luque, T. et al. Impact of delirium in acute cardiac care unit after transcatheter aortic valve replacement. Int. J. Cardiol. 330, 164–170 (2021).
Khan, M. M. et al. The value of screening for cognition, depression, and frailty in patients referred for TAVI. Clin. Interv. Aging 14, 841–848 (2019).
Husser, O. et al. Conscious sedation versus general anesthesia in transcatheter aortic valve replacement: The German Aortic Valve Registry. JACC Cardiovasc. Interv. 11(6), 567–578 (2018).
Bitsch, M., Foss, N., Kristensen, B. & Kehlet, H. Pathogenesis of and management strategies for postoperative delirium after hip fracture: A review. Acta Orthop. Scand. 75, 378–389 (2004).
Neuman, M. D. et al. Spinal anesthesia or general anesthesia for hip surgery in older adults. N. Engl. J. Med. 385, 2025–2035 (2021).
Yang, J. S., Lee, J. J., Kwon, Y. S., Kim, J. H. & Sohn, J. H. Preoperative inflammatory markers and the risk of postoperative delirium in patients undergoing lumbar spinal fusion surgery. J. Clin. Med. 11, 4085 (2022).
Pasqui, E. et al. The Predictive role of inflammatory biochemical markers in post-operative delirium after vascular surgery procedures. Vasc. Health Risk Manag. 18, 747–756 (2022).
Kotfis, K., Ślozowska, J., Safranow, K., Szylińska, A. & Listewnik, M. The practical use of white cell inflammatory biomarkers in prediction of postoperative delirium after cardiac surgery. Brain Sci. 9, 308 (2019).
Liu, X., Yu, Y. & Zhu, S. Inflammatory markers in postoperative delirium (POD) and cognitive dysfunction (POCD): A meta-analysis of observational studies. PloS one. 13, e0195659 (2018).
Ni Choileain, N. & Redmond, H. P. Cell response to surgery. Arch. Surg. (Chicago, IL: 1960) 141, 1132–1140 (2006).
Brattinga, B. et al. The association between the inflammatory response following surgery and post-operative delirium in older oncological patients: A prospective cohort study. Age Ageing 51, afab237 (2022).
Subramaniyan, S. & Terrando, N. Neuroinflammation and perioperative neurocognitive disorders. Anesth. Analg. 128, 781–788 (2019).
Ransohoff, R. M. How neuroinflammation contributes to neurodegeneration. Science (New York, NY). 353, 777–783 (2016).
Robinson, T. N. et al. Postoperative delirium in the elderly: risk factors and outcomes. Ann. Surg. 249, 173–178 (2009).
Hung, K. C. et al. Conscious sedation/monitored anesthesia care versus general anesthesia in patients undergoing transcatheter aortic valve replacement: A meta-analysis. Front. Cardiovasc. Med. 9, 1099959 (2022).
Wachtendorf, L. J. et al. Association between intraoperative arterial hypotension and postoperative delirium after noncardiac surgery: A retrospective multicenter cohort study. Anesth. Analg. 134, 822–833 (2022).
Maheshwari, K. et al. Association between perioperative hypotension and delirium in postoperative critically ill patients: A retrospective cohort analysis. Anesth. Analg. 130, 636–643 (2020).
Ushio, M., Egi, M., Fujimoto, D., Obata, N. & Mizobuchi, S. Timing, threshold, and duration of intraoperative hypotension in cardiac surgery: their associations with postoperative delirium. J. Cardiothorac. Vasc. Anesth. 36, 4062–4069 (2022).
Kotfis, K., Ślozowska, J., Listewnik, M., Szylińska, A. & Rotter, I. The impact of acute kidney injury in the perioperative period on the incidence of postoperative delirium in patients undergoing coronary artery bypass grafting—observational cohort study. Int. J. Environ. Res. Public Health 17, 1440 (2020).
Chen, H., Mo, L., Hu, H., Ou, Y. & Luo, J. Risk factors of postoperative delirium after cardiac surgery: A meta-analysis. J. Cardiothorac. Surg. 16, 113 (2021).
Howard, C. et al. TAVI and the future of aortic valve replacement. J. Cardiac. Surg. 34, 1577–1590 (2019).
Waksman, R. et al. Transcatheter aortic valve replacement in low-risk patients with symptomatic severe aortic stenosis. J. Am. Coll. Cardiol. 72, 2095–2105 (2018).
Waksman, R. et al. TAVR in low-risk patients: 1-year results from the LRT trial. JACC Cardiovasc. Interv. 12, 901–907 (2019).
Janssen, T. L. et al. Prevention of postoperative delirium in elderly patients planned for elective surgery: Systematic review and meta-analysis. Clin. Interv. Aging. 14, 1095–1117 (2019).
Hughes, C. G. et al. American society for enhanced recovery and perioperative quality initiative joint consensus statement on postoperative delirium prevention. Anesth. Analg. 130, 1572 (2020).
Swarbrick, C. & Partridge, J. Evidence-based strategies to reduce the incidence of postoperative delirium: A narrative review. Anaesthesia 77, 92–101 (2022).
Campbell, A. M. et al. Melatonin for the prevention of postoperative delirium in older adults: A systematic review and meta-analysis. BMC Geriatr. 19, 272 (2019).
Funding
This research was funded by Chi Mei Medical Center, Tainan, Taiwan, grant number CMNDMC11105. The APC was funded by CMNDMC11105.
Author information
Authors and Affiliations
Contributions
Conceptualization, C.-C.K. and K.-C.H.; methodology, Y.-P.C.; software, C.-C.L.; formal analysis, W.-J.C. and J.-Y.W.; data curation, J.-Y.W. and Y.-Y.L.; writing—original draft preparation, C.-C.K., K.-C.H., C.-K.S., and Y.-Y.L.; writing—review and editing, K.-C.H. and C.-K.S. All authors have read and agreed to the published version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ko, CC., Hung, KC., Chang, YP. et al. Association of general anesthesia exposure with risk of postoperative delirium in patients receiving transcatheter aortic valve replacement: a meta-analysis and systematic review. Sci Rep 13, 16241 (2023). https://doi.org/10.1038/s41598-023-43548-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-43548-2
This article is cited by
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
