
Abstract
During the past 30 years, a mortality gap developed between Lolland-Falster (the rural-provincial southeastern part) and the rest of Denmark. A main driver was selective in-migration of Danes with a high risk of death, especially of working-ages. In the present study, we determined the role of economic status in this selective in-migration. We used individual-level data from the Central Population Register and data on income source; self- or publicly supported. The study population included people aged 30–64 and living in Denmark at any time between 1992 and 2018. Mortality rate ratios (MRR) were calculated using Poisson regression for three time-periods: 1992–1999, 2000–2009 and 2010–2018. Two in five in-migrants to Lolland-Falster were people on public support. In 2010–2018, they had an MRR of 8.71 (95% confidence interval (CI): 8.05–9.42) compared with self-supported people, and an MRR of 1.49 (95% CI: 1.38–1.61) compared with publicly supported people elsewhere in Denmark. In-migration of working-aged people on public support was a main contributor to the excess mortality in Lolland-Falster as compared with the rest of Denmark. To understand urban–rural differences in health, population movements and national income patterns are important to take into account.
Similar content being viewed by others

Introduction
Trends of healthy people leaving rural areas in favour of urban areas have been found to increase geographical inequalities in health, as the vulnerable and elderly people are left behind1,2,3,4. In Europe, certain rural areas suffering from depopulation may enter a ‘vicius circle of decline’ where people migrate in search of better jobs, public health services decline, and private health service practioners move to more profitable areas5.
In Denmark, Lolland-Falster is a rural-provincial area in the south eastern part of the country characterised by depopulation6, low life expectancy7, a high proportion of elderly people6, several negative health indicators such as high prevalence of smoking and obesity, and low prevalence of physical activity, and a high prevalence of chronic diseases e.g. diabetes, hypertension and cancer8.
However, in contrast to the observations from other countries, the currently high mortality in Lolland-Falster has been driven mainly by vulnerable people of working-age moving into Lolland-Falster from other parts of Denmark9,10. In-migrants to Lolland-Falster of working-ages have a mortality rate ratio (MRR) of 2.35 (95% confidence interval (CI): 2.19–2.52) compared with the mortality in the rest of Denmark10.
On this basis, we determined the role of economic status behind this selective migration pattern from the urban parts of Denmark to the rural-provincial area of Lolland-Falster.
Methods
The study population included all people aged 30–64 years and living in Denmark at any time between 1992 and 2018. Data for the study population were extracted from the Central Population Register (CPR), with individual-level data on all persons ever living in Denmark in the study period including data on sex, date of birth, death, address history, emigration, and immigration11. A given person contributed person-years at risk during the time-period he/she had been present in Denmark in the relevant age-group 30–64 years. We studied three time-periods: 1992–1999, 2000–2009; and 2010–2018.
CPR data were merged with data from Statistics Denmark´s socioeconomic classification (SOCIO13) including data on annual main income source for 1991–201712. Data was accessed through Statistics Denmark’s research server. Data are available from Statistics Denmark upon reasonable request.
Residency group
Lolland-Falster includes Lolland and Guldborgsund municipalities. We divided the Danish population into three residency groups: long-term residents of Lolland-Falster, the in-migrants to Lolland-Falster, and the rest of the Danish population for the three time-periods (1992–1999, 2000–2009, and 2010–2018). Construction of the residency groups has been reported in details previously10. In short, a person’s residency group was based on his/her address history during the previous 10 years. Thus, to be a long-term resident in a given time-period, a person had to have lived continuously in Lolland-Falster 10 years prior to the time-period and he/she remained in the long-term residency group up until death, emigration, or end of follow-up. In-migrants had moved to Lolland-Falster during the 10 years preceding the time-period or during the time-period. A person could contribute person-years to different residency groups during different time-periods, and a long-term resident would become an in-migrant if he/she moved outside Lolland-Falster and back again during a time-period. The long-term residents and the in-migrants together constituted the total Lolland-Falster population.
Economic status
In a previous study on economic status in Danish municipalities by the Danish Center for Social Science Research, unemployed persons and other people on public support were merged into one group13. Likewise, in the present study we used the annual SOCIO13-groups with 20 mutually exclusive categories to create a dichotomous variable indicating whether a person during the majority of the previous year was economically self-supported or publicly supported. The self-supported group included employees, self-employed persons and their assisting spouses. The publicly supported group included people on public transfer payment; non-old age pensioners, old age pensioners, and people on unemployment benefit, early retirement scheme, sickness benefits, cash benefits or adult education support (see Appendix Table 1)12. Non-old age pensioners included persons receiving pension due to disability or chronic disease. Cash benefit is the residual group of the unemployed people not qualified to be in the other groups, including individuals waiting to be accepted into one of the other groups. If a person had missing data for SOCIO13 one year; they would not contribute to the analysis with person-years or deaths in the following year.
Analysis
The study used Danish administrative register-data. All registers include date of birth, all changes of addresses with dates, and data on socioeconomic status are registered once a year. The study population was dynamic in the sense that a given person contributed person-years to a given group from the point in time where he/she fulfilled the criteria for belonging to the group until he/she did not any longer fulfill these criteria. First, a given person contributed person-years as long as he/she was 30–64 years old. Second, a given person belonged to the population in the rest of Denmark as long as he/she was registered with an address in Denmark outside Lolland-Falster. Lolland-Falster residents were divided into long-term residents and in-migrants based on their address history. Third, a given person belonged to the last socioeconomic group in which he/she appeared in the register.
The number of persons belonging to a given group can be calculated for a given date, e.g. 1 January 1992. However, over time a given person could contribute to more than one group. The sum of numbers of persons aged 30–64 years over time, e.g. 1992 to 1999, contributing to the different groups was therefore larger than the counts of persons on a given date. The population flow by address-group during each time-period is illustrated in Appendix Fig. 1. Due to movements between groups over time, the study population is reflected better in person-years than in the number of persons.
For analysis of mortality by residency and economic status, we used Poisson regression to calculate mortality rate ratio (MRR) with 95% CI. We used the method described by Rostgaard to transform the longitudinal dataset into event-time tables and conduct the Poisson regression14. The analysis was conducted separately for men and women and for the total population. The model was adjusted for 5-year age-group and for sex for the total population. For each time-period, self-supported people in the rest of Denmark were used as the reference group; or publicly supported people in Lolland-Falster were compared with that of publicly supported people in the rest of Denmark.
Two sensitivity analyses were made. First, residency was categorised by residency 20 years instead of 10 years before each time-period. Second, as a self-supported person who becomes sick and dies may receive public support shortly before death, the death rate for publicly supported persons may be inflated. Thus, an additional analysis was made categorising economic status by the annual status three years before. This analysis could not be made for 1992–1999, as SOCIO13 data were available only from 1991 onwards.
All analysis were made in SAS 9.4 and graphics were made in R 4.0.3 at a research server in Statistics Denmark.
Ethics
The present study was a register-based study using anonymised individual level data. According to Danish legislations, register-based studies not including genetic data and with no contact to patients, relatives, and/or treating physician, registration by the responsible institution serves at ethical clearance (Databeskyttelsesforordningen and Databeskyttelsesloven)15,16. The study registration number in Region Zealand is REG-108-2018.
Results
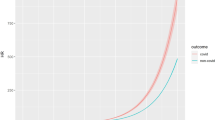
In the rest of Denmark, the population aged 30–64 increased between 1992 and 2008 from 2,090,000 to 2,380,000; decreased to 2,300,000 in 2013, and was relatively stable until 2018 (Fig. 1). In Lolland-Falster, the population aged 30–64 increased slightly from 48,400 in 1992 to 49,800 in 1998, whereafter it decreased by 20% to 39,800 in 2018.

Mid-year population number for people aged 30–64 years living in Lolland-Falster and in the rest of Denmark by year, 1992–2018.
The study population included 66,226,171 person-years and 270,466 deaths (Table 1). In the rest of Denmark, the self-supported group constituted 74% of the person-years in 1992–1999, and 78% in 2000–2009 as well as 2010–2018. In Lolland-Falster, the self-supported group constituted 67% of the person-years in 1992–1999, 70% in 2000–2009, and 68% in 2010–2018. In Lolland-Falster in 2010–2018, 72% of long-term residents and 58% of in-migrants in Lolland-Falster were self-supported.
Over time, self-supported, long-term residents constituted 52–54% of the person-years in the total Lolland-Falster population, while self-supported in-migrants constituted 13–17%. The publicly supported, long-term residents constituted 19–22% of the total Lolland-Falster population, while the publicly supported in-migrants constituted the remaining 11–12%. The publicly supported group consisted mainly of persons on non-old age pension or cash benefit. In 2010–2018, 47% of people on public support in Lolland-Falster received non-old age pension; 51% among long-term residents and 39% among in-migrants; compared with 37% in the rest of Denmark (Appendix Table 1). The percentages for cash benefit were 21% for Lolland-Falster; 15% for long-term residents; 31% for in-migrants; and 20% for the rest of Denmark.
Mortality rate ratio for residency groups by economic status
Compared with self-supported people in the rest of Denmark, self-supported people in Lolland-Falster had an elevated MRR increasing by time from 1.12 (95% CI: 1.04–1.21) in 1992–1999 to 1.42 (95% CI: 1.31–1.53) in 2010–2018 (Table 2 and Fig. 2). Compared with publicly supported people in the rest of Denmark, publicly supported people in Lolland-Falster had an elevated MRR increasing from 1.02 (95% CI: 0.98–1.07) in 1992–1999 to 1.28 (95% CI: 1.22–1.34) in 2010–2018 (Appendix Table 2).

Mortality rate ratio and percentage of person-years for the rest of Denmark and the total population aged 30–64 years in Lolland-Falster by residency group, economic status, and time-period. Adjusted for 5-year age-groups and sex. Reference population = Self-supported in rest of Denmark.
For the self-supported group in Lolland-Falster, the excess mortality as compared with that of self-supported people in the rest of Denmark emerged over time for long-term residents and was present for in-migrants in all time-periods (Table 2 and Fig. 2). The MRRs for self-supported, long-term residents increased from 1.08 (95% CI: 0.99–1.17) in 1992–1999 to 1.39 (95% CI: 1.28–1.51) in 2010–2018. For self-supported in-migrants, the MRR increased from 1.33 (95% CI: 1.12–1.59) in 1992–1999 to 1.55 (95% CI: 1.30–1.85) in 2010–2018.
For the publicly supported group in Lolland-Falster, the excess mortality as compared with self-supported people in the rest of Denmark increased with every time-period for the long-term residents as well as for the in-migrants. The MRR for the publicly supported long-term residents reached 6.63 (95% CI: 6.26–7.03) in 2010–2018, and the MRR for publicly supported in-migrants reached 8.71 (95% CI: 8.05–9.42) in 2010–2018. However, compared with self-supported people, the excess mortality for the publicly supported group increased also over time in the rest of Denmark from 3.91 (95% CI: 3.84–3.97) in 1992–1999 to 5.65 (95% CI: 5.56–5.74) in 2010–2018.
The MRR trends were similar for men and women. It should be noted though that in 2010–2018 the MRR for male in-migrants on public support reached 9.76 (95% CI: 8.88–10.74).
Sensitivity analysis
Sensitivity analysis using 20 years of address history prior to the time-period to categorise the residency groups, showed similar results as the main analysis using 10 years of address history (Appendix Table 3).
When categorising annual economic group three years back in time instead of one year, the excess mortality for publicly supported people compared with self-supported people decreased slightly (Appendix Table 4). Compared with self-supported people in the rest of Denmark, the MRR for publicly supported people in the rest of Denmark 2010-2018 was 5.65 (95% CI: 5.56–5.74) when categorising one year back in time and 4.60 (95% CI: 4.53–4.67) when categorised three years back. For the total of Lolland-Falster, the change was from an MRR of 7.24 (95% CI: 6.90–7.59) to 6.08 (95% CI: 5.78–6.40).
Discussion
Main results
Mortality in the rural-provincial area of Lolland-Falster is high compared with the level in the rest of Denmark. This is a relatively new phenomenon where a gap in mortality between Lolland-Falster and the rest of Denmark emerged gradually from around 19909. We have shown previously that this excess mortality derived mainly from in-migrants from other parts of Denmark, and especially from in-migrants of working-age10. In the present analysis, we demonstrated that this mortality gap was attributable mainly to in-migration to Lolland-Falster of persons economically on public support. In the Danish welfare system, poor health is in some instances a precondition for eligibility for public support in working-age17. In 2010–2018, two out of five in-migrants of working-age to Lolland-Falster were on public support, and these in-migrants had a ninefold mortality compared with that of self-supported persons in the rest of Denmark. Selective migration of publicly supported people of working-age was thus the most important factor behind the presently high mortality at Lolland-Falster.
Previous studies
The impact of selective migration on area-based differences in mortality has been investigated in a number of studies from the UK. Most of these studies have taken advantage of the Office for National Statistics Longitudinal Study (ONS LS)18. In these studies, areas have been classified in two ways; by an area-based deprivation index and by a rural–urban gradient. When comparing studies from the UK with those from other countries, it is important to note that there is a positive correlation between severity of deprivation and urbanity in the UK, while in many other countries, the rural areas are the most deprived. In the following we therefore focus on the UK studies on rural–urban differences in mortality.
It was a consistent pattern across the UK studies that rural areas had lower mortality than urban areas, and this mortality gap increased over time19. Over the 20-year period from 1981 to 2001, selective migration of better off people from urban to rural areas contributed to this increasing gap in England and Wales19, but in studies covering shorter periods; 1991–2001 in Scotland20 and 2006–2011 in Wales21, selective migration had no impact on the regional mortality differences. As noted by Brimblecombe et al.22, the measured impact of migration on geographical differences in mortality depends also on the composition of the areas; the measured impact will be greater when migration is studied between small homogeneous districts than between larger heterogenous regions.
In Sweden, the mortality of people moving from Northern to Southern Sweden resembled that of people staying in other parts of Sweden23. However, the movers had higher education, thus, when adjusting for education, the movers had an excess mortality. Men returning to Northern Sweden after having lived in Southern Sweden had higher mortality than men staying in other parts of Sweden. Adjustment for education enhanced the difference. The pattern illustrated the salmon effect where migrants move home in anticipation of death; here the pattern indicated to be most common among migrants with higher education.
Another Swedish study investigated the potential impact of selective migration on the low mortality in Halland, Sweden for the period 1980–199024. Within Halland, men born there had lower mortality than men born elsewhere despite indication of a higher socioeconomic background of these in-migrants25. Outside Halland, men born in Halland still had lower mortality than other men. These differences were statistically non-significant for women24. Thus, selective migration did not explain the low mortality in Halland.
Mortality in 1971–2004 for 40–59 old persons in Finland was analysed by birthplace26. Among men living in Southern Finland, those born in Northern and Eastern Finland had an excess mortality. When adjusted for education the excess risk prevailed for men born in Northern Finland but not for men born in Eastern Finland. Men who migrated from Northern Finland also had higher mortality than men who stayed in the North. Differences for women were not statistically significant. The study indicated that men who migrated out of Northern Finland constituted a high-risk group unrelated to their level of education.
The difference between the UK and Denmark was noteworthy. In the UK, the rural areas have lower mortality than urban areas, and selective migration of better off people from urban to rural areas contributed to a widening of this gap over time. In Denmark, the rural area of Lolland-Falster has higher mortality than the rest of Denmark, and selective in-migration of people on public support has contributed to a widening of this gap. The Swedish and Finnish studies focused on people moving from the rural North to the urban South of the respective countries. In Finland, people in the North had higher mortality than people in the South and Northern migrants to the South constituted a high-risk group both compared with those who stayed in the North and those who lived in the South. In Sweden, migrants from the North had a mortality similar to people staying in the South, while movers from the North returning to the North had a higher risk of death. In Denmark, the mortality gap between Lolland-Falster and the rest of Denmark started around 19909. The mortality gap developed alongside with a population decrease. The decrease has mainly been attributed to young people moving away10, but these generations are still too young to have affected regional differences in mortality.
Strengths and limitations
A strength in the present study was the use of nationwide, high-quality, Danish register data. As these register-data are used for official statsistics, they are already validated by Statistics Denmark, before released for research purpose. On a subject level we divided the follow-up time into groups given by age, calendar period, sex, residency group, and economic status and counted the number of deaths for each combination of these variables. The natural model for analysing count data is Poisson regression. Differences in follow-up time were accounted for by including an offset in the model27.
Mortality was higher among people on public support than among self-supported people, but the mortality rates of people on public support may be inflated by deaths in previously self-supported people being on e.g. sickness benefit towards the end of life. We therefore added an analysis based on economic status three years back (see Appendix Table 4). This decreased the excess mortality of publicly supported people, though the relative difference between Lolland-Falster and the rest of Denmark, between in-migrants and long-term residents, and across time-periods persisted.
Interpretation
The above comparison with UK and Nordic studies illustrated that local circumstances have to be taken into account in the interpretation of regional differences in mortality. In the rural area of Lolland-Falster, the mortality is higher than in the rest of Denmark, and the present study showed that a major part of this excess mortality is attributable to in-migrants on public support.
The increased mortality among people on public support may be due to selection with illness causing inability to work and/or a negative impact on health of a life outside the labour market28. In our study population, the most common type of public support was non-old age pension for which permanently impaired health is the main eligibility criteria17. Among publicly supported people, those on unemployment benefit constituted a smaller group, but unemployment in itself may impair health29. The excess mortality of the publicly supported group in our study increased over time. This trend may have been enhanced by political initiatives to keep people in the workforce and affecting selection as more stringent criteria were used for granting of non-old age pension. It may also explain the increasing proportion of people on cash benefit, which is granted to people in principle considered suitable for work. Cash benefit is the economically lowest type of public support. Thus, the publicly supported people in Denmark may have become relatively poorer over time compared with the self-supported people.
Economic Council of the Labour Movement has previously reported that Lolland-Falster was among the areas in Denmark with the highest net growth in in-migration of people on public support30, and in 2020, in-migrants to Lolland-Falster had a lower disposable income than in-migrants to other municipalities31. A reason for people with a relatively low disposable income moving to Lolland-Falster was primarily an increasing gap in housing prices between rural areas like Lolland-Falster and urban/suburban areas close to the capital of Copenhagen32,33. In Denmark, people on public support can move freely between areas of the country. Thus, it was possible for publicly supported people to move to an area with lower expenses. Other changes in living circumstances like break-up with partners, conflicts with neighbors or other difficulties in life that we could not include in the present study, may also have played a role. The in-migrant population was not stable but relatively dynamic with persons moving in, followed by moving out, and then in again and out again, as illustrated in Appendix Fig. 1. The disposable income decreased from 2002 to 2011 for the poorest decile of the Danish population, despite an increase in the average income34, and using the Gini coefficient the OECD concluded that Denmark among other countries experienced increasing income inequality between 1980 and 201335. Low socioeconomic status is in itself a risk factor for premature death36, and social inequality in mortality in Denmark has increased37,38.
We observed previously a selective in-migration to Lolland-Falster of people with a high risk of death10. The present study was the first to investigate the role of economic status in selective migration and regional mortality differences in Denmark. Given the high inflow of people at a high risk of death, our study illustrates the role of circulation of biological capital39 in the generation of regional differences in mortality in a Nordic welfare state. However, the excess mortality on Lolland-Falster could not be explained entirely by the large share of people on public support. Compared with the rest of Denmark, we found an excess mortality in Lolland-Falster within each of the economic status and residency groups, though stronger for in-migrants than for long-term residents. An explanation could be that in-migrants generally have a weaker social support system than long-term residents, placing them at increased risk of death when health fails them. Another explanation could be a generally negative health selection of people moving to Lolland-Falster independently of economic status. It should be noted though that we used a crude categorisation of economic status; within the group of self-supported people there is inequalities in mortality across occupations40,41; and within the group of publicly supported people, mortality is expected to differ between those on temporary unemployment benefit and those on permanent non-old age pension.
Lolland-Falster had a relatively high annual population turn-over of 7%42. The number of people moving in and out of Lolland-Falster was almost similar over the years, though, a higher number of people moving in were between ages 30 and 64 years42. We found previously that long-term residents moving away from Lolland-Falster were younger and had lower mortality than in-migrants moving out10. However, as out-migrants are relatively young, the absolute number of deaths in this group is small, and mortality estimates unstable. We therefore did not include sub-analysis by socioeconomic groups for out-migrants.
Denmark is a country where fifty years ago a high mortality was found in the inner-city working-class areas, especially in the capital of Copenhagen43. Otherwise throughout the rest of Denmark, health conditions and mortality were fairly similar. Over time, this pattern has been reversed. At present the highest mortality in Denmark is found in the rural area of Lolland-Falster. Our study demonstrated that health-related internal migration was a key component in this reversal. High prices of housing in the capital and suburban areas pushed people on public support, and therefore on low income, to move to areas like Lolland-Falster where prices were lower. This led to an aggregation in Lolland-Falster of unstable people at a high risk of death. The high influx of vulnerable people to Lolland-Falster places a burden on the health care and social support systems in the area. The in-migrants die from the same causes as people in the rest of Denmark, just at a younger age44. Thus, health prevention and treatment in Lolland-Falster cannot be restricted to specific causes; nor to this geographical area as many of the in-migrants’ health complications were established elsewhere.
Conclusion
Economic status was a key factor behind the increasing mortality gap between Lolland-Falster and the rest of Denmark. Two out of five in-migrants to Loland-Falster were on public support, and they had a nine-fold death rate as compared with self-supported people in the rest of Denmark, and a 50% higher mortality than publicly supported people elsewhere in Denmark. Also, self-supported in-migrants to Lolland-Falster was a somewhat selected group with a 50% higher mortality than self-supported people in the rest of Denmark. Over time, this inflow of vulnerable people affected the mortality pattern of long-term residents. While the self-supported long-term residents in 1992–1999 had the same mortality as self-supported people in the rest of Denmark, they had by 2010–2018 a 40% excess mortality. In Denmark, poor health is the main eligibility criteria for public support in working-ages. Thirty years of inflow of this healthwise vulnerable group of citizens affected the mortality generating a gap between Lolland-Falster and the rest of Denmark.
Data availability
Data was extracted from the Danish Health Data Authority and Statistics Denmark. The data that support the findings of this study are available from Statistics Denmark but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data used for this study can be accessed from Statistics Denmark’s Research Service upon reasonable request (e-mail: forskningsservice@dst.dk).
References
Johnson, K. M. & Lichter, D. T. Rural depopulation: Growth and decline processes over the past century. Rural Sociol. 84, 3–27 (2019).
Vaalavuo, M. & Sihvola, M. W. Are the sick left behind at the peripheries? Health Selection in migration to growing urban centres in Finland. Eur. J. Popul. 37, 341–356 (2020).
Yi, Y. et al. Health selectivity and rural-urban migration in china: A nationwide multiple cross-sectional study in 2012, 2014, 2016. Int. J. Environ. Res. Public Health. 16, 1–14 (2019).
Dijkstra, A., Kibele, E. U. B., Verweij, A., Van Der Lucht, F. & Janssen, F. Can selective migration explain why health is worse in regions with population decline?: A study on migration and self-rated health in the Netherlands. Eur. J. Public Health. 25, 944–950 (2015).
Margaras, V. Demographic trends in EU regions. Eur. Parliam. Res. Serv. 2019, 12 (2019).
Statistics Denmark. Population at the First Day of the Quarter by Marital Status, Age, Sex, Region and Time [Internet]. StatBank Denmark. 2022, (accessed 30 Jun 2022); https://www.statbank.dk/hisb7
Statistics Denmark. Life Expectancy for New Born Babies by Municipality 2017:2021 [Internet]. StatBank Denmark. 2022, (accessed 30 Jun 2022); https://www.statbank.dk/hisb7
Danish Health Authority, National Institute of Public Health. Danskernes Sundhed [Health of the Danes] [Internet]. Tal fra Den Nationale Sundhedsprofil [Numbers from the National Health Profile]. 2022, (accessed 30 Jun 2022); https://www.danskernessundhed.dk/
Holmager, T. L. F., Thygesen, L., Buur, L. T. & Lynge, E. Emergence of a mortality disparity between a marginal rural area and the rest of Denmark, 1968–2017. BMC Public Health 90, 1–11 (2021).
Holmager, T. L. F., Lophaven, S. N., Mortensen, L. H. & Lynge, E. Does Lolland-Falster make people sick, or do sick people move to Lolland-Falster? An example of selective migration and mortality in Denmark, 1968–2017. Soc. Sci. Med. 2021, 277 (2021).
The CPR-office. Udtræksvejledning for offentlige brugere [Extraction manuel for public users]. The Central Population Register. Copenhagen 2011, 1–98 (2011).
Statistics Denmark. Socio-Economic Classification (SOCIO13), v1:2014 [Internet]. Classifications. 2022 (accessed 30 Jun 2022); https://www.dst.dk/en/Statistik/dokumentation/nomenklaturer/sociooekonomisk-klassifikation--socio-
Panduro, B. Arbejdsløse og øvrige offentligt forsørgede i kommunerne [Unemployed and other publicly supported in the municipalities]. The Danish Center for Social Science Research. Copenhagen 2017, 1–18 (2017).
Rostgaard, K. Methods for stratification of person-time and events—a prerequisite for Poisson regression and SIR estimation. Epidemiol. Perspect. Innov. 5, 1–16 (2008).
The Danish Ministry of Health & The Danish Regions. Søg om sundhedsdata til forskning ét sted [Apply for health data for research one in place] [Internet]. Én indgang til sundhedsdata [One entrance for health data]. 2022 (accessed 15 Jul 2022); https://www.enindgangtilsundhedsdata.dk/da-DK/Services/Ansoegningsportalen#213868F815044FB18A3F92AB9A951946
The Danish Health Data Authority. Lovgivning og tilladelser [Laws and permissions] [Internet]. Forskerservice [Rearch service]. 2022 (accessed 15 Jul 2022); https://sundhedsdatastyrelsen.dk/da/forskerservice/for-du-soger
Borger.dk. Hvem kan få førtidspension? [Who are entitled to early retirement pension?] [Internet]. Førtidspension [Early retirement pension]. 2022 (accessed 30 Jun 2022); https://www.borger.dk/pension-og-efterloen/Foertidspension-oversigt/Hvem-kan-faa-foertidspension-og-seniorfoertidspension
Hattersley, L. & Creeser, R. Longitudinal study 1971–1991: History, organisation and quality of data. ONS Ser. 1995, 1–374 (1995).
Riva, M., Curtis, S. & Norman, P. Residential mobility within England and urban-rural inequalities in mortality. Soc. Sci. Med. 73, 1698–1706 (2011).
Popham, F., Boyle, P. J., O’Reilly, D. & Leyland, A. H. Selective internal migration. Does it explain Glasgow’s worsening mortality record?. Heal. Place. 17, 1212–1217 (2011).
Gartner, A. et al. Does selective migration alter socioeconomic inequalities in mortality in Wales?: A record-linked total population e-cohort study. SSM Popul. Heal. 5, 48–54 (2018).
Brimblecombe, N., Dorling, D. & Shaw, M. Mortality and migration in Britain, first results from the British Household Panel Survey. Soc. Sci. Med. 49, 981–988 (1999).
Andersson, G. & Drefahl, S. Long-distance migration and mortality in Sweden: Testing the salmon bias and healthy migrant hypotheses. Popul. Space Place. 2017, 23 (2017).
Baigi, A. & Holmen, A. Internal migration and the risk of death: Impact of socio-epidemiological factors in a long living Swedish Population. Epidemiol. Open Access. 8, 1–7 (2018).
Baigi, A., Holmén, A., Högstedt, B., Odén, A. & Herrström, P. Birthplace and social characteristics as risk factors for acute myocardial infarction in the province of Halland, Sweden. Public Health 116, 279–284 (2002).
Saarela, J. & Finnäs, F. Internal migration and mortality: The case of Finland. Environ. Health Insights. 2, 1–12 (2008).
Carstensen, B. Who needs the Cox model anyway? Steno Diabetes Center Copenhagen & Department of Biostatistics, University of Copenhagen. Gentofte 2019, 1–31 (2019).
Marmot, M. The Health Gap—The Challenge of an Unequal World 1–389 (Bloomsbury Publishing Plc, 2016).
Paul, K. I. & Moser, K. Unemployment impairs mental health: Meta-analyses. J. Voca. Behav. 74, 264–282 (2009).
Juul, J. S. & Blicher, S. P. Folk i job fraflytter udkanten og folk uden job kommer til [People in jobs move away from margianl areas and people without jobs move in]. The Economic Council of the Labour Movement. Copenhagen 2017, 1–14 (2017).
Caspersen, S. Hørsholms tilflyttere er dobbelt så rige som Lollands [Hørsholm’s newcomers are twice as rich as Lolland’s]. The Economic Council of the Labour Movement. Copenhagen 2021, 1–6 (2021).
Hansen, J. Z. & Østergaard, A. Ejerboliger i det 21, århundrede [Owner-occupied homes in the 21st century]. The Knowledge Centre for Housing Economics. Copenhagen 2018, 1–38 (2018).
The National Building Fund. Huslejestatistik 2020 [Rent statistics 2020]. Copenhagen 2020, 1–53 (2020).
Sabiers, S. E. & Amin, S. N. Ulighed: De fattigste danskere er blevet fattigere [Inequality: The poorest Danes have become poorer]. The Economic Council of the Labour Movement. Copenhagen 2013, 1–7 (2013).
Keeley, B. What’s happening to income inequality? Income inequality: The gap between rich and poor 31–39 (OECD Publishing, 2015).
Stringhini, S. et al. Socioeconomic status and the 25 × 25 risk factors as determinants of premature mortality: A multicohort study and meta-analysis of 1·7 million men and women. Lancet 389, 1229–1237 (2017).
Brønnum-Hansen, H. & Baadsgaard, M. Widening social inequality in life expectancy in Denmark. A register-based study on social composition and mortality trends for the Danish population. BMC Public Health 2012, 12 (2012).
Danish Health Authority, National Institute of Public Health. Social ulighed i sundhed og sygdom [Social inequality in health and disease]. Udviklingen i Danmark i perioden 2010–2017 [The development in Denmark during the period 2010–2017]. Copenhagen 2020, 1–266 (2020).
Vineis, P. & Kelly-Irving, M. Biography and biological capital. Eur. J. Epidemiol. 34, 979–982 (2019).
Toch-Marquardt, M. et al. Occupational class inequalities in all-cause and cause-specific mortality among middle-aged men in 14 European populations during the early 2000s. PLoS ONE 2014, 9 (2014).
Marmot, M. G. et al. Health inequalities among British civil servants: The Whitehall II study. Lancet 337, 1387–1393 (1991).
Statistics Denmark. Internal migration between municipalities by sex, age and municipality [Internet]. StatBank Denmark. 2022 (accessed 24 Oct 2022); https://www.statistikbanken.dk/statbank5a/selectvarval/define.asp?MainTable=FLY66&PLanguage=0&Tabstrip=&PXSId=0&SessID=394049772&FF=20&grouping3=20063915132215154453&tfrequency=1
Juel, K. Dødeligheden i Danmark gennem 100 år [Mortality in Denmark during 100 years]. National Institute of Public Health. Copenhagen; 2004.
Holmager, T. L. F., Nymand Lophaven, S., Mortensen, L. H. & Lynge, E. Temporal trends in cause-specific mortality in a rural-provincial area of Denmark, Lolland-Falster, 1970–2018. Scand. J. Public Health 2022, 1–9 (2022).
Funding
This study was financially supported by the Danish Health Fund (Grant number: 20-B-0023).
Author information
Authors and Affiliations
Contributions
All authors came up with the idea for the study. T.L.F.H. carried out the analysis. S.N.L. and E.L. provided input for the analysis. T.L.F.H. and E.L. wrote the first draft. All authors read and approved the submitted manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Holmager, T.L.F., Lophaven, S.N., Mortensen, L.H. et al. Selective migration and mortality by economic status in Lolland-Falster, Denmark, 1992–2018. Sci Rep 12, 19970 (2022). https://doi.org/10.1038/s41598-022-24635-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-24635-2
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
