
Abstract
Disproportionately enlarged subarachnoid space hydrocephalus (DESH) is the characteristic feature of idiopathic normal pressure hydrocephalus. We aimed to characterize the prevalence, development, and association of DESH to cognitive deficit in a large population. We reviewed the data of 1384 subjects eligible for the present study among 1590 participants who underwent magnetic resonance imaging (MRI) in the Ohasama Study, a population-based study in Ohasama, Japan. The participants with Mini-Mental State Examination (MMSE) score < = 25 were assumed to have cognitive deficit and DESH was evaluated by reviewing the MRIs. We assessed the association between DESH, Evans index (EI), and cognitive deficit using multivariate logistic regression models adjusted for relevant confounders. Furthermore, we evaluated the new development of DESH and the deterioration of cognitive function in the participants with DESH. There were nine participants with DESH (0.65%), seven of whom showed cognitive deficit. DESH was significantly associated with cognitive deficit in multivariate regression analyses (odds ratio; 8.50 [95% confidence interval: 1.61–44.88]). In the 669 participants who underwent follow-up MRI, we found four participants newly presenting with DESH; the development of DESH was observed before/after the presence of EI > 0.3. We also found two participants with existing DESH showing no remarkable worsening in MMSE and EI. The present study demonstrated a positive association between the presence of DESH and cognitive deficit. DESH can develop independently of EI > 0.3, and ventricular enlargement in combination with DESH may be an important factor in the worsening of cognitive deficit.
Similar content being viewed by others
Introduction
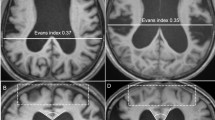
Idiopathic normal pressure hydrocephalus (iNPH) is known to be a cause of treatable dementia and gait disturbance in elderly patients. For diagnosis of iNPH, the Evans Index (EI) has been widely used to estimate the size of cerebral ventricles1, initially described in 1942 as a linear ratio of the maximum width of the frontal horns of the lateral ventricles and the maximal internal diameter of the skull at the same level. Normal values of the EI fall between 0.20 and 0.25, and values above 0.30 indicate definite ventricular enlargement2. Consensus guidelines have been accepted that an EI > 0.3 is one of the neuroimaging requisites for the diagnosis of NPH3. In addition to an EI > 0.3, when a characteristic pattern of “disproportionate enlargement of the inferior subarachnoid spaces with tight high-convexity subarachnoid spaces” is observed, it is called disproportionately enlarged subarachnoid space hydrocephalus (DESH)4,5. The presence of DESH has been proposed to be a potential iNPH-related feature4. So far, a few studies have reported the prevalence of DESH6,7,8, and studies on the association between the presence of DESH and cognitive impairment in a general population are still insufficient9. We have previously reported that cognitive function in participants with DESH was significantly lower than that in participants with standard magnetic resonance imaging (MRI) findings in a univariate study by observing 506 participants aged 75 years in a community-based birth cohort investigation of the Vienna Trans-Danube Aging study8. The present study, therefore, aimed to reveal the prevalence of DESH and its association with cognitive deficit using multivariate logistic regression models in a general population. Furthermore, we followed up the participants and evaluated the new development of DESH along with the change of cognitive function in the participants with DESH.
Methods
Design
The present study is a part of the Ohasama Study, which started in 1987 in Ohasama, Japan; the details of this ongoing cohort have been described previously10,11. The institutional review boards of Tohoku University School of Medicine, Kyoto Koka Women’s University, and the Department of Health of the Ohasama Municipal Government approved the study.
Subjects
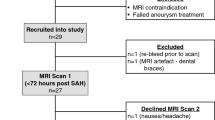
We used data of the participants who provided informed consent and underwent MRI between 1992 and 2016 (n = 1590). Of those, 18 individuals under 55 years of age were excluded because the surveys on MRI and MMSE were mainly performed in the participants over 55 years old in Ohasama study. Moreover, the participants with missing data on the Mini-Mental State Examination (MMSE) (n = 58), and incomplete answers (n = 130). Thus, data of 1,384 participants were eligible for the analyses in the present cross-sectional study (Fig. 1). Among these participants, 669 underwent an MRI and MMSE in the follow-up surveys.

Overview of the study population.
The Japanese version of MMSE was administered to evaluate cognitive function; the details have been described previously12. The subjects with a score of < = 25 were assumed to have cognitive deficit in the present study13; in addition, those with scores < = 26 and < = 24 were also assessed.
MRI scanning and evaluation
Images were collected using a Toshiba MRT-50A with a 0.5-T superconducting magnet (Toshiba Medical, Tokyo, Japan)14. EI was measured as the ratio of the maximal width of the frontal horns to the internal diameter of the cranium2. DESH was diagnosed following the general definition: “disproportionate enlargement of the inferior subarachnoid spaces with tight high-convexity subarachnoid spaces” and “EI > 0.3” on the MRI4,5. We sometimes observe “disproportionate enlargement of the inferior subarachnoid spaces with tight high-convexity subarachnoid spaces” in case the EI is 0.29 or so at outpatient clinics. We therefore conducted further analyses to determine if the criterion of EI for diagnosing DESH should be expanded to > 0.28 (“DESH-expanded”). A neurologist (I. A.) and a neurosurgeon (T. N.) independently reviewed MRI recordings from all participants of this study blinded to their clinical information. Disagreement in assessment was resolved by consensus after discussion. The inter-observer reproducibility value for DESH and the kappa coefficient were calculated.
Statistical analysis
We calculated the odds ratios (ORs) of EI (> 0.3/ = < 0.3) and DESH (presence/absence) for the prevalence of cognitive deficit using multivariate logistic regression analysis, adjusting for age, sex, history of cerebrovascular diseases (CVD), history of hypertension, history of diabetes mellitus, history of hyperlipidemia, smoking history, drinking history, and duration of education. The duration of education was categorized as being either less than or at least 10 years. We conducted the same analysis on the association between DESH-expanded and cognitive deficit. All significance tests were two-tailed, and p < 0.05 was considered significant in all analyses. All statistical analyses were performed with IBM SPSS Statistics for Windows version 25 (IBM Corp., Armonk, NY).
Ethics approval
This study conforms to the Helsinki declaration. The Institutional Review Boards of Teikyo University, Tohoku Medical and Pharmaceutical University, and Tohoku University approved the study protocol.
Consent to participate
Informed consent was obtained from all individual participants included in the study.
Results
The inter-observer reproducibility value for DESH was 0.99 and the kappa coefficient of the inter-observer reliability was 0.68. There were 92 participants with EI > 0.3 (6.6%), which was significantly associated with age, sex, history of CVD, history of hyperlipidemia, smoking history, and drinking history (Table 1). The prevalence of EI > 0.3 increased with age group, and it was higher in men than in women in all age groups (Table 2). Among the 92 participants with EI > 0.3, nine subjects presented with DESH, so the prevalence of DESH was 0.65% (9/1384) in this population. Seven of them were included in the criteria for cognitive deficit. The presence of DESH was not associated with the relevant variables (Table 1); however, the prevalence of DESH and DESH-expanded tended to increase with age (Table 2).
The median EI and MMSE were 0.261 (interquartile range, 0.245–0.277) and 28 (interquartile range, 25–29), respectively, in this population. Not only EI > 0.3 but also EI > 0.28 was not associated with cognitive deficit in multivariate logistic regression analyses. In contrast, DESH was associated with cognitive deficit not only in univariate but also in multivariate logistic regression analyses (Table 3). These results were also statistically significant even if the criteria of cognitive deficit were changed (MMSE = < 24 or = < 26), or if the criterion of EI for diagnosing DESH was expanded to > 0.28.
We followed up 669 participants (451 women and 218 men; follow-up period [mean ± s.d.] 8.89 ± 4.55 years, min. 2.6 and max. 24.9), and found 4 participants newly presenting with DESH (two men and two women; mean age: 66.3 years; mean EI, 0.305); the development of DESH was observed before/after the presence of EI > 0.3 (Table 4). Moreover, we also evaluated the deterioration of cognitive function in the participants with DESH in the baseline surveys.
We could follow up only two of the nine participants with DESH and found that their MMSE did not change a lot and that their MRI findings were not accompanied by remarkable EI changes either (63.9-year-old man: MMSE 21–20 and EI 0.317–0.324 for 4 years; 55.7-year-old man: MMSE 27–27 and EI 0.355–0.335 for 7.2 years).
Discussion
To our knowledge, the present study is the most extensive one that demonstrates the prevalence of DESH and the development of DESH in a general population. Moreover, we found that DESH was positively associated with cognitive deficit using multivariate logistic regression analyses, adjusting for relevant variables. In the follow-up surveys, we found that DESH developed independently of existing EI > 0.3, and it did not necessarily accompany the decline of cognitive function. Besides, the follow-up surveys demonstrated individuals with existing DESH showing no remarkable worsening in MMSE; in these cases, EI did not increase a lot.
As DESH is diagnosed based on an EI > 0.3, EI is the index essential for diagnosing ventricular enlargement in clinical sites. However, the mean EI is considered variable depending on the studied population, i.e., it is influenced by differences in age, gender, and related variables, while it is still controversial15. The proportion of the participants with EI > 0.3 (6.5%) in the present study was similar to that in many studies (2.8%: mean age, 59 years15; 16.1%: mean age, 75 years8; 17.0%: mean age, 73.6 years16; 6.5%: 61 and 70–72 years6), and the mean EI was also reasonable since it was compatible with other population-based studies16,17,18, excluding one study (mean EI, 0.248 ± 0.022: mean age, 70.6 years)1. Following these results and ours, it is appropriate to consider that EI increases with age and is greater in men than in women16,19. The same applies to DESH. The prevalence of DESH, limited to 75 years and over, in the present study (2.2%; 2 in 89 participants) was consistent with that in other studies (1.5–2.0% at 61–79 years)6,7,8. The present study demonstrated an age-dependent increase in the prevalence of the “DESH-expanded” when the criterion of EI for diagnosing DESH was expanded to > 0.28. Besides, our follow-up surveys demonstrated the development of DESH. These findings strongly suggest age-dependent increases in the prevalence of DESH.
In the present study, EI was not found to be associated with cognitive deficit after sex differences and age-dependent changes being taken into consideration. On the other hand, in a recent survey on 314 residents (mean age, 70.6 ± 7.9; mean EI, 0.246 ± 0.022; EI > 0.3 was seen in six subjects, 1.9%), there was a significant inverse relationship between EI and cognitive function in multivariate linear regression analyses1. The difference between these two studies is unclear, but the difference in the mean EI mentioned above might have influenced the results. In contrast, while DESH is diagnosed based on an EI > 0.3, the presence of DESH was independently associated with cognitive deficit in the present study. The difference in the association to cognitive deficit between EI and DESH may be explained by the assumption that DESH contains more specific pathological information than EI. In the present study we didn’t evaluate other indexes like z-Evans index, which is defined as the maximum z-axial length of the frontal horns of the lateral ventricles to the maximum cranial z- axial length and is thought to have a high affinity to DESH21,22, such indexes may positively associate with cognitive deficit.
As shown in Table 4 and DESH-expanded cases, “disproportionate enlargement of the inferior subarachnoid spaces with tight high-convexity subarachnoid spaces” developed before/after EI exceeded 0.3. DESH is thought to be induced by perivascular space narrowing, particularly at the centrum semiovale8, which is considered to be associated with cerebral amyloid angiopathy in cortical and leptomeningeal arteries20. These pathological changes should occur independently of an EI > 0.3; therefore, it may be reasonable to consider that the development of “disproportionate enlargement of the inferior subarachnoid spaces with tight high-convexity subarachnoid spaces” was observed before/after EI exceeded 0.3. In other words, whether EI exceeds 0.3 or not may depend on the complex of various cerebrospinal fluid hydration pathway obstructions, including perivascular space narrowing.
It is also unclear whether asymptomatic DESH is a risk for cognitive deficit or not. Iseki et al. have reported that 8 out of 12 individuals with DESH were asymptomatic, and 2 of them developed dementia and/or gait disturbance with worsening of ventriculomegaly during the follow-up period of 4–8 years6. In contrast, while we could follow up only two of the nine participants with DESH, neither of them showed a remarkable change in MMSE; at the same time, EI did not increase a lot. These findings may suggest that ventricular enlargement, in combination with the emergence of DESH, plays an essential role in the deterioration of cognitive function.
The present study has some limitations. First, the number of participants with DESH might be too small to conduct multivariate logistic regression analyses after adjustment for some relevant variables. Second, the present study did not assess gait disturbance, which is also one of the most critical symptoms of iNPH. Finally, the DESH was qualitatively identified following its characteristic pattern; therefore, the kappa coefficient of the inter-observer reliability in the present study may be insufficient for the diagnosis of DESH for clear identification, and the development of universal grading systems, like the Fazekas scale23, may be needed.
Conclusion
The present study is the most extensive one on the prevalence of DESH and the development of DESH, involving the observation of 1384 participants in a general population and demonstrating that the presence of DESH was associated with cognitive deficit using multivariate analyses. In contrast, the follow-up study showed that the development of DESH did not always accompany cognitive deficit and that DESH without a remarkable increase in EI did not cause the deterioration of cognitive function. These findings may suggest that DESH develops independently of an EI > 0.3 and the emergence of ventricular enlargement in combination with disproportionately enlarged subarachnoid space plays an essential role in the worsening of cognitive function in DESH.
References
Del Brutto, O. H. et al. Inverse relationship between the evans index and cognitive performance in non-disabled, stroke-free, community-dwelling older adults. A population-based study. Clin. Neurol. Neurosurg. 169, 139–143. https://doi.org/10.1016/j.clineuro.2018.03.021 (2018).
Evans, W. An encephalographic ratio for estimating ventricular enlargement and cerebral atrophy. Arch Neurol. Psychiatry 47, 931–937 (1942).
Marmarou, A., Bergsneider, M., Relkin, N., Klinge, P. & Black, P. M. Development of guidelines for idiopathic normal-pressure hydrocephalus: introduction. Neurosurgery 57, S1-3 (2005).
Nishida, N. et al. Association of lipocalin-type prostaglandin D synthase with disproportionately enlarged subarachnoid-space in idiopathic normal pressure hydrocephalus. Fluids Barriers CNS 11, 9. https://doi.org/10.1186/2045-8118-11-9 (2014).
Hashimoto, M., Ishikawa, M., Mori, E., Kuwana, N. & Study of, I. Diagnosis of idiopathic normal pressure hydrocephalus is supported by MRI-based scheme: a prospective cohort study. Cerebrospinal Fluid Res. 7, 18. https://doi.org/10.1186/1743-8454-7-18 (2010).
Iseki, C. et al. Asymptomatic ventriculomegaly with features of idiopathic normal pressure hydrocephalus on MRI (AVIM) in the elderly: A prospective study in a Japanese population. J. Neurol. Sci. 277, 54–57. https://doi.org/10.1016/j.jns.2008.10.004 (2009).
Jaraj, D. et al. Prevalence of idiopathic normal-pressure hydrocephalus. Neurology 82, 1449–1454. https://doi.org/10.1212/WNL.0000000000000342 (2014).
Akiguchi, I. et al. Disproportionate subarachnoid space hydrocephalus-outcome and perivascular space. Ann. Clin. Transl. Neurol. 1, 562–569. https://doi.org/10.1002/acn3.87 (2014).
Yamada, S., Ishikawa, M. & Yamamoto, K. Comparison of CSF distribution between idiopathic normal pressure hydrocephalus and Alzheimer disease. AJNR Am. J. Neuroradiol. 37, 1249–1255. https://doi.org/10.3174/ajnr.A4695 (2016).
Imai, Y. et al. Ambulatory blood pressure of adults in Ohasama, Japan. Hypertension 22, 900–912 (1993).
Ohkubo, T. et al. Prediction of stroke by ambulatory blood pressure monitoring versus screening blood pressure measurements in a general population: The Ohasama study. J. Hypertens. 18, 847–854 (2000).
Elnimr, E. M. et al. Association between white matter hyperintensity and lacunar infarction on MRI and subitem scores of the Japanese version of mini-mental state examination for testing cognitive decline: the Ohasama study. Clin. Exp. Hypertens. 34, 541–547. https://doi.org/10.3109/10641963.2012.681723 (2012).
Braekhus, A., Laake, K. & Engedal, K. A low, “normal” score on the mini-mental state examination predicts development of dementia after three years. J. Am. Geriatr. Soc. 43, 656–661 (1995).
Aono, Y. et al. Plasma fibrinogen, ambulatory blood pressure, and silent cerebrovascular lesions: The Ohasama study. Arterioscler. Thromb. Vasc. Biol. 27, 963–968. https://doi.org/10.1161/01.ATV.0000258947.17570.38 (2007).
Inatomi, Y., Yonehara, T., Hashimoto, Y., Hirano, T. & Uchino, M. Correlation between ventricular enlargement and white matter changes. J. Neurol. Sci. 269, 12–17. https://doi.org/10.1016/j.jns.2007.12.007 (2008).
Missori, P. et al. In normal aging ventricular system never attains pathological values of Evans’ index. Oncotarget 7, 11860–11863. https://doi.org/10.18632/oncotarget.7644 (2016).
Hamidu, A. U. et al. Computerized tomographic study of normal Evans index in adult Nigerians. J. Neurosci. Rural Pract. 6, 55–58. https://doi.org/10.4103/0976-3147.143195 (2015).
Jaraj, D. et al. Estimated ventricle size using Evans index: Reference values from a population-based sample. Eur. J. Neurol. 24, 468–474. https://doi.org/10.1111/ene.13226 (2017).
Brix, M. K. et al. The Evans’ Index revisited: New cut-off levels for use in radiological assessment of ventricular enlargement in the elderly. Eur. J. Radiol. 95, 28–32. https://doi.org/10.1016/j.ejrad.2017.07.013 (2017).
Roher, A. E. et al. Cortical and leptomeningeal cerebrovascular amyloid and white matter pathology in Alzheimer’s disease. Mol. Med. 9, 112–122 (2003).
Yamada, S., Ishikawa, M. & Yamamoto, K. Optimal diagnostic indices for idiopathic normal pressure hydrocephalus based on the 3D quantitative volumetric analysis for the cerebral ventricle and subarachnoid space. AJNR Am. J. Neuroradiol. 36, 2262–2269. https://doi.org/10.3174/ajnr.A4440 (2015).
Yamada, S., Ishikawa, M., Yamaguchi, M. & Yamamoto, K. Longitudinal morphological changes during recovery from brain deformation due to idiopathic normal pressure hydrocephalus after ventriculoperitoneal shunt surgery. Sci. Rep. 9, 17318. https://doi.org/10.1038/s41598-019-53888-7 (2019).
Fazekas, F., Chawluk, J. B., Alavi, A., Hurtig, H. I. & Zimmerman, R. A. MR signal abnormalities at 1.5 T in Alzheimer’s dementia and normal aging. AJR Am. J. Roentgenol. 149, 351–356. https://doi.org/10.2214/ajr.149.2.351 (1987).
Funding
This study was supported by Grants for Scientific Research, Ministry of Education, Culture, Sports, Science and Technology, Japan (17H04126, 17K15853, 17K19930, 18K09674, 18K09904, 18K17396, 19K19466, 19H03908, 19K10662); Grant-in-Aid for Young Scientists of Showa Pharmaceutical University H28-4; the Japan Arteriosclerosis Prevention Fund; Grant-in-aid from the Ministry of Health, Labor, and Welfare, Japan. (H29-Junkankitou-Ippan-003 and 20FA1002); A Scheme to Revitalize Agriculture and Fisheries in Disaster Area through Deploying Highly Advanced Technology (NouEi 2-02) from the Ministry of Agriculture, Forestry and Fisheries, Japan; The Academic Contributions from Pfizer Japan Inc.; Scholarship donations from Chugai Pharmaceutical Co., Ltd., Daiichi Sankyo Co.,Ltd.; Research Support from Astellas Pharma Inc. and Takeda Pharmaceutical Co.,Ltd.; The Health Care Science Institute Research Grant. Health Science Center Research Grant.
Author information
Authors and Affiliations
Contributions
T.N. wrote the first draft of this manuscript. M.S., A.H., M.H., A.H., H.M., K.A., M.K., K.N., A.H., Y.I., and T.O. conducted the Ohasama study. T.N., I.A, and N.M. conducted the analyses on MRI findings for this study. All authors commented to the draft and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Nishikawa, T., Akiguchi, I., Satoh, M. et al. The association of disproportionately enlarged subarachnoid space hydrocephalus with cognitive deficit in a general population: the Ohasama study. Sci Rep 11, 17061 (2021). https://doi.org/10.1038/s41598-021-95961-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-021-95961-0
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
