
Abstract
To examine the effects of different PM2.5 concentration ranges on daily all-cause mortality, 8768 all-cause deaths were recorded in the database of the Shandong Provincial Hospital Affiliated to Shandong First Medical University. Data of air pollutants (PM2.5 and O3) concentration were provided by the Jinan Environment Monitoring Center. The relative risk of all-cause mortality was assessed using a quasi-Poisson regression model after adjusting for confounding factors. The concentrations of PM2.5 were divided into four ranges 0–35 μg/m3; 35–75 μg/m3; 75–115 μg/m3; 115–150 μg/m3. There was no significant relationship between PM2.5 exposure and all-cause deaths in individuals aged < 60 years. However, for individuals aged ≥ 60 years, there was a significant positive association between exposure concentrations and all-cause deaths within the ranges 0–35 μg/m3, 35–75 μg/m3, and 115–150 μg/m3 with a mortality increase of 1.07 (1.01, 1.13), 1.03 (1.00, 1.05), and 1.05 (1.01, 1.08), respectively. When the population aged ≥ 60 years was stratified into gender groups, exposure to PM2.5 in the range 0–35 μg/m3 increased the mortality risk in men but not women. All-cause mortality in women, but not men, increased significantly with exposure to PM2.5 in the ranges of 35–75, 75–115, and 115–150 μg/m3.
Similar content being viewed by others


Introduction
Particulate matter in the air refers to the dispersed solid, liquid or solid–liquid suspended body in the air. Particulate matter in the air is divided into coarse particulate matter PM10 (aerodynamic diameter below 10 μm), fine particulate matter PM2.5 (aerodynamic diameter below 2.5 μm), and ultrafine particles (aerodynamic diameter less than 0.1 μm). The toxicity and pathogenicity of particulate matter are closely related to its diameter composition and source. PM2.5 is mainly caused by the burning of fossil fuels such as oil, coal or wood. The particles produced by power plants, industrial production, residential heating and motor vehicle driving are usually composed of carbon, transition metals complex organic molecules, sulfate and nitrate. Soluble components (ultrafine particulate matter) of PM2.5 can enter the blood circulation through the alveolar capillaries, while insoluble components can be deposited in the lungs, obstruct airflow and affect the respiratory system1,2,3.
O3 is formed by photochemical reactions of oxidants and hydrocarbons in the atmosphere under the catalysis of sunlight. As a major component of acid rain and photochemical smog, the strong oxidation of O3 can cause serious damage to cell walls and have acute effects on the lungs and respiratory system. There is ample evidence that ground-level ozone impairs lung function and stimulates the respiratory system3,4,5. Exposure to ozone (and the pollutants that produce it) is significantly associated with premature death, asthma, bronchitis, heart attacks and other heart and lung problems.
The adverse effects of airborne particulate matter ≤ 2.5 µm, PM2.5 on public health, especially in the respiratory and cardiovascular systems, have been studied for nearly half a century. The formation of PM2.5 and its adverse impact on public health are evident in both developed and developing countries6,7,8. Various studies in Europe, the United States, and developing countries such as China, India, and Korea found that entire populations were affected by short-term exposure to fine particulate matter and that there was a positive correlation between PM2.5 levels and mortality9,10,11,12,13,14. In addition, substantial epidemiological evidence demonstrates that ground-level fine particulate matter is linked to various respiratory diseases, including asthma, chronic obstructive pulmonary disease, lung cancer15,16,17, and cardiovascular mortality18,19,20.
However, the results of all-cause mortality associated with exposure to PM2.5 are inconsistent; therefore, public awareness of the risk of this type of exposure is low21,22,23. Moreover, few studies to date investigated the PM2.5 ranges that poses no health risk. For this reason, a recommended PM2.5 concentration is needed to minimize the adverse health effects24.
The objective of this study is to examine the effects of different PM2.5 ranges on all-cause mortality and provide public health recommendations to avoid exposure to PM2.5.
Materials and methods
Data source
Daily concentrations of PM2.5 in 24-h intervals and ozone (O3) in 1-h intervals averaged in urban areas of Jinan, China, from 2013 to 2015, were obtained from 14 permanent air quality monitoring stations of Jinan Environmental Protection Bureau. PM2.5 is monitored by Beta attenuation monitoring technique, light scattering, and micro oscillatory balance method, O3 is monitored by spectrophotometry, ultraviolet spectrophotometry, and chemiluminescence method, at each air quality monitoring stations under supervision of Jinan Environmental Protection Bureau. Also, the use of monitors follows the Technical specifications for operation and quality control of ambient air quality automated monitoring system for particulate matter. Daily mean air temperatures and relative humidity in the corresponding period were provided by the Jinan Bureau of Meteorology. We use expectation maximization to make up for the missing values.
Data on the daily mortality of the registered population of Jinan for the period 2013–2015 were recorded in the database of Shandong Provincial Hospital Affiliated to Shandong First Medical University. Detailed demographic information, including age, gender, date of hospital admission, date of hospital discharge, admission diagnosis, discharge diagnosis codes, and current residence. Mortality data on total non-accidental causes (codes A00–R99), cardiovascular disease (codes I00–I99), and respiratory disease (codes J00–J98) were classified according to International Classification of Diseases Tenth Revision 10 (ICD-10). The data on all-cause mortality were stratified by gender (male and female) and age (< 60 and ≥ 60 years).
Data analysis
PM2.5 concentrations were classified into four ranges: 0–35 μg/m3, 35–75 μg/m3, 75–115 μg/m3 and 115–150 μg/m3—based on the Chinese new air quality index (AQI) (GB3095-2012) released by the Ministry of Environmental Protection (MEP). To establish the four PM2.5 concentration ranges, we set all concentrations outside the range as “NA”.
A quasi-Poisson regression model with natural splines was used to assess the impact of different PM2.5 ranges on daily all-cause mortality because the daily death counts in Jinan approximately followed a Poisson distribution. This regression model is used to adjust inference for overdispersion25. The natural cubic spline for mean temperatures with 5 degrees of freedom and relative air humidity with 3 degrees of freedom (df) was controlled to analyze all-cause mortality based on Akaike’s Information Criterion (AIC) for lag effects of up to 3 days26. Confounding factors such as day of the week and holidays were included as dummy variables.
The natural cubic spline smoothing function degree of freedom for mean temperature and relative air humidity is determined as follows:
Yt represents the death counts on day t. E(Yt) represents the expected death counts on day t, ns stands for the natural cubic spline smoothing function, Temp represents the mean temperature, RH represents the relative air humidity, DOW and Holiday stands for the day of the week effect and legal holidays respectively, β1 and β2 are the coefficient of DOW and Holiday respectively. The degree of freedom of the mean temperature factor is N (N = 2,3,…,6). Obtain the magnitude of the corresponding AIC of the equation when N is different, and the minimum value of AIC is the optimal degree of freedom.
Different PM2.5 ranges were added into the above basic model to establish a single-pollutant model. Multi-pollutant models with PM2.5 and O3, with multi-day moving average lag structures [from a lag of 0 to 1 day (mean) to a lag of 0 to 3 days (mean)], were used for sensitivity analysis to determine the stability of the model.
The relative risk (RR) and corresponding 95% confidence interval (CI) for an increase of 10 μg/m3 in pollutant concentration were estimated to assess the impact of different PM2.5 ranges on daily counts of all-cause mortality. P-values smaller than 0.05 were considered statistically significant.
Stratified analyses of exposure to different PM2.5 ranges based on gender (male or female) and age (< 60 years and ≥ 60 years) were performed to find associations with daily all-cause mortality.
Results
Distribution of ambient pollutants and weather data
The mean daily concentrations of PM2.5 and O3 from 2013 to 2015 were 96 μg/m3 and 102.4 μg/m3, and these values are 1.28- and 0.64-fold higher than those reported by the new Chinese ambient air quality standards (GB3095-2013). The levels of PM2.5 in 625 of 1095 days exceeded the annual secondary national 24-h ambient air quality standards (75 μg/m3). The frequency distribution of daily ambient pollutant levels and temperatures are shown in Fig. 1.

Distribution of daily ambient pollutant concentrations and temperature in Jinan, China, from 2013 to 2015.
Data description
A total of 8768 all-cause deaths (5462 men and 3306 women) for the period 2013–2015 were recorded in the database of Shandong Provincial Hospital Affiliated to Shandong First Medical University. The percentage of individuals aged < 60 and ≥ 60 years was 38.79% (3401/8768) and 61.21% (5367/8768), respectively. The distributions of the daily concentrations of air pollutants, weather parameters, and deaths are shown in Table 1.
According to MEP, air quality was good (green category) in 4.11% of the days, moderate (yellow category) in 38.36% of the days, poor for sensitive groups (orange category) in 32.24% of the days, poor (red category) in 12.42% of the days, and very poor (purple category) in 12.88% of the days for all populations. PM25 concentration and air quality index values in the study period are shown in Table 2.
Daily all-cause mortality
For individuals aged ≥ 60 years, there were strong associations between exposures on lag days 0, 1, 2, and 3 and means of lags 0–1, 0–2 and 0–3 to the three PM2.5 concentrations ranges 0–35, 35–75, and 115–150 μg/m3. The statistically significant relative risks (RR) with 95% confidence intervals (CI) for daily all-cause mortality from exposure to the three PM2.5 ranges were 1.07 (1.01, 1.13), (lag 1, 0–35 μg/m3), 1.03 (1.00, 1.05), (lag 0, 35–75 μg/m3) and 1.05 (1.01, 1.08), (lag 0, 115–150 μg/m3). For a moving average lag structure of 01 the statistically significant relative risks RR (95% CI) for daily all-cause mortality from exposure to PM2.5 in the ranges of 0–35, 35–75, and 115–150 μg/m3 were 1.10 (1.02, 1.18), 1.04 (1.01, 1.07), and 1.06 (1.02, 1.11) respectively. Furthermore, RR (95% CI) for daily all-cause mortality from exposure to 115–150 μg/m3 of PM2.5 was 1.06 (1.01, 1.11) in lag 02 (Table 3).
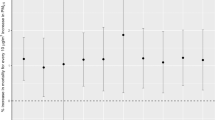
Stratified analysis based on gender and age indicated that there was a significant relationship between all-cause mortality and a PM2.5 range of 0–35 μg/m3 in men in lags 1 and 01. All-cause deaths in women significantly increased with exposure to PM2.5 in the ranges of 35–75 μg/m3, 75–115 μg/m3, and 115–150 μg/m3 in lag 1; lags 0 and 01; and lags 0, 1, 01, 02, and 03, respectively. There were no significant associations between PM2.5 exposure and all-cause mortality in individuals aged < 60 years. All-cause deaths in individuals aged ≥ 60 years were significantly correlated with exposure to ranges of 35–75 μg/m3, 75–115 μg/m3, and 115–150 μg/m3 in lags 1 and 01; lags 1 and 01; and lags 0 and 01, respectively (Fig. 2).

Lag structures of age and gender-specific relative risk (RR) of daily mortality from exposure to different PM2.5 ranges. a0–35 μg/m3, b35–75 μg/m3, c75–115 μg/m3, d115–150 μg/m3. *p < 0.05.
The results of sensitivity analysis indicated that the relative risk at different PM2.5 ranges for daily all-cause mortality generally decreased slightly after including O3 in the multi-day moving average lag structures (Fig. 3). This may be related to the strong collinearity between different Pollutants. Some studies also believe that dual-pollutant models will increase the standard deviation of model fitting, so the significance of statistical analysis is weak27.

Lag structures of relative risk (RR) and 95% confidence interval (CI) between single pollutant models and two-pollutant models for different PM2.5 ranges in lag 0 to lag 03. a0–35 μg/m3, b35–75 μg/m3, c75–115 μg/m3, d115–150 μg/m3. *p < 0.05.
Discussion
To our knowledge, this epidemiologic study is the first to examine the association of PM2.5 concentration ranges with all-cause mortality in Asia. The results indicated that, except for the PM2.5 range of 75–115 μg/m3, the concentrations of PM2.5 in the ranges 0–35 μg/m3, 35–75 μg/m3, and 115–150 μg/m3 were significantly associated with mortality from all causes for individuals aged ≥ 60 years. At the optimum lag structure, the statistically significant relative risks RR (95% CI) for daily all-cause mortality from exposure in the ranges 0–35 μg/m3, 35–75 μg/m3, and 115–150 μg/m3 of PM2.5 were 1.10 (1.02, 1.18), 1.04 (1.01, 1.07), and 1.06 (1.02, 1.11) respectively. This indicated that the adverse impacts on public health do not decrease as pollutant levels decrease. The statistically significant relative risks RR (95% CI) for daily all-cause mortality from exposure in the range 0–35 μg/m3 of PM2.5 were 1.10 (1.02, 1.18). This means that in the concentration range of 0 to 35 μg/m3, the effects of PM2.5 were stronger as the concentration increased. In the same way, in the concentration ranges of 35 to 75 μg/m3 and 115 to 150 μg/m3, we can get the same conclusion. . In addition, as shown in Table 3, in the PM2.5 concentration range of 0 to 35 μg/m3, RR (95% CI) for daily all-cause mortality was 1.10 (1.02, 1.18), and Fig. 2 indicated that there was a significant relationship between all-cause mortality and a PM2.5 range 0–35 μg/m3 in men and individuals aged ≥ 60 years in lags 1 and 01, both of these indicated that consistent with other studies28,29,30, even for concentrations lower than 35 μg/m3, PM2.5 is a significant risk factor for all-cause mortality.
For individuals aged ≥ 60 years, the association between all-cause deaths and PM2.5 exposures was statistically significant at ranges of 0–35 μg/m3, 35–75 μg/m3, and 115–150 μg/m3. The lack of significance in the 75–115 μg/m3 range may be because of the relatively fewer deaths in this range. Furthermore, the daily temperatures corresponding to concentrations of 75–115 μg/m3 were higher than those at 0–35, 35–75, and 115–150 μg/m3. The impact of different PM2.5 ranges on mortality may be due to differences temperatures31,32.
The results of a previous study on the gender-specific effects of particulate matter were inconsistent33. The results of the gender-stratified analysis demonstrated that female subjects were more sensitive to the PM2.5 in the ranges of 35–75 μg/m3, 75–115 μg/m3, and 115–150 μg/m3, whereas male subjects were more sensitive to PM2.5 in the range of 0–35 μg/m3, indicating that men are more susceptible to lower PM2.5 concentrations than women. Smoking is a critical environmental risk factor, and one study suggested that the estimated impact of air pollution might be stronger in nonsmokers than smokers34. A potential reason for this difference may be that women have slightly stronger airway reactivity and smaller airways than men35. Moreover, the adverse impacts of additional exposure to PM2.5 may be overcome by the oxidative and inflammatory effects of smoking36.
Older individuals had increased susceptibility to PM2.5 ranges of 35–75 μg/m3, 75–115 μg/m3, and 115–150 μg/m3 compared with younger individuals, possibly because the former group has a weaker immune system and higher sensitivity to these particles37,38. However, there was no significant association between PM2.5 exposure and all-cause mortality in individuals aged < 60 years, indicating that the general population should avoid high levels of PM2.5 (≥ 75 μg/m3).
This study has some limitations. First, the study selected the mean air pollutant concentration from each monitoring site in Jinan as the exposure concentration; nonetheless, individual exposure may depend on other factors, including the type of outdoor activity, physical fitness, and living habits, potentially causing exposure measurement errors or underestimating the impact of air pollution. In addition, this study belongs to the field of ecological research, and the conclusions cannot prove causality but merely indicate the relationship between air pollutants and all-cause mortality.
Conclusions
There was no significant relationship between PM2.5 exposure and all-cause deaths in individuals aged < 60 years. However, for individuals aged ≥ 60 years, there was a significant positive association between exposure concentrations and all-cause deaths within the ranges 0–35 μg/m3, 35–75 μg/m3, and 115–150 μg/m3 with a mortality increase of 1.07 (1.01, 1.13), 1.03 (1.00, 1.05), and 1.05 (1.01, 1.08), respectively. When the population aged ≥ 60 years was divided into gender groups, exposure to PM2.5 in the range 0–35 μg/m3 increased the mortality risk in men but not women. All-cause mortality in women, but not men, increased significantly with exposure to PM2.5 in the ranges of 35–75, 75–115, and 115–150 μg/m3.
References
Dons, E. et al. Concern over health effects of air pollution is associated to NO2 in seven European cities. Air Qual. Atmos. Health 11(5), 591–599 (2018).
Gao, H. et al. Analysis of the air quality and the effect of governance policies in China’s Pearl River Delta, 2015–2018. Atmosphere 10(7), 412 (2019).
Zheng, S. et al. The effect of a new subway line on local air quality: A case study in Changsha. Transp. Res. D Transp. Environ. 68, 26–38 (2019).
DeFlorio-Barker, S. et al. Acute effects of short-term exposure to air pollution while being physically active, the potential for modification: A review of the literature. Prev. Med. 139, 106195 (2020).
Yang, J. & Xu, L. How does China’s air pollution influence its labor wage distortions? Theoretical and empirical analysis from the perspective of spatial spillover effects. Sci. Total Environ. 745, 140843 (2020).
Brunekreef, B. Air pollution and health. Ned. Tijdschr. Geneeskd. 162, 27 (2018).
Cascio, W. E. & Long, T. C. Ambient air quality and cardiovascular health: Translation of environmental research for public health and clinical care. N. C. Med. J. 79(5), 306–312 (2018).
Kim, M. J. The effects of transboundary air pollution from China on ambient air quality in South Korea. Heliyon 5(12), e02953 (2019).
Son, J. Y. & Bell, M. L. The relationships between short-term exposure to particulate matter and mortality in Korea: Impact of particulate matter exposure metrics for sub-daily exposures. Environ. Res. Lett 8(1), 014015 (2013).
Loxham, M., Davies, D. E. & Holgate, S. T. The health effects of fine particulate air pollution: The harder we look, the more we find. Br. Med. J. 367, l6609 (2019).
Duan, R.-R., Hao, K. & Yang, T. Air pollution and chronic obstructive pulmonary disease. Chronic Dis. Transl. Med. 6(4), 260–269 (2020).
Zhao, W. Effect of air pollution on household insurance purchases. Evidence from China household finance survey data. PLoS ONE 15(11), e0242282 (2020).
Mehdi, F. et al. Long term exposure to ambient air particulate matter and mortality effects in Megacity of Tehran, Iran: 2012–2017. Particuology 58, 139–146 (2021).
Tayebeh, K. et al. Association of short-term exposure to air pollution with mortality in a middle eastern tourist city. Air Qual. Atmos. Health 13, 1223–1234 (2020).
Fan, J. et al. The impact of PM2.5 on asthma emergency department visits: A systematic review and meta-analysis. Environ. Sci. Pollut. Res Int. 23(1), 843–850 (2016).
Hu, W. et al. Contribution of regional PM2.5 transport to air pollution enhanced by sub-basin topography: A modeling case over Central China. Atmosphere 11(11), 1258 (2020).
Wu, X. et al. Effect of air pollution on the stock yield of heavy pollution enterprises in China’s key control cities. J. Clean. Prod. 170, 399–406 (2018).
David Hu, J. J. PM25 Pollution and risk for lung cancer: A rising issue in China. J. Environ. Prot. 5, 731 (2014).
Khilnani, G. C. & Tiwari, P. Air pollution in India and related adverse respiratory health effects: Past, present, and future directions. Curr. Opin. Pulm. Med. 24(2), 108–116 (2018).
Liu, Y. et al. A multicity analysis of the short-term effects of air pollution on the chronic obstructive pulmonary disease hospital admissions in Shandong, China. Int. J. Environ. Res. Public Health 15(4), 774 (2018).
Kan, H. & Shi, X. Research progress of ambient air pollution and human health in China. Zhonghua Yufang Yixue Zazhi 53(1), 4–9 (2019).
Wang, Z. et al. Impact of air pollution waves on the burden of stroke in a megacity in China. Atmos. Environ. 202, 142–148 (2019).
Hunter, P., The health toll of air pollution Despite global efforts to clean up the air, outdoor and indoor air pollution still have a drastic negative effect on public health. Embo Reports, 2020. 21(8).
Leon, A. C., Davis, L. L. & Kraemer, H. C. The role and interpretation of pilot studies in clinical research. J. Psychiatr. Res. 45(5), 626–629 (2011).
Zhang, X. Y. & Jie, J. L. The effect of group mindfulness therapy on sleep quality and job burnout among nurses. J. Nurses Train 29, 1419–1420 (2014).
Hurvich, C. M., Simonoff, J. S. & Tsai, C. L. Smoothing parameter selection in nonparametric regression using an improved akaike information criterion. J. R. Stat. Soc. 60(2), 271–293 (1998).
赵庆国,梁志江,李兵,杜玉开.某市空气污染对早产急性影响的Poisson广义可加模型分析[J].环境与健康杂志. 27(06), 488–492 (2010).
Chowdhury, S. & Dey, S. Cause-specific premature death from ambient PM2.5 exposure in India: Estimate adjusted for baseline mortality. Environ. Int. 91, 283–290 (2016).
Schwartz, J. et al. The effect of dose and timing of dose on the association between airborne particles and survival. Environ. Health Perspect. 116(1), 64–69 (2008).
Shi, L. et al. Low-concentration PM2.5 and mortality: Estimating acute and chronic effects in a population-based study. Environ. Health Perspect. 124(1), 46–52 (2016).
Azhar, G. S. et al. Heat-related mortality in India: Excess all-cause mortality associated with the 2010 Ahmedabad heat wave. PLoS ONE 9(3), e91831 (2014).
Rathi, S. K. et al. Summer temperature and spatial variability of all-cause mortality in Surat City, India. Indian J. Community Med. 42(2), 111–115 (2017).
Clougherty, J. E., Souza, K. & Cullen, M. R. Work and its role in shaping the social gradient in health. Ann. N. Y. Acad. Sci. 1186, 102–124 (2010).
Nino, K. et al. Ambient air pollution and atherosclerosis in Los Angeles. Environ. Health Perspect. 113(2), 201–206 (2005).
Bhatawadekar, S. A. et al. Reduced baseline airway caliber relates to larger airway sensitivity to rostral fluid shift in asthma. Front. Physiol. 8, 1012 (2017).
Chen, R. et al. Association of particulate air pollution with daily mortality: The China air pollution and health effects study. Am. J. Epidemiol. 175(11), 1173–1181 (2012).
Ariana, Z., Antonella, Z. & Joel, S. Individual-level modifiers of the effects of particulate matter on daily mortality. Am. J. Epidemiol. 163(9), 849–859 (2006).
Franklin, M., Zeka, A. & Schwartz, J. Association between PM2.5 and all-cause and specific-cause mortality in 27 US communities. J. Expo Sci. Environ. Epidemiol. 17(3), 279–287 (2007).
Acknowledgements
We wish to thank Lv Chenguang and Zhou Tianran for advice on experimental design.
Funding
This work was supported by the National Key Research and Development Program (2019YFE0117800), the Shandong Provincial Key Research and Development Program (2021CXGC010506), the National Natural Science Foundation of China (22176115), Cultivating Fund for NSFC of Shandong Provincial Qianfoshan Hosipital (QYPY2019NSFC0603), and Natural Foundation of Shandong Provincial Natural Science Foundation (ZR2021QH290).
Author information
Authors and Affiliations
Contributions
M.Z. and M.X. performed most of the investigation, data analysis and wrote the manuscript; C.C. contributed to scoping and structuring the paper and guided method development; C.B. provided research data; L.W. provided pathological assistance; Z.C. contributed to the interpretation of the data and analyses, L.W. and Z.C. are corresponding teachers. All of the authors have read and approved the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ma, Z., Meng, X., Chen, C. et al. Short-term effects of different PM2.5 ranges on daily all-cause mortality in Jinan, China. Sci Rep 12, 5665 (2022). https://doi.org/10.1038/s41598-022-09057-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-09057-4
This article is cited by
-
The changing health effects of air pollution exposure for respiratory diseases: a multicity study during 2017–2022
Environmental Health (2024)
-
Analyzing the complementarity between thermal improvement and the replacement of wood-burning heaters to reduce outdoor air pollution
International Journal of Environmental Science and Technology (2024)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
