
Abstract
Social buffering, a phenomenon where social presence can reduce anxiety and fear-related autonomic responses, has been studied in numerous laboratory settings. The results suggest that the familiarity of the interaction partner influences social buffering while also providing some evidence for gender effects. In the laboratory, however, it is difficult to mimic the complexity of real-life social interactions. Consequently, the social modulation of anxiety and related autonomic responses in everyday life remains poorly understood. We used smartphone-based Ecological Momentary Assessment (EMA) combined with wearable electrocardiogram sensors to investigate how everyday-life social interactions affect state anxiety and related cardiac changes in women and men. On five consecutive days, 96 healthy young participants (53% women) answered up to six EMA surveys per day, indicating characteristics of their most recent social interaction and the respective interaction partner(s). In women, our results showed lower heart rate in the presence of a male interaction partner. Men showed the same effect with female interaction partners. Moreover, only women showed decreased heart rate and increased heart rate variability with increasing interaction partner familiarity. These findings specify the conditions under which social interactions reduce anxiety-related responses in women and men.
Similar content being viewed by others


Introduction
Animal and human studies have shown that the mere presence of a conspecific can reduce physiological stress and fear responses1,2, a phenomenon called social buffering3,4. So far, social buffering has mostly been investigated in the laboratory. In human studies, participants typically experience a stress or anxiety-inducing situation (e.g., pain induction, public speech) alone or in the presence of another person. Some studies extend the social aspect, for instance by modulating the familiarity (e.g., stranger versus friend) or affiliative behaviour (e.g., social support versus no support) of the interaction partner1,5. Social buffering effects are inferred from reductions of reported anxiety or adaptive changes in autonomic responses caused by the interaction partner’s presence or behaviour6,7. For example, the presence of social support has been linked to reduced heart rate (HR)8, indicating lower acute (social) stress9,10. In contrast, a lack of social contact (i.e., social isolation) has been associated with lower heart rate variability (HRV)11, reflecting diminished behavioural and emotion-regulatory adaptability12,13.
The social buffering effects observed in the laboratory were modulated by various factors, including the gender of the participant as well as the familiarity and gender of their interaction partner. Regarding familiarity, findings suggest stronger social buffering effects in the presence of more familiar interaction partners14,15. Regarding the participant’s gender, previous studies imply that men and women experience certain social situations differently. In general, self-reported anxiety tends to be higher in women16,17 which is paralleled by stronger physiological reactions such as higher HR18,19 and lower HRV20 in anxiety-inducing situations. Findings concerning gender effects in social buffering of anxiety are mixed, however. Some studies reported stronger effects in women compared to men3,21, while other studies showed the opposite22,23. Yet other studies found no gender differences in general anxiety levels24,25 or social buffering effects26,27.
Regarding the gender of the interaction partner, both men and women showed reduced autonomic responses (systolic blood pressure [BP]) when receiving social support from female but not male social partners19. Similarly, other laboratory settings with anxiety-related autonomic measurements revealed social buffering effects in female but not male dyads, e.g., on skin conductance responses3. Challenging this result, other studies reported reduced cardiovascular reactivity (systolic BP, HR) in women in the presence of their romantic partner28 or when receiving social support from a male friend29. Yet another study showed reduced cortisol levels in men in the presence of their (female) romantic partner, but not in women in the presence of their (male) romantic partner22. Finally, a meta-analysis revealed no gender differences in the effect of social stress induction on HRV. In both genders, dyadic tasks designed to elicit negative affect decreased HRV, whereas dyadic tasks eliciting positive or no particular valence had no significant influence26.
Overall, findings from previous laboratory studies suggest that social presence and contact, particularly with more familiar persons, can reduce anxiety on the subjective and autonomic level, and that the gender of the participants and the interaction partner might play a role. However, the findings are inconsistent and were mainly observed in the laboratory. Capturing the complexity of everyday-life social interactions is difficult in the laboratory, for example, regarding the inclusion of all possible combinations of same- and mixed-gender interaction partners at varying quantities and familiarity levels. Thus, it remains unclear whether social buffering effects found in the laboratory transfer to social situations in everyday life. Here, we used smartphone-based Ecological Momentary Assessment (EMA) with wearable electrocardiogram (ECG) sensors to investigate how everyday-life social interactions affect subjective state anxiety and related cardiovascular changes depending on characteristics of both the participants and their interaction partners. EMA encompasses repeated, real-time subjective and/or physiological assessments of people’s behaviour and experiences in a naturalistic setting. It can integrate multiple within- and between-subject variables simultaneously, thereby further minimizing biases and measurement restrictions associated with laboratory settings. As such, EMA facilitates the economic testing of laboratory findings’ ecological validity in everyday life30,31,32.
Previous studies successfully applied EMA to investigate changes of autonomic responses and started to uncover the effects of important social factors like familiarity in everyday life. In accordance with decreased state anxiety in response to social support from familiar versus unfamiliar persons observed during psychosocial stress in the laboratory33, an EMA study revealed lower self-reported anxiety levels when spending time with familiar versus less familiar social partners, particularly in socially anxious individuals34. Similar relations were found between interaction partner familiarity and state social interaction anxiety32, an anxiety measure closely related to higher state anxiety levels35. Other EMA research has revealed reduced cardiovascular responses (i.e., ambulatory BP) in healthy participants when interacting with family members or romantic partners compared to unfamiliar partners36, and increased HRV with familiar interaction partners (family, romantic partner) compared to strangers in shy individuals37. These studies provided first insights into the effect of social factors like familiarity in everyday-life settings but did not consider the gender of the participants and interaction partners. Extending previous EMA work, we designed an EMA study to investigate how the gender of the participant and the interaction partner affect social buffering of state anxiety and related autonomic responses in everyday life, particularly regarding the effect of familiarity.
We hypothesized that participants would benefit from more familiar interaction partners which would be represented in decreased state anxiety32 and HR as well as increased HRV36,37, and tested how these effects were influenced by the gender of the participants and their interaction partners. We assumed that women would show higher HR and lower HRV than men during everyday-life social interactions18,20. However, based on previous findings3,19,22, we additionally hypothesized that men and women would show more adaptive subjective and cardiovascular responses (i.e., lower state anxiety, lower HR, higher HRV) in the presence of female interaction partners. Alternatively, we expected opposite-gender social buffering effects28,29 or no effects of the interaction partners’ gender26.
Methods
Participants
122 healthy men and women aged 18 to 35 years participated in the study (two dropouts). After data curation, the final sample consisted of 96 participants (53.1% female; mean age = 25.17, SD = 4.12) with a total of 1 536 observations. Exclusion criteria included current pregnancy or lactation period, cardiovascular illnesses, chronic neurological disorders, acute psychiatric disorders, other severe medical illnesses, psychotropic medication, and visual and motoric impairments. We excluded nine participants after visual inspection of ECG data due to frequent artefacts and 15 participants with invalid baseline measurements. Invalid data were mainly caused by insufficient quality of ECG chest belts. A sensitivity analysis using G*Power software (version 3.1.9.7)38 revealed that the final sample size of N = 96 had a statistical power of > 0.80 with a 5% type I error rate to detect small to medium effect sizes (f2 = 0.08) in a multiple regression model with 15 predictors (comparable to our models, see below). Given that the within-subject effects have larger level-1 sample sizes (equivalent to the number of observations nested within persons), we expected to have sufficient power to detect small effects. All participants provided written informed consent. The study protocol was approved by the ethics committee of the medical faculty of the University of Würzburg (vote #180/20) and complies with the Declaration of Helsinki.
Procedure
Participants were invited to a pre-session. A chest belt with ECG sensor was attached and the participant’s schedule for the five EMA measurement days was enquired to adjust the 12-h measurement time windows, starting one hour after the usual wake-up time. Participants filled in sociodemographic and clinical questionnaires. During the subsequent 5-min baseline measurement, the participants sat upright facing a 16:9 computer screen at approx. 140 cm distance. They were asked to relax while watching an audio-visual clip of an aquarium. Afterwards, the participants practiced the correct use of the ECG belt and the EMA questionnaire application (app) delivered on a study smartphone. Supervised by the experimenter, they answered the EMA survey in two imaginary situations (social, non-social) before receiving the study material. On five consecutive days, participants carried the smartphone with them while wearing the ambulatory ECG sensor within the 12-h time windows. Within three days after the final assessment, they returned to the laboratory, filled in questionnaires, and received a financial compensation. An overview of the study procedure is displayed in Fig. 1.

Study procedure. ECG, Electrocardiogram; EMA, Ecological Momentary Assessment.
Measures
Trait questionnaires
Participants were screened for depression using the 15-item short form of the Center for Epidemiologic Studies Depression Scale (German: “Allgemeine Depressionsskala—Kurzform”, ADS-K)39. In addition, we assessed participants’ trait anxiety and social interaction anxiety using the trait anxiety subscale of the state-trait anxiety inventory (STAI)40 and the social interaction anxiety scale (SIAS)41, respectively.
EMA survey items
EMA surveys were delivered with the movisensXS app (Movisens GmbH) on an android smartphone. State anxiety was assessed with a 10-item short form of the STAI state anxiety subscale42 rated on a Likert scale from 1 (“not at all”) to 8 (“totally”). Participants indicated the time of their most recent social interaction (“now”, “within the last 30 min”, “more than 30 min ago”). For social interactions ≤ 30 min ago, they answered the social interaction questionnaire (for a detailed item list, see Table S1). Otherwise, they answered a similarly structured activity questionnaire to prevent avoidance behaviour due to time savings (see Table S2). The social interaction questionnaire first assessed the type (“direct contact”, “telephone call”, “e-mail/letter”, “SMS”, “social media”; “private”, “job-related”), the approximate start and duration of the social interaction (slider scales with three anchors: “ < 1 min”, “15 min”, “ > 30 min”), and the quantity (“1” to “5 or more”) and gender (“female”, “male”, “mixed”) of the interaction partners. The familiarity of the interaction partners (“I know the other person/one of the other persons well.”) was assessed continuously with a Likert scale ranging from 1 (“not at all”) to 8 (“very”)43,44, given that the categorical measurement of familiarity in previous studies may overlook relations like estranged family members or familiar long-time colleagues. State social interaction anxiety was averaged from two items (“I worried about what the other person(s) thought of me”, “I was worried that I would say or do the wrong things”) rated on a Likert scale from 1 (“not at all”) to 9 ("very")45,46. We assessed the pleasantness of the interaction (“How (un)pleasant was the interaction?”) on an 8-point Likert scale ranging from 1 (“very unpleasant”) to 8 (“very pleasant”)47. The final screen assessed ECG control variables (e.g., consumption of caffeine/nicotine/alcohol during the last hour)48,49.
Autonomic measures
HR and HRV were measured continuously with an ambulatory ECG, i.e., the movisens EcgMove4 sensor (Movisens GmbH, Karlsruhe, Germany). HR describes the number of heartbeats in beats per minute (bpm). In the presence of a stressor, HR is increased by vagal withdrawal and sympathetic activation9,12. HRV is a quantitative marker of autonomic nervous system activity influenced by both sympathetic and parasympathetic activity50,51. It describes the fluctuation in the time intervals between adjacent heartbeats, which show less linearity and more spatial and temporal complexity in healthy individuals (i.e., higher HRV)52,53. Higher HRV relates to higher skills, engagement, and stress regulation in social situations13,54, including the adaptive regulation of HR55. This study’s HRV measure is the root mean square of successive differences between heartbeats (RMSSD) measured in ms. RMSSD estimates vagal cardiac control and reflects short-term parasympathetic variations. There is support that time-domain HRV measures like RMSSD show higher robustness to (motion) artefacts than frequency-domain HRV measures56. RMSSD is an appropriate measure for long- and short-term time windows57 and EMA research58,59. For comprehensive guidelines, see50 or48.
The ECG sensor was attached to a chest belt worn at the base of the sternum with direct skin contact of two dry electrodes. Participants were instructed to clean the skin beneath the electrodes with alcohol pads (70% isopropyl alcohol) prior to attachment. The sensor collected single channel ECG data (resolution = 12 bits, sampling rate = 1 204 Hz). Participants were asked not to consume a heavy meal, coffee, alcohol or tobacco, and to only drink low amounts of water in the two hours prior to the pre-session48. All baseline ECG measurements were collected between 12 and 6 pm.
Data analysis
EMA survey data curation
We screened the EMA survey data for invalid or incoherent data. Continuous within-person variables were person-centred and continuous between-person variables were grand mean-centred60. We categorized the social interaction type into “direct” or “virtual” and transformed consumption indications into binary variables (“yes”, “no”). Finally, we added a binary variable for the interaction partner quantity (“1”, “2 or more”) to account for the constitutional absence of mixed-gender social interactions with one person only.
ECG data curation and heart rate variability calculation
After visual inspection of ECG data, we applied the movisens DataAnalyzer software (version 1.13.8) to convert the ECG signals into HRV indices. The software uses an automated algorithm to detect artefacts. Its output is based on minute-by-minute calculations derived from 2-min segments. The DataAnalyzer detects R-peaks61, marks signal amplitude and number of zero crossings per s outside a normal physiological range as artefacts, and filters invalid R-peaks and artefacts62 (for more details, see supplement). Bodily movement (sampling rate = 64 Hz) was transformed into 1-min epochs.
ECG and EMA data were aligned and imported into R (version 4.2.0). We rounded ECG data to whole-minute values, excluded ECG segments labelled as invalid, and calculated mean scores for HR and RMSSD at baseline (first minute excluded). We calculated separate outlier detections for baseline and EMA values of HR and RMSSD. Values outside the upper and lower quartile by at least 1.5 times the interquartile range were removed63. 73.4% of rows had valid HR and RMSSD. We extracted mean HR and RMSSD values for each social interaction (time retrieved from slider scales, transformed to 1-min-intervals; first and last segment of time window excluded). The survey prompt marked the end of ongoing social interactions. We removed social interactions shorter than 60 s. A natural logarithmic transformation was performed to correct for skewness (RMSSD). The final 96 participants provided a total of 1 536 valid observations, i.e., 16 social interaction assessments on average (SD = 5.08, range = 5–27).
Statistical analysis
To test our hypotheses, we calculated three linear mixed models with participant as random intercept and state anxiety, HR, and RMSSD as dependent variables, respectively, using the ‘lme4’ package64. Differences in main variables between male and female participants were calculated using t-tests. All linear mixed models were tested against basic models without interactions. Model significance was calculated with the ‘lmerTest’ package65, applying Satterthwaite’s method to estimate degrees of freedom and p-values. We assessed multicollinearity within the models by calculating variance inflation factors (VIF) with the ‘performance’ package66. The ‘sjPlot’ package provided ICC and R267. We conducted simple slope analyses for significant interactions with continuous variables using the ‘interactions’ package68 and post hoc comparisons using pairwise t-tests (Bonferroni-corrected) for interactions with categorical variables.
First, as a manipulation check for the expected relationship between subjective anxiety and autonomic responses, we created two simple models with state anxiety as outcome and HR or RMSSD during EMA as predictor. We added essential autonomic control variables (caffeine, nicotine, alcohol, acceleration, baseline; see below).
Second, we created the main models. The state anxiety, HR, and RMSSD models included the predictors participant’s gender (gender participant; two levels: female, male), familiarity (familiarity IP; centred within [cw]) and gender of the interaction partner (gender IP; three levels: female, male, mixed; reference: female), state social interaction anxiety (state SI anxiety; cw), trait social interaction anxiety (SIAS; centred between [cb]), and social interaction type (SI type; two levels: direct, virtual). HR and RMSSD are sensitive to a number of potential confounds48,49,56. To enhance model comparability, we therefore included the following covariates into all three models: duration of the social interaction (SI duration; measured in s, cw), interaction partner quantity (quantity IP; two levels: 1, 2 or more), and consumption of caffeine, nicotine, and alcohol within the last hour (two levels each: yes, no). For HR and RMSSD, we additionally included movement acceleration (accel; mean, cw) as an indicator of physical activity, a factor which can enhance HR49 and interfere with vagal cardiac control as reflected in HRV69. To account for individual differences in autonomic baseline levels, the HR and RMSSD models further included the covariate HR at baseline (cb) and RMSSD at baseline (cb), respectively, as recommended for ECG assessments48. All three models originally included two interactions: gender participant x gender IP, and gender participant x familiarity IP. For state anxiety, the interaction effects were non-significant, and model comparison with likelihood ratio tests indicated no difference in model fit with or without the interactions (p = 0.734). Therefore, we chose the basic state anxiety model as main model. For the HR and RMSSD models, model comparison indicated better model fit of the interaction models (both ps’ < 0.001), which were therefore chosen as main HR and RMSSD models.
Finally, we compared the main models to more complex (and less parsimonious) models. First, we added age (cb) and depression scores (ADS-K; cb) as additional control variables. Second, we integrated social interactions with romantic partners (two levels: yes, no) as potential confounding variable for gender IP effects. Third, we tested two additional control interactions (SI type x accel, gender IP x quantity IP) for the autonomic models. Age and ADS-K improved model fit for the anxiety model and were therefore added to the final anxiety model. There were no other significant improvements in model fit (all ps' > 0.05) and thus no other changes. Note that we also conducted exploratory analyses to test for moderating effects of social interaction pleasantness on familiarity IP47,70 and of SIAS on familiarity IP41 and SI type71. The interactions remained non-significant in the state anxiety model (all ps’ > 0.484). For HR and RMSSD, the interactions also remained non-significant, with the interaction between pleasantness and familiarity showing a trend towards significance for HR (β = 0.15, SE = 0.08, p = 0.056) and RMSSD (β = − 0.01, SE = 0.00, p = 0.074; all other ps’ > 0.621). However, the inclusion of the interactions did not improve model fit (HR: p = 0.393; RMSSD: p = 0.484) and was therefore discarded.
Ethical standards
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008.
Results
Sample characteristics
The observations consisted of 78.4% direct and 21.6% virtual social interactions. 40.2% of social interactions took place with female, 29.5% with male, and 30.3% with mixed interaction partners. Overall, 42.5% of social interactions included two or more interaction partners (16.9% female, 12.1% male, 71.0% mixed). 57.5% of one-person social interactions were with female interaction partners (see Supplementary Table S5 for additional characteristics of social interactions). Sample characteristics and gender differences are reported in Table 1 (see Table S6 for correlations between HR, RMSSD, and trait questionnaires). Compared to men, women showed higher mean levels of HR during social interactions. Women also tended to show higher HR during baseline and higher depression scores (for numeric values, see Table 1).
State anxiety
The manipulation check confirmed a relationship between subjective and autonomic indicators of anxiety. Higher state anxiety correlated with higher HR during social interactions (β = 0.17, p < 0.001) but not with changes in RMSSD (β = − 1.20, p < 0.184).
Details of the results for the state anxiety model are presented in Table 2 (left column). VIF (all ≤ 2.39) were in an acceptable range72. There was a main effect of familiarity IP (β = − 0.94, p < 0.001; see Fig. 2), indicating lower state anxiety after interacting with more familiar interaction partners.

Main effect of familiarity (centred within, cw) on state anxiety. Shaded errors indicate 95% confidence intervals.
In addition, lower state anxiety was related to lower state SI anxiety (β = 1.96, p < 0.001), and state anxiety was lower during direct compared to virtual social interactions (χ2(1) = 8.65, p = 0.003). On the between-person level, state anxiety increased with age (β = 0.23, p = 0.014), trait SI anxiety (β = 0.56, p = 0.021), and depression scores (β = 1.20, p < 0.001). There were no significant gender effects.
Heart rate
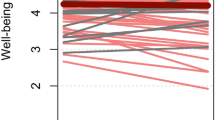
Details of the results for the HR model are presented in Table 2 (middle column). VIF (all ≤ 7.45) were in an acceptable range72. The HR results showed a significant main effect of state SI anxiety (β = 0.49, p = 0.002), representing higher HR with higher state social interaction anxiety. In addition, the main effect of SI type (χ2(1) = 19.92, p < 0.001) indicated lower HR during virtual versus direct social interactions. The main effect of the participant’s gender (χ2(1) = 16.61, p < 0.001) reflected higher HR in women. The participant’s gender also interacted with familiarity IP (χ2(1) = 12.60, p < 0.001; Fig. 3A). Follow-up analyses for the simple slopes of familiarity for female and male participants revealed a negative slope for women (β = − 0.54, p < 0.001) but no effect for men (β = 0.24, p = 0.163).

Prediction of HR (A) and RMSSD (ln; B) by familiarity x gender participant, i.e., in female (turquoise) and male (red) participants. Shaded errors indicate 95% confidence intervals. bpm, Beats per min; cw, Centred within.
Lastly, HR was affected by the interaction partners’ gender (χ2(2) = 11.26, p = 0.004), but gender IP also interacted with the participant’s gender (χ2(2) = 18.30, p < 0.001; Fig. 4A). Pairwise t-tests revealed higher HR in women when interacting with female versus male IP (t(1514) = 2.60, p = 0.005). In contrast, men showed lower HR when interacting with female versus mixed IP (t(1475) = − 2.83, p = 0.015) and tended to show lower HR when interacting with female versus male IP (t(1507) = − 2.13, p = 0.070). Comparing male and female participants, men showed lower HR than women when interacting with female IP (t(131) = − 5.44, p < 0.001).

HR (A) and RMSSD (B) in female (turquoise) and male (red) participants in social interactions with female, male, and mixed interaction partners (IP). Dots within boxplots represent group mean, lines represent medians. bpm, Beats per min.
Heart rate variability
Details of the results for the RMSSD (i.e., HRV) model are presented in Table 2 (right column). VIF (all ≤ 7.45) were in an acceptable range72. In accordance with the state anxiety model, RMSSD was higher (i.e., more adaptive) when participants interacted with more familiar interaction partners (β = − 0.03, p < 0.001). In accordance with the HR results, RMSSD was higher during virtual versus direct social interactions (χ2(1) = 8.62, p = 0.003), and a marginal main effect for the participant’s gender (β = − 0.10, p = 0.071) indicated a tendency towards lower RMSSD in women. The participant’s gender also interacted with familiarity IP (χ2(1) = 25.99, p < 0.001; Fig. 3B). Simple slope analyses revealed a positive slope for women (β = 0.02, p = 0.004) but a negative slope for men (β = − 0.03, p < 0.001).
Due to the main effects of autonomic baseline values and gender participant in the HR and RMSSD models, we additionally tested if baseline levels affected the gender participant x familiarity IP effects by testing the main models against a model with an additional three-way interaction (gender participant x familiarity IP x baseline). In the HR model, this interaction was neither significant (χ2(1) = 0.04, p = 0.833) nor improved model performance (p = 0.691). In the RMSSD model, the three-way interaction was significant (χ2(1) = 9.76, p = 0.002; see Fig. 5) and improved model fit (p = 0.005). Separate simple slope analyses in the male and female subsample revealed a negative slope for men with low baseline RMSSD levels (β = − 0.06, p = 0.010), indicating that the gender-specific negative relationship between familiarity and RMSSD in men was limited to those with low baseline RMSSD, while the positive relation in women was independent of baseline RMSSD.

Prediction of RMSSD by familiarity in male (left panel) and female (right panel) participants at low (-1SD), medium, and high (+ 1SD) levels of baseline RMSSD. cb, Centred between; cw, Centred within.
Lastly, as for HR, gender IP interacted with the participant’s gender (χ2(2) = 9.54, p = 0.008; Fig. 4B). Pairwise t-tests revealed lower RMSSD in women when interacting with female versus male IP (t(1515) = − 0.11, p = 0.008). There were no other significant contrasts (all ps’ ≥ 0.220).
Discussion
Overcoming limitations of previous social buffering studies in laboratory settings, this EMA study investigated how important characteristics of an interaction partner such as their familiarity and gender affect social buffering of state anxiety and related cardiovascular responses during real-life social interactions in women and men. Our results showed a decrease in state anxiety with increasing familiarity of the interaction partner (Fig. 2) which was independent of the gender of the participant and their interaction partner(s). In parallel, we assessed HR and HRV, i.e., cardiovascular responses related to subjective state anxiety ratings [see also18,20]. HR and HRV were more sensitive to gender differences than the subjective anxiety ratings. Specifically, our results showed a decrease in HR and an increase in HRV with increasing familiarity of the interaction partner in women but not in men (Fig. 3) and suggested opposite-gender social buffering effects on the autonomic level (Fig. 4).
The finding of reduced state anxiety with more familiar interaction partners in both men and women replicated the previously found social buffering effect of familiarity on subjective anxiety measures32,33,34 in everyday life. This effect was gender-independent. Extending previous findings36,37, we revealed that the social buffering effect of familiarity on autonomic anxiety-related responses differed between genders. The decrease in HR and the increase in HRV when women interacted with more familiar persons are in accordance with other findings of stronger social buffering effects in women3,21 and imply that women benefit more from the presence of a familiar interaction partner than men. The tend-and-befriend theory may provide explanations for this gender-dependent familiarity effect. This theory proposes that women have evolved to respond to stress by engaging in nurturing and protective behaviours towards social connections, seeking social support, and forming strong social bonds73,74. In the context of the present study, this suggests that women may engage in interactions with more familiar interaction partners for stress reduction, given that these persons are more likely to provide social support, and thus, to lead to stress and anxiety-reducing effects5,33. Empirical evidence further indicates that women reported greater tendencies towards tend-and-befriend and flight responses during stress, while men reported more fight responses74. In line with this, higher perceived social support under conditions of higher stress was previously associated with higher HRV in women but not in men. In turn, this aligns with previous findings which imply different stress management strategies in women versus men75. In our study, gender-dependent HRV levels suggest that men might have engaged in more adaptive autonomic regulation (i.e., higher HRV) when confronted with less familiar interaction partners. Previously, men but not women have shown adaptive HRV in negative social situations (e.g., negative social evaluation)76 as well as more adaptive stress responses after receiving social support from strangers22. As social interactions with less familiar interaction partners could be perceived as (more) negative77, this could translate to more adaptive responses in men and less autonomic emotion regulation in women during such situations. Unfamiliar interaction partners could therefore have affected women more negatively than men, similar to evidence of a higher vulnerability of women to stress-induced hyperarousal18,78 as well as their higher tendency towards tend-and-befriend or flight behaviours73,74.
In the present study, women also showed higher general levels of autonomic arousal than men, represented in higher HR during social interactions. Thus, in comparison to women, men’s need for social buffering may have been smaller as their cardiac arousal was already lower, leading to the lack of autonomic social buffering effects of familiarity in men. However, the exploratory finding of HRV-reducing effects of familiarity in men at lower (i.e., less adaptive) baseline HRV levels refutes this argument. The maladaptive effect of higher familiarity particularly emerged for those men more likely to require social buffering12,13, wheras even women with higher (i.e., more adaptive) baseline HRV profited from the social buffering effect of familiarity. These findings further support the novel gender-specific effect. Overall, the observed reductions of state anxiety scores and autonomic responses with increasing familiarity are in line with previous laboratory and EMA findings34,36,37. Extending these previous results, our findings show that in everyday life, the presence of a familiar interaction partner has a differential effect on cardiovascular responses of women versus men. The finding of differences in autonomic responses but not in subjective anxiety scores is in line with previous findings showing social buffering effects on the autonomic but not the subjective level19,22,29. It is possible that anxiety-altering effects of gender only emerged on the autonomic level because they were suppressed or misconceived on the subjective level. Factors like social norms could cause participants not to admit to gender-related differences in state anxiety79,80.
Evidence regarding gender effects in social buffering have been largely conflicting, ranging from stronger social buffering effects in women3,21, vice versa22,23, to no gender differences in social buffering26,27. Most previous studies primarily focused on the participant’s gender, while the gender of the interaction partner was either kept constant3,22 or was not included in the main analyses23. The present findings of autonomic opposite-gender effects are novel, showing that social buffering effects in everyday life are shaped by the gender of both the participant and their interaction partners. In greater detail, our results showed stronger autonomic social buffering effects if participants interacted with persons from the opposite gender (Fig. 4). In women, this was reflected in decreased HR and increased HRV in the presence of male compared to female interaction partners28,29. Similarly, men showed lower HR in the presence of female interaction partners compared to mixed-gender social interactions.
Previous studies investigating opposite-gender effects often focussed on romantic partners22,28,81. Importantly, entering romantic relationship as a control variable into our models neither improved model fit nor distinguished the opposite-gender social buffering effects, which rules out the assumption that these effects were mainly driven by the romantic partner. Men’s reduced HR when interacting with women agrees with other results on social buffering effects of a female interaction partner in men only19,22,81, while the stronger social buffering effect in women in the presence of a male interaction partner is in contrast to anxiety-buffering effects of female dyads found in the laboratory3,19. This could have different causes relating to methodology. For instance, conclusions on same versus opposite-gender social buffering effects from previous laboratory studies may be limited as many of them only investigated two-person interactions and did not compare all possible gender constellations, e.g., investigating same-gender3 or opposite-gender dyads22 but not both. Factors like role expectations82 could also be more salient and influential in laboratory compared to EMA settings and bias participants’ experience and behaviour, e.g., female participants wanting to fulfil expectations of getting along with other women and thus acting accordingly83,84.
With our EMA approach, we were able to assess everyday-life social interactions with a variety of male and female interaction partners (e.g., differing in quantity, familiarity). Extending previous studies, this allowed us to investigate the effects of social interactions with multiple interaction partners and in different gender constellations outside the laboratory, thus identifying gender-dependent social buffering effects in everyday-life social interactions. In contrast to other studies, our analyses did not only include present or very recent social interactions (e.g., within the previous five minutes)12, but also interactions that had ended anytime within the 30 min prior to the EMA prompt. In addition, we considered the length of the social interactions which could be as short as 1 min. Main effects in our models revealed that longer interactions related to lower state anxiety and higher HRV. Our findings thus suggest that social buffering effects on state anxiety may endure and last over several minutes (< 30 min) and that autonomic and subjective anxiety reductions—while being stronger after longer social interactions—can evolve even from brief contact. Note that men’s lower HR with female compared to mixed interaction partners hints towards higher anxiety-related responses during mixed-gender social interactions. This aligns with previous findings on such differential effects85,86, including stronger anxiety induction by same versus mixed-gender social partners87,88. By default, mixed-gender interactions included two or more interaction partners, whereas interactions with female or male interaction partners could also include just one person. Interestingly, our models revealed that more interaction partners were associated with lower HRV levels, implying that dyads relate to more adaptive autonomic responses than group interactions. Note that exploratory analyses showed that the opposite-gender effect did not depend on interaction partner quantity. Future research should look more closely into the diverse effects of same versus mixed-gender social interactions in everyday life.
The results of the current study show that EMA combining smartphones and wearable sensors is a useful and sensitive tool to investigate the effects of complex social interactions in everyday life. In the current study, we used this set-up in healthy and young participants with relatively low anxiety, most of whom were university students. To enhance the present findings’ generalizability, future studies should validate our findings with clinical (e.g., from the anxiety-disorder spectrum) as well as more diverse samples (e.g., differing in age and/or socioeconomic and educational background). Moreover, other potential influences on cardiovascular activity such as hormonal fluctuations in relation to women’s menstrual cycle or use of oral contraceptives89,90 could be considered. Finally, our participants interacted more frequently with familiar versus unfamiliar interaction partners. A study including more social interactions with unfamiliar interaction partners could confirm the stability of the familiarity effects. Such a study should also include a baseline measurement of state anxiety to investigate whether familiar or opposite-gender interaction partners reduce anxiety levels beyond baseline.
In summary, the present EMA study provides novel insights into gender-dependent changes in anxiety-related autonomic responses during social contacts. Based on our results, social contacts with more familiar male interaction partners could be best suited to help reduce anxiety-related autonomic responses in women. At the same time, female interaction partners (or practitioners) may be best suited for anxiety reductions in men, while their familiarity might be disregarded. In conclusion, our study underlines the importance of considering gender in the context of social buffering.
Data availability
The data and analyses presented in this study can be found in the following online repository: https://osf.io/d3tg5/?view_only=0679d2a299254ac0a0d60672c8ad6975.
References
Kikusui, T., Winslow, J. T. & Mori, Y. Social buffering: Relief from stress and anxiety. Philos. Trans. R. Soci. B Biol. Sci. 361, 2215–2228 (2006).
Christenfeld, N. & Gerin, W. Social support and cardiovascular reactivity. Biomed. Pharmacother. 54, 251–257 (2000).
Qi, Y. et al. Social buffering of human fear is shaped by gender, social concern, and the presence of real versus virtual agents. Transl. Psychiatry 11, 641 (2021).
Hennessy, M. B., Kaiser, S. & Sachser, N. Social buffering of the stress response: Diversity, mechanisms, and functions. Front. Neuroendocrinol. 30, 470–482 (2009).
Taylor, S. E. Social support: A review. In The Oxford Handbook of Health Psychology (ed. Friedman, S.) 189–214 (Oxford University Press, New York, NY, USA, 2011).
Ditzen, B. et al. Adult attachment and social support interact to reduce psychological but not cortisol responses to stress. J. Psychosom. Res. 64, 479–486 (2008).
Ryska, T. A. & Yin, Z. Testing the buffering hypothesis: Perceptions of coach support and pre-competitive anxiety among male and female high school athletes. Curr. Psychol. 18, 381–393 (1999).
Thorsteinsson, E. B. & James, J. E. A meta-analysis of the effects of experimental manipulations of social support during laboratory stress. Psychol. Health 14, 869–886 (1999).
Schiweck, C., Piette, D., Berckmans, D., Claes, S. & Vrieze, E. Heart rate and high frequency heart rate variability during stress as biomarker for clinical depression. A systematic review. Psychol. Med. 49, 200–211 (2019).
Grillon, C., Duncko, R., Covington, M. F., Kopperman, L. & Kling, M. A. Acute stress potentiates anxiety in humans. Biol. Psychiatry 62, 1183–1186 (2007).
Horsten, M. et al. Psychosocial factors and heart rate variability in healthy women. Psychosom. Med. 61, 49–57 (1999).
Schwerdtfeger, A. R. & Friedrich-Mai, P. Social interaction moderates the relationship between depressive mood and heart rate variability: Evidence from an ambulatory monitoring study. Health Psychol. 28, 501–509 (2009).
Appelhans, B. M. & Luecken, L. J. Heart rate variability as an index of regulated emotional responding. Rev. Gen. Psychol. 10, 229–240 (2006).
Krahé, C., Springer, A., Weinman, J. A. & Fotopoulou, A. The social modulation of pain: Others as predictive signals of salience–a systematic review. Front. Hum. Neurosci. 7, 386 (2013).
Eisenberger, N. I. An empirical review of the neural underpinnings of receiving and giving social support: Implications for health. Psychosom. Med. 75, 545–556 (2013).
McLean, C. P. & Anderson, E. R. Brave men and timid women? A review of the gender differences in fear and anxiety. Clin. Psychol. Rev. 29, 496–505 (2009).
Villada, C., Hidalgo, V., Almela, M. & Salvador, A. Individual differences in the psychobiological response to psychosocial stress (Trier Social Stress Test): The relevance of trait anxiety and coping styles. Stress Health 32, 90–99 (2016).
Kudielka, B. M., Buske-Kirschbaum, A., Hellhammer, D. H. & Kirschbaum, C. Differential heart rate reactivity and recovery after psychosocial stress (TSST) in healthy children, younger adults, and elderly adults: The impact of age and gender. Int. J. Behav. Med. 11, 116–121 (2004).
Glynn, L. M., Christenfeld, N. & Gerin, W. Gender, social support, and cardiovascular responses to stress. Psychosom. Med. 61, 234–242 (1999).
Hamidovic, A. et al. Quantitative meta-analysis of heart rate variability finds reduced parasympathetic cardiac tone in women compared to men during laboratory-based social stress. Neurosci. Biobehav. Rev. 114, 194–200 (2020).
Reddan, M. C., Young, H., Falkner, J., López-Solà, M. & Wager, T. D. Touch and social support influence interpersonal synchrony and pain. Soc. Cogn. Affect. Neurosci. 15, 1064–1075 (2020).
Kirschbaum, C., Klauer, T., Filipp, S.-H. & Hellhammer, D. H. Sex-specific effects of social support on cortisol and subjective responses to acute psychological stress. Psychosom. Med. 57, 23–31 (1995).
Well, S. V. & Kolk, A. M. Social support and cardiovascular responding to laboratory stress: Moderating effects of gender role identification, sex, and type of support. Psychol. Health 23, 887–907 (2008).
Kelly, M. M., Tyrka, A. R., Anderson, G. M., Price, L. H. & Carpenter, L. L. Sex differences in emotional and physiological responses to the trier social stress test. J. Behav. Ther. Exp. Psychiatry 39, 87–98 (2008).
Trotman, G. P. et al. Associations between heart rate, perceived heart rate, and anxiety during acute psychological stress. Anxiety Stress Coping 32, 711–727 (2019).
Shahrestani, S., Stewart, E. M., Quintana, D. S., Hickie, I. B. & Guastella, A. J. Heart rate variability during adolescent and adult social interactions: A meta-analysis. Biol. Psychol. 105, 43–50 (2015).
Lepore, S. J. Social conflict, social support, and psychological distress: Evidence of cross-domain buffering effects. J. Pers. Soc. Psychol. 63, 857–867 (1992).
Phillips, A. C., Carroll, D., Hunt, K. & Der, G. The effects of the spontaneous presence of a spouse/partner and others on cardiovascular reactions to an acute psychological challenge. Psychophysiology 43, 633–640 (2006).
Phillips, A. C., Gallagher, S. & Carroll, D. Social support, social intimacy, and cardiovascular reactions to acute psychological stress. Ann. Behav. Med. 37, 38–45 (2009).
Conner, T. S. & Mehl, M. R. Ambulatory assessment: Methods for studying everyday life. In Emerging Trends in the Social and Behavioral Sciences: An Interdisciplinary, Searchable, and Linkable Resource (ed. R. Scott, S.K., N. Pinkerton) 1–15 (John Wiley & Sons, Hoboken, NJ, 2015).
Shiffman, S., Stone, A. A. & Hufford, M. R. Ecological momentary assessment. Annu. Rev. Clin. Psychol. 4, 1–32 (2008).
Lee, H. J. Perceptions towards an interaction partner predict social anxiety: An ecological momentary assessment study. Cogn. Emot. 35, 1479–1498 (2021).
Mascret, N., Vors, O., Marqueste, T., Casanova, R. & Cury, F. Social support from evaluative familiar persons–a buffer against stress? Preliminary evidence of neuroendocrine and psychological responses. Anxiety Stress Coping 32, 534–544 (2019).
Hur, J. et al. Social context and the real-world consequences of social anxiety. Psychol. Med. 50, 1989–2000 (2019).
Heimberg, R.G., Brozovich, F.A. & Rapee, R.M. A cognitive behavioral model of social anxiety disorder: Update and extension. In Social Anxiety (eds. Hofmann, S.G. & DiBartolo, P.M.) 395–422 (Elsevier, 2010).
Holt-Lunstad, J., Uchino, B. N., Smith, T. W., Olson-Cerny, C. & Nealey-Moore, J. B. Social relationships and ambulatory blood pressure: Structural and qualitative predictors of cardiovascular function during everyday social interactions. Health Psychol 22, 388–397 (2003).
Schwerdtfeger, A. R., Rominger, C. & Obser, P. D. A shy heart may benefit from everyday life social interactions with close others: An ecological momentary assessment trial using Bayesian multilevel modeling. Biol. Psychol. 152, 107864 (2020).
Faul, F., Erdfelder, E., Buchner, A. & Lang, A. G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 41, 1149–1160 (2009).
Hautzinger, M. & Bailer, M. in Allgemeine Depressionsskala (Kurzform). (Beltz Test Gesellschaft, Göttingen, 1993).
Laux, L., Glanzmann, P., Schaffner, P. & Spielberger, C. D. Das State-Trait-Angstinventar (STAI) (Beltz, 1981).
Heimberg, R. G., Mueller, G. P., Holt, C. S., Hope, D. A. & Liebowitz, M. R. Assessment of anxiety in social interaction and being observed by others: The social interaction anxiety scale and the social phobia scale. Behav. Ther. 23, 53–73 (1992).
Grimm, J. State-Trait-Anxiety Inventory nach Spielberger. Deutsche Lang-und Kurzversion. Methodenforum der Universität Wien: MF-Working Paper (2009).
Venaglia, R. B. & Lemay, E. P. Jr. Hedonic benefits of close and distant interaction partners: The mediating roles of social approval and authenticity. Pers. Soc. Psychol. Bull. 43, 1255–1267 (2017).
Vogel, N., Ram, N., Conroy, D. E., Pincus, A. L. & Gerstorf, D. How the social ecology and social situation shape individuals’ affect valence and arousal. Emotion 17, 509–527 (2017).
Goodman, F. R., Stiksma, M. C. & Kashdan, T. B. Social anxiety and the quality of everyday social interactions: The moderating influence of alcohol consumption. Behav. Ther. 49, 373–387 (2018).
Kashdan, T. B. et al. A contextual approach to experiential avoidance and social anxiety: Evidence from an experimental interaction and daily interactions of people with social anxiety disorder. Emotion 14, 769–781 (2014).
Cornelius, T., Birk, J. L., Edmondson, D. & Schwartz, J. E. The joint influence of emotional reactivity and social interaction quality on cardiovascular responses to daily social interactions in working adults. J. Psychosom. Res. 108, 70–77 (2018).
Quintana, D. S. & Heathers, J. A. Considerations in the assessment of heart rate variability in biobehavioral research. Front. Psychol. 5, 805 (2014).
Valentini, M. & Parati, G. Variables influencing heart rate. Prog. Cardiovasc. Dis. 52, 11–19 (2009).
Camm, A. J. et al. Heart rate variability: Standards of measurement, physiological interpretation and clinical use. Task force of the european society of cardiology and the north american society of pacing and electrophysiology. Circulation 93, 1043–11065 (1996).
Thayer, J. F., Ahs, F., Fredrikson, M., Sollers, J. J. & Wager, T. D. A meta-analysis of heart rate variability and neuroimaging studies: Implications for heart rate variability as a marker of stress and health. Neurosci. Biobehav. Rev. 36, 747–756 (2012).
McCraty, R. & Shaffer, F. Heart rate variability: New perspectives on physiological mechanisms, assessment of self-regulatory capacity, and health risk. Glob. Adv. Health Med. 4, 46–61 (2015).
Shaffer, F. & Ginsberg, J. P. An overview of heart rate variability metrics and norms. Front. Public Health 5, 258 (2017).
Kemp, A. H. & Quintana, D. S. The relationship between mental and physical health: Insights from the study of heart rate variability. Int. J. Psychophysiol. 89, 288–296 (2013).
Kok, B. E. & Fredrickson, B. L. Upward spirals of the heart: Autonomic flexibility, as indexed by vagal tone, reciprocally and prospectively predicts positive emotions and social connectedness. Biol. Psychol. 85, 432–436 (2010).
Sheridan, D. C., Dehart, R., Lin, A., Sabbaj, M. & Baker, S. D. Heart rate variability analysis: How much artifact can we remove?. Psychiatry Investig. 17, 960–965 (2020).
Pham, T., Lau, Z. J., Chen, S. & Makowski, D. Heart rate variability in psychology: A review of HRV indices and an analysis tutorial. Sensors 21, 3998 (2021).
Liu, H., Chen, B., Wang, Y., Zhao, X. & Hu, J. Social affiliation moderates the link between depressive symptoms and heart rate variability in healthy middle-aged and older individuals: An intensive ecologic momentary assessment study. Psychophysiology 59, e13958 (2021).
Wrzus, C., Müller, V., Wagner, G. G., Lindenberger, U. & Riediger, M. Affective and cardiovascular responding to unpleasant events from adolescence to old age: Complexity of events matters. Dev. Psychol. 49, 384–397 (2013).
Bolger, N. & Laurenceau, J.-P. Intensive Longitudinal Methods: An Introduction to Diary and Experience Sampling Research (Guilford press, 2013).
Hamilton, P. Open source ECG analysis. in Computers in Cardiology 101–104 (IEEE, Memphis, TN, USA, 2002).
Clifford, G., McSharry, P. & Tarassenko, L. Characterizing artefact in the normal human 24-hour RR time series to aid identification and artificial replication of circadian variations in human beat to beat heart rate using a simple threshold. In Computers in Cardiology (Memphis, TN, USA, pp. 129–132, 2002).
Tukey, J. W. Exploratory Data Analysis (Pearson, London, 1977).
Bates, D., Mächler, M., Bolker, B. & Walker, S. Fitting linear mixed-effects models using lme4. J. Stat. Softw. 67, 1–48 (2015).
Kuznetsova, A., Brockhoff, P. B. & Christensen, R. H. lmerTest package: Tests in linear mixed effects models. J. Stat. Softw. 82, 1–26 (2017).
Lüdecke, D., Ben-Shachar, M. S., Patil, I., Waggoner, P. & Makowski, D. performance: An R package for assessment, comparison and testing of statistical models. J. Open Source Softw. 6, 3139 (2021).
Lüdecke, D. sjPlot: Data visualization for statistics in social science. R package version 2.8.11. (2015).
Long, J.A. Interactions: Comprehensive, user-friendly toolkit for probing interactions. R package version 1.1.5. (2019).
Laborde, S., Mosley, E. & Thayer, J. F. Heart rate variability and cardiac vagal tone in psychophysiological research—Recommendations for experiment planning, data analysis, and data reporting. Front. Psychol. 8, 213 (2017).
Bernstein, M. J., Zawadzki, M. J., Juth, V., Benfield, J. A. & Smyth, J. M. Social interactions in daily life: Within-person associations between momentary social experiences and psychological and physical health indicators. J. Soc. Pers. Relat. 35, 372–394 (2018).
O’Day, E. B. & Heimberg, R. G. Social media use, social anxiety, and loneliness: A systematic review. Comput. Hum. Behav. Rep. 3, 100070 (2021).
Kutner, M. H., Nachtsheim, C. J. & Neter, J. Applied Linear Regression Models (McGraw-Hill/Irwin, New York, 2004).
Taylor, S. E. et al. Biobehavioral responses to stress in females: Tend-and-befriend, not fight-or-flight. Psychol. Rev. 107, 411 (2000).
Levy, K. N., Hlay, J. K., Johnson, B. N. & Witmer, C. P. An attachment theoretical perspective on tend-and-befriend stress reactions. Evol. Psychol. Sci. 5, 426–439 (2019).
Kvadsheim, E. et al. Vagally mediated heart rate variability, stress, and perceived social support: A focus on sex differences. Stress 25, 113–121 (2022).
Vanderhasselt, M.-A., De Raedt, R., Nasso, S., Puttevils, L. & Mueller, S. C. Don’t judge me: Psychophysiological evidence of gender differences to social evaluative feedback. Biol. Psychol. 135, 29–35 (2018).
Reis, H. T., Maniaci, M. R., Caprariello, P. A., Eastwick, P. W. & Finkel, E. J. Familiarity does indeed promote attraction in live interaction. J. Pers. Soc. Psychol. 101, 557–570 (2011).
Bangasser, D. A., Eck, S. R., Telenson, A. M. & Salvatore, M. Sex differences in stress regulation of arousal and cognition. Physiol. Behav. 187, 42–50 (2018).
Biel, A. & Thøgersen, J. Activation of social norms in social dilemmas: A review of the evidence and reflections on the implications for environmental behaviour. J. Econ. Psychol. 28, 93–112 (2007).
Cislaghi, B. & Heise, L. Gender norms and social norms: Differences, similarities and why they matter in prevention science. Sociol. Health Illn. 42, 407–422 (2020).
Monin, J. K. et al. Gender differences in short-term cardiovascular effects of giving and receiving support for health concerns in marriage. Health Psychol. 38, 936–947 (2019).
Robinson, M. E. & Wise, E. A. Gender bias in the observation of experimental pain. Pain 104, 259–264 (2003).
Eagly, A.H. & Wood, W. Social role theory. In Handbook of theories of social psychology, Vol. 2 (eds. Lange, P.A.M.V., Kruglanski, A.W. & Higgins, E.T.) 458–476 (Sage publications, Thousand Oaks, CA, 2012).
Eagly, A. H. & Wood, W. Explaining sex differences in social behavior: A meta-analytic perspective. Pers. Soc. Psychol. Bull. 17, 306–315 (1991).
Greenfield, S. F., Cummings, A. M., Kuper, L. E., Wigderson, S. B. & Koro-Ljungberg, M. A qualitative analysis of women’s experiences in single-gender versus mixed-gender substance abuse group therapy. Subst. Use Misuse 48, 750–760 (2013).
Leaper, C. Young adults’ conversational strategies during negotiation and self-disclosure in same-gender and mixed-gender friendships. Sex Roles 81, 561–575 (2019).
Allen, A. P., Kennedy, P. J., Cryan, J. F., Dinan, T. G. & Clarke, G. Biological and psychological markers of stress in humans: Focus on the trier social stress test. Neurosci. Biobehav. Rev. 38, 94–124 (2014).
Duchesne, A., Tessera, E., Dedovic, K., Engert, V. & Pruessner, J. C. Effects of panel sex composition on the physiological stress responses to psychosocial stress in healthy young men and women. Biol. Psychol. 89, 99–106 (2012).
Schmalenberger, K. M. et al. A systematic review and meta-analysis of within-person changes in cardiac vagal activity across the menstrual cycle: Implications for female health and future studies. J. Clin. Med. 8, 1946 (2019).
Kirschbaum, C., Kudielka, B. M., Gaab, J., Schommer, N. C. & Hellhammer, D. H. Impact of gender, menstrual cycle phase, and oral contraceptives on the activity of the hypothalamus-pituitary-adrenal axis. Psychosom. Med. 61, 154–162 (1999).
Acknowledgements
We thank Julia Weschenfelder for her support during data collection and Shawn Hiew Siu Ping for valuable input on a previous version of the manuscript. This work was supported by the German Research Foundation (GH, grant number HE 4566/5-1).
Funding
This publication was supported by the Open Access Publication Fund of the University of Wuerzburg. Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Contributions
Conceptualization: M.G. and G.H.; Data curation: M.G. and M.W.; Formal analysis: M.G. and M.W.; Funding acquisition: J.D. and G.H.; Investigation: M.G. and K.S.; Methodology: M.G., M.W. and G.H.; Project administration: M.G.; Resources: J.D. and G.H.; Supervision: M.W. and G.H.; Validation: M.G., M.W. and G.H.; Visualization: M.G. and M.W.; Writing – original draft: M.G., M.W., K.S. and G.H.; Writing - review & editing: M.G., M.W., K.S., J.D. and G.H.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Gründahl, M., Weiß, M., Stenzel, K. et al. The effects of everyday-life social interactions on anxiety-related autonomic responses differ between men and women. Sci Rep 13, 9498 (2023). https://doi.org/10.1038/s41598-023-36118-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-36118-z
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
