
Abstract
Obstructive sleep apnea syndrome (OSAS) is underdiagnosed in females and gender differences in clinical and polysomnographic findings have not been widely investigated in China. We examined clinical and polysomnographic differences between males and females with OSAS in order to determine the influence of gender on clinical presentation and polysomnographic features. Data were collected from 303 adult patients diagnosed with OSAS (237 males and 66 females) from 2017 to 2019. All the patients completed physical examination, Epworth sleepiness scale, and whole night polysomnography. AVONA, univariate and multivariate logistic regression analyses were conducted to assess gender differences of clinical and polysomnographic findings with OSAS. P < 0.05 was statistically significant. The average age was 48.4 ± 12.6 years for females and 43.4 ± 12.4 years for males. Compared with female patients with OSAS, male patients were taller and heavier, had higher systolic blood pressure in the morning, shorter duration of slow wave sleep, more micro-arousal events, greater AHI, and more complex sleep apnea events. There are obvious gender differences of clinical and polysomnographic characteristics with OSAS. Understanding gender differences will contribute to better clinical recognition of OSAS in females as well as the provision of proper health care and therapeutic practice.
Similar content being viewed by others

Introduction
Obstructive sleep apnea syndrome (OSAS) is a common sleep disorder characterized by repetitive episodes of partial or complete upper airway obstruction, resulting in sleep fragmentation and cardiovascular comorbidity1. OSAS was thought to be very rare in females and a great number of epidemiological studies of OSAS included only males2,3. According to studies in the past, the male to female prevalence ratio of OSAS varied from 2:1–4:1 in the community to 8:1 or greater in the clinics4,5,6. It has been estimated that females with OSAS was under-diagnosed to a large extent7.
Inadequate understanding of sex difference in OSAS might be the root of the gender bias observed in OSAS. The National Sleep Disorders Research Plan8 acknowledged that there was a lack of inclusion of women in the past studies and has given priority to the exploration of gender differences in sleep disorders. Understanding gender differences in OSAS has currently been an important issue.
Gender differences in clinical and polysomnographic (PSG) findings have not been widely investigated outside North America9, and Chinese patients with OSAS may have different clinical features from North American patients. Therefore, the present study was undertaken to examine the gender differences in clinical and PSG findings in a subset of Chinese adult patients with OSAS and compare the findings with data from the literature.
Results
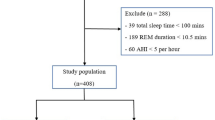
A total of 303 adult patients who were diagnosed with OSAS based on PSG were the focus of the study. The male to female ratio was 3.59:1 with respect to 237 males and 66 females. The mean age was 43.4 ± 12.4 years for males and 48.4 ± 12.6 years for females. 24.2% of females and 7.5% of males were older than 60 years (Table 1).
Regarding body mass index (BMI) distribution, in the normal weight group, females were proportionally more (57.6 vs 40.9%), whereas in the overweight group, males were proportionally more (45.9 vs 28.7%). The proportion of obese patients was similar in male and female groups (11.4% vs 10.7%) (Table 2).
According to univariate and multivariate logistic regression analyses (Tables 3 and 4), compared with female patients with OSAS, male patients were taller (157.5 ± 5.0 cm, versus 169.8 ± 6.0 cm, respectively) and heavier (61.1 ± 9.6 kg versus 74.9 ± 11.5 kg, respectively). Male patients had higher systolic blood pressure in the morning (119.4 ± 13.6 mmHg versus 124.3 ± 16.1 mmHg, respectively), shorter duration of slow wave sleep (SWS) (52.7 ± 41.5 min versus 37.8 ± 27.3 min, respectively), more micro-arousal events (100.1 ± 77.0 versus 161.2 ± 125.5, respectively), more complex apnea events (2.7 ± 6.2 versus 18.2 ± 46.3, respectively). Apnea–hypopnea index (AHI) during total sleep time (TST) was greater in males than in females (24.3 ± 19.4 min versus 33.9 ± 25.5 min, respectively).
TST was similar in male and female patients (455.1 ± 68.7 min versus 451.7 ± 69.8 min, respectively). There were no gender differences in REM sleep stage, N1 and N2 sleep duration (67.4 ± 30.8 min versus 71.9 ± 28.3 min, respectively, 331.5 ± 67.8 min versus 359.8 ± 240.6 min, respectively). Sleep latency of N1 and N2 was similar in females and males (14.1 ± 15.4 min versus 9.4 ± 17.3 min, 23.9 ± 29.9 min versus 16.7 ± 24.1 min, respectively). There was no significant gender difference of sleep efficiency (85.6 ± 10.5% versus 86.3 ± 12.1%, respectively). Mean and minimum oxygen desaturation were similar between genders (95.6 ± 1.7% versus 95.9 ± 2.0%, 78.7 ± 14.1% versus 82.6 ± 8.8%).
Discussion
The male to female ratio in our study was 3.59:1, which was consistent with previous studies4,5,6. According to previous literature, most of the female patients with OSAS were in menopause and older than male patients. Raluca et al pointed out that hormones especially progesterone might protect premenopausal women from developing OSAS and testosterone may be a risk factor of OSAS10.
Our study found that male patients were taller and heavier than female patients. According to the report on Nutrition and Chronic Disease Status of Chinese Residents (2015), the average height for males and females aged over 18 years old were 167.1cm and 155.8cm respectively, which was similar to our findings. Literature about the gender differences in BMI among OSAS patients were mixed. Most of the studies reported that females had higher BMI than males11,12 whereas other studies including our study showed that BMI could not play a role in the gender differences of OSAS patients13.
Our study showed that daytime sleepiness and snoring symptoms were similar between male and female patients with OSAS, and males showed more witnessed apneas. Andressa Silva et al.14 found that snoring and sleepiness were similarly common in females and males, but females went to see a doctor more often with a chief complaint of insomnia, which may partly explain the phenomenon of lower diagnostic rate of OSAS in females.
Our study showed that female patients had longer duration of SWS. Fewer studies have investigated gender differences in the SWS, and the data are more conflicting. Few studies indicated that there were no gender differences in the amount of SWS15, whereas other studies reported that males may have sustained reductions in SWS as compared with females over the lifespan16,17,18. It is well known that AHI is significantly decreased during SWS 19 and there is an attempt to explain it by higher upper-airway muscle activity and/or lower upper-airway collapsibility during SWS20,21.
Our study found that males have more severe OSAS than females, which was consistent with most of the previous studies6,12,22,23,24. The pathophysiologic mechanisms have not been well clarified. Differences in the dynamic properties of the upper airway may play a critical role. Elisa Perger et al.25 suggested that upper airways were stiffer in females than in males, so that females were less susceptible to collapse and males had greater pharyngeal collapsibility. In addition, female hormones may increase the upper airway dilator muscles tone, which helped to prevent airway collapse26.
Our study found that systolic blood pressure in the morning was significantly higher in males than in females. The micro-arousal events were also greater in males. Recently emerging evidence suggests that there is a causal link between OSAS and hypertension, and hypertension represents an independent risk factor of OSAS. In addition, the existence of micro-arousals is enough to cause an hypertension peak which might partly explain the results27.
Limitations of the study need to be pointed out. The patients enrolled in the study were from only one sleep disorder center, which might result in potential sampling bias. Larger, multi-center studies are required to explore the impact of gender on OSAS. A better understanding of gender differences of OSAS will be useful in better recognition, intervention and treatment of the syndrome in females.
Methods
Participants
A total of 303 adult patients with OSAS were referred to the sleep disorder center of department of psychosomatics, Sichuan Academy of Medical Sciences & Sichuan Provincial People's Hospital from 2017 to 2019. All patients completed physical examination, Epworth Sleepiness Scale (ESS) and PSG.
The study was reviewed and approved by the Ethics Committee of Sichuan Academy of Medical Sciences & Sichuan Provincial People's Hospital, and conducted in accordance with the Declaration of Helsinki.
Questionnaire
The most important scale for the assessment of daytime sleepiness is ESS published in 1991 by Murray Johns28. It consists of a self-administered questionnaire that investigates the extent of daytime sleepiness specifically and in a very simple manner. There are 8 items in ESS and subjects are asked to rate on a 4-point scale (0–3) his/her chances of dozing in each of 8 different situations that are often encountered in daily life. Arbitrarily, a score of ≧12 has been suggested as being abnormal and an indicator of excessive daytime sleepiness29.
PSG data collection
The gold standard diagnostic method for OSAS is a full-night PSG30. The frequency of episodes of apnea and/or hypopnea per hour of sleep, also known as AHI, as well as the lowest observed oxyhemoglobin saturation during sleep is used as the main criteria for severity assessment.
All patients had to have a minimum of 8 h of monitored sleep in the sleep disorder center. They underwent nocturnal PSG monitoring (Philips Alice Version 6, Netherland) using 6 scalp electrodes (C3, C4, F3, F4, O1 and O2 locations), 2 reference electrodes behind the ears (left [A1] and right [A2] mastoid areas), 3 electromyographic electrodes over the submental muscles, 4 electromyographic electrodes over the leg muscles, 2 electrooculographic electrodes, one ground electrode and nasal flow detector. Pulse oximeter was used to obtain nocturnal oximetry recordings. Electrocardiogram was used to obtain rhythm of the heart. The AHI documented the number of apnea-plus-hypopnea incidents every hour during sleep31.
Statistics
Statistical analyses were performed with SPSS 26.0 for mac. The summary of descriptive statistics was presented as mean (with SD) for continuous variables and as frequencies (with percentages) for categorical variables. ANOVA was used for comparison of quantitative data. Univariate and multivariate logistic regression analyses were conducted to identify gender differences of clinical and polysomnographic findings with OSAS. Statistically significant difference was considered if P value < 0 0.0531.
Ethics approval and consent to participate
The research was approved by the Ethics Committee of Sichuan Academy of Medical Sciences & Sichuan Provincial People's Hospital. Written informed consent was obtained from all the participants.
Consent to publish
Written informed consent was obtained from all participants for the publication of any potentially identifiable images or data included in this article.
Data availability
The data used and analyzed during the current study are available from the corresponding author on reasonable request.
References
Park, J. G., Ramar, K. & Olson, E. J. Updates on definition, consequences, and management of obstructive sleep apnea. Mayo Clin. Proc. 86, 549–554; quiz 554–545, doi:https://doi.org/10.4065/mcp.2010.0810 (2011).
Fekete, K. et al. Resting energy expenditure in OSAS: the impact of a single CPAP application. Sleep Breath 20, 121–128. https://doi.org/10.1007/s11325-015-1194-y (2016).
Chen, D.-D., Huang, J.-F., Lin, Q.-C., Chen, G.-P. & Zhao, J.-M. Relationship between serum adiponectin and bone mineral density in male patients with obstructive sleep apnea syndrome. Sleep breath 21(2), 557–564 (2017).
Bozkurt, M. K. et al. Gender differences in polysomnographic findings in Turkish patients with obstructive sleep apnea syndrome. Eur. Arch. Otorhinolaryngol. 265, 821–824. https://doi.org/10.1007/s00405-007-0554-z (2008).
Senaratna, C. V. et al. Prevalence of obstructive sleep apnea in the general population: a systematic review. Sleep Med. Rev. 34, 70–81. https://doi.org/10.1016/j.smrv.2016.07.002 (2017).
Heinzer, R. et al. Prevalence of sleep-disordered breathing in the general population: the HypnoLaus study. Lancet Respir. Med. 3, 310–318. https://doi.org/10.1016/S2213-2600(15)00043-0 (2015).
Karaduman, M. et al. Evaluation of obstructive sleep apnea symptoms in pregnant women with chronic disease. J. Matern. Fetal Neonatal Med. 29, 3379–3385. https://doi.org/10.3109/14767058.2015.1127346 (2016).
Research, N. C. o. S. D. 2003 National Sleep Disorders Research Plan. Sleep 26(3), 253–257 (2003).
Tufik, S., Santos-Silva, R., Taddei, J. A. & Bittencourt, L. R. Obstructive sleep apnea syndrome in the Sao Paulo Epidemiologic Sleep Study. Sleep Med. 11, 441–446. https://doi.org/10.1016/j.sleep.2009.10.005 (2010).
Bercea, R., Bercea, B. & Mihăescu, T. Association between the serum level of testosterone and other comorbidities in obstructive sleep apnea. Pneumologia 61(2), 98–101 (2012).
Topirceanu, A., Udrescu, L., Udrescu, M. & Mihaicuta, S. Gender phenotyping of patients with obstructive sleep apnea syndrome using a network science approach. J. Clin. Med. 9, 4025. https://doi.org/10.3390/jcm9124025 (2020).
Erdemir Işık, M., Gulbay, B., Çiftci, F. & Acıcan, T. Polysomnographic, demographic and clinic differences between male and female obstructive sleep apnea patients. Tuberk Toraks 68(4), 361–370 (2020).
Vagiakis, E. et al. Gender differences on polysomnographic Wndings in Greek subjects with obstructive sleep apnea syndrome. Sleep Med. 7, 424–430 (2006).
Silva, A. et al. Gender differences in sleep patterns and sleep complaints of elite athletes. Sleep Sci. 12, 242–248. https://doi.org/10.5935/1984-0063.20190084 (2019).
Krishnan, V. & Collop, N. A. Gender differences in sleep disorders. Curr. Opin. Pulm. Med. 12, 383–389. https://doi.org/10.1097/01.mcp.0000245705.69440.6a (2006).
Mokhlesi, B., Pannain, S., Ghods, F. & Knutson, K. L. Predictors of slow-wave sleep in a clinic-based sample. J. Sleep Res. 21, 170–175. https://doi.org/10.1111/j.1365-2869.2011.00959.x (2012).
Yetton, B. D., McDevitt, E. A., Cellini, N., Shelton, C. & Mednick, S. C. Quantifying sleep architecture dynamics and individual differences using big data and Bayesian networks. PLoS ONE 13, e0194604. https://doi.org/10.1371/journal.pone.0194604 (2018).
Luca, G. et al. Age and gender variations of sleep in subjects without sleep disorders. Ann Med 47, 482–491. https://doi.org/10.3109/07853890.2015.1074271 (2015).
Koutsourelakis, I., Lamprou, K., Vagiakis, E. & Zakynthinos, S. Resolution of apnoeas in slow wave sleep. Sleep Breath 20, 819–820. https://doi.org/10.1007/s11325-015-1275-y (2016).
McSharry, D. G. et al. A mechanism for upper airway stability during slow wave sleep. Sleep 36, 555–563. https://doi.org/10.5665/sleep.2544 (2013).
Carberry, J. C., Jordan, A. S., White, D. P., Wellman, A. & Eckert, D. J. Upper airway collapsibility (pcrit) and pharyngeal dilator muscle activity are sleep stage dependent. Sleep 39, 511–521. https://doi.org/10.5665/sleep.5516 (2016).
Mieno, Y. et al. Gender differences in the clinical features of sleep apnea syndrome. Intern. Med. 57, 2157–2163. https://doi.org/10.2169/internalmedicine.7570-16 (2018).
Saldias Penafiel, F. et al. Gender differences in clinical features and performance of sleep questionnaires in adults with obstructive sleep apnea syndrome. Rev. Med. Chil. 147, 1291–1302. https://doi.org/10.4067/s0034-98872019001001291 (2019).
Basoglu, O. K. & Tasbakan, M. S. Gender differences in clinical and polysomnographic features of obstructive sleep apnea: a clinical study of 2827 patients. Sleep Breath 22, 241–249. https://doi.org/10.1007/s11325-017-1482-9 (2018).
Perger, E., Mattaliano, P. & Lombardi, C. Menopause and sleep apnea. Maturitas 124, 35–38. https://doi.org/10.1016/j.maturitas.2019.02.011 (2019).
Asavasupreechar, T., Saito, R., Edwards, D. P., Sasano, H. & Boonyaratanakornkit, V. Progesterone receptor isoform B expression in pulmonary neuroendocrine cells decreases cell proliferation. J. Steroid Biochem. Mol. Biol. 190, 212–223 (2019).
Ciccone, M. M. et al. Is there a correlation between OSAS duration/severity and carotid intima-media thickness?. Respir. Med. 106, 740–746. https://doi.org/10.1016/j.rmed.2011.12.016 (2012).
Johns, M. W. A new method for measuring daytime sleepiness: the Epworth sleepiness scale. Sleep 14, 540–545. https://doi.org/10.1093/sleep/14.6.540 (1991).
Dauvilliers, Y. et al. Long-term use of pitolisant to treat patients with narcolepsy: Harmony III Study. Sleep 42(11), zsz74 (2019).
Hug, M. et al. Screening for obstructive sleep apnea among hospital outpatients. PLoS ONE 13, e0198315 (2018).
Zhou, X. et al. Risk factors associated with the severity of obstructive sleep apnea syndrome among adults. Sci. Rep. 10, 13508. https://doi.org/10.1038/s41598-020-70286-6 (2020).
Acknowledgements
The study was financially supported by the projects (grant number: 2016LY12) from Sichuan Academy of Medical Sciences & Sichuan Provincial People's Hospital. We would like to thank Dr Fang Luo, Dr Xi Yu and Dr Yan Jiang for their help in collecting the data. We would like to thank Dr Zhe Li for her advice in improving the quality of the manuscript.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Q.L., S.P.L. and Z.Y.P. and F. L. The first draft of the manuscript was written by X.Z., B.Z. and Z.L provided valuable advice. All authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Zhou, X., Zhou, B., Li, Z. et al. Gender differences of clinical and polysomnographic findings with obstructive sleep apnea syndrome. Sci Rep 11, 5938 (2021). https://doi.org/10.1038/s41598-021-85558-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-021-85558-y
This article is cited by
-
Analysis by sex of safety and effectiveness of transvenous phrenic nerve stimulation
Sleep and Breathing (2023)
-
Clinical and polysomnographic predictors of suboptimal auto-adjusting CPAP titration in adult OSA patients: a single-center study
European Archives of Oto-Rhino-Laryngology (2023)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
