
Abstract
Staphylococcus aureus or methicillin-resistant Staphylococcus aureus (MRSA) is an important issue associated with significant morbidity and mortality and well known as a predominant pathogen causing bloodstream infection (BSIs) globally. To estimate the antibiotic resistance and molecular characteristics of S. aureus causing BSIs in Shanghai, 120 S. aureus isolates (20 isolates each year) from the patients with S. aureus BSIs from 2013 to 2018 were randomly selected and enrolled in this study. Fifty-three (44.2%) MRSA isolates were determined, and no isolate was found resistant to vancomycin, daptomycin, synercid, linezolid and ceftaroline. The toxin genes tst, sec, seg and sei were found more frequently among MRSA isolates compared with MSSA isolates (all P < 0.0001). Twenty-nine sequence types (STs) were identified, and ST5 (23.3%) was the most common ST, followed by ST398 (11.7%) and ST764 (10.0%). SCCmec II (73.6%) was the most frequent SCCmec type among MRSA isolates. The dominant clonal complexes (CCs) were CC5 (ST5, ST764, ST965 and ST3066; 36.7%) and the livestock-associated clone CC398 (ST398, 11.7%). MRSA-CC5 was the predominant CC among MRSA isolates (37/53, 69.8%), and CC5-II MRSA was found in 34 isolates accounting for 91.9% (34/37) among CC5 MRSA isolates. In addition, all 29 tst-positive MRSA isolates were CC5-MRSA as well. Our study provided the properties and genotypes of S. aureus causing BSIs at Ruijin Hospital in Shanghai from 2013 to 2018, and might suggest of value clues for the further study insights into pathogenic mechanisms intrinsically referring to the development of human-adapted S. aureus clones and their diffusions.
Similar content being viewed by others

Introduction
Bloodstream infections (BSIs) is a severe infection with high incidence and lethality all over the world, and it always prolonged hospital stay for a long period1. It has been reported to be one of the seven leading causes of death in North America and Europe2. Staphylococcus aureus is well known as one of the most important human pathogens across the world and is capable of causing a variety of infections in healthcare facilities and communities. Furthermore, S. aureus is one of the major and most fatal causes of bacteremia with an estimated mortality of 20%, and at least 50% of patients with S. aureus bacteremia (SAB) will develop complicated bacteremia3.
S. aureus is one of the most common causes of severe BSIs with high morbidity and mortality. Early mortality associated with SAB appears to have plateaued at approximately 20–30%4, and imposes a substantial burden on patients and healthcare systems. In the United States, the annual incidence of SAB is 4.3 to 38.2 per 100,000 person-years, and the 30-day all-cause mortality of SAB is 20% and has not changed since the 1990s5. In Ireland, S. aureus accounted for approximately 19–32% annually among BSIs and has been the second most common cause of BSIs consistently, ranking only second to Escherichia coli between 2006 and 2016 as reported6. Besides, S. aureus is also the second-most frequent pathogen found in neonatal bacteremia in the UK, resulting in significant neonatal morbidity and mortality that approximately 20–35%7.In China from 2012 to 2016, S. aureus accounted for 25.9% among BSIs in Jiangxi province, which is located in Southeastern China8. The European Antimicrobial Resistance Surveillance System including 27 countries revealed an increased burden of S. aureus BSIs by 2.3% per year in the 2000s and rising levels of S. aureus BSIs due to methicillin-susceptible S. aureus (MSSA)9. In Alberta, Canada, there were 299 cases of methicillin-resistant S. aureus (MRSA) BSIs in total from 2011 to 2013, equating to 3.95 cases per 100,000 population as reported10. The epidemiology of S. aureus among BSIs appears to be changing, and several surveillances worldwide reveal an increasing incidence of BSIs with S. aureus11.
S. aureus features among for its versatility in adaptability, ability to capture various resistance, virulence genes and genetic diversity. Thus, our study aimed to investigate the antimicrobial resistance and molecular characteristics of S. aureus causing BSIs in Shanghai, China from 2013 to 2018.
Materials and Methods
Study design and bacterial isolates
This study was performed at Ruijin Hospital, Shanghai Jiao Tong University School of Medicine, a tertiary teaching hospital with more than 3,000 beds serving patients from all over China. Because of the transferring of laboratory information system at Ruijin Hospital in 2015, the detail information of BSIs from January 2013 to July 2015 were missing. From August 2015 to December 2018, a total of 2760 patients with BSIs were determined at Ruijin Hospital, and 204 (7.4%) of them were caused by S. aureus.
All patients with BSIs in this study were determined by blood culture. Only the first positive blood cultures were reviewed and recorded. The initial species identification was performed using MALDI-TOF MS (bioMérieux, Marcy-l’Étoile, France). From January 2013 to December 2018, 243 S. aureus isolated from the patients with SAB were collected. One hundred and twenty S. aureus isolates were randomly selected (20 isolates each year) and enrolled in this study using the random number generation function in Microsoft Office Excel 2016 (Microsoft Corporation, Redmond, WA, USA). This study was approved by Ethics Committee of Ruijin Hospital affiliated to Shanghai Jiao Tong University School of Medicine (2019 LinLunShen No.146), and the Review Committee removed the need for informed consent for this retrospective study which focused on bacteria and did not involve patient interventions.
Antimicrobial susceptibility testing
Antimicrobial susceptibility testing was performed manually according to the guidelines of Clinical and Laboratory Standards Institute issued in 2018 (CLSI 2018)12. Antibiotics tested were as following using broth microdilution method: penicillin(0.03,0.12–0.25,2,8 μg/ml), cefoxitin screen(4 μg/ml), oxacillin(0.25,1–2 μg/ml), erythromycin(0.5–4 μg/ml), clindamycin(0.25–0.5,2 μg/ml), azithromycin(2–4 μg/ml), gentamicin(4–8 μg/ml), levofloxacin(1–4 μg/ml), moxifloxacin(0.5–1,4 μg/ml), ciprofloxacin(1–2 μg/ml), cefazolin(8–16 μg/ml), rifampin(1–2 μg/ml), ampicillin(2–8 μg/ml), ampicillin/sulbactam(8/4–16/8 μg/ml), amoxicillin/K Clavulanate(4/2 μg/ml), tetracycline(4–8 μg/ml), chloramphenicol(8–16 μg/ml), trimethoprim/sulfamethoxazole(0.5/9.5–2/38 μg/ml), vancomycin(0.5–16 μg/ml), daptomycin(1,4 μg/ml), synercid(0.5–2 μg/ml), linezolid(2–4 μg/ml), ceftaroline(0.5–2 μg/ml). The antibiotics selected and their ranges were referred to MicroScan Pos Combo Panel Type 44 (Beckman Coulter, Inc. USA). S. aureus ATCC29213 strain was used as the quality control for the antimicrobial susceptibility testing.
Toxin genes detection
A total of 13 significant toxin genes clinically including lukS/F-PV, tst, eta, etb, sea-see and seg-sej were detected on all 120 S. aureus isolates in this study by polymerase chain reaction (PCR) as described previously13. lukS/F-PV encodes Panton-Valentine leukocidin; tst encodes toxic shock syndrome toxin 1; eta and etb encodes exfoliative toxin A and B; sea-see and seg-sej encodes staphylococcal enterotoxins SEA-SEE and SEG-SEJ.
Molecular typing
Multilocus sequence typing (MLST), spa typing and agr typing were performed on all 120 S. aureus isolates according to the guidelines on the websites (https://pubmlst.org/, http://spa.ridom.de/index.shtml) and other published documents and researches13,14. mecA detection was performed on all 120 S. aureus isolates as well to confirm the existence of MRSA. SCCmec types of MRSA were determined by the previous method as described15. The gene blaZ, which produces beta-lactamase and inactivates penicillin by hydrolyzing the beta-lactam ring, was detected on all 120 S. aureus isolates16.
Statistical analysis
The chi-square or Fisher’s exact test was used for statistical analysis as appropriate, and a two-sided P value of <0.05 was considered for statistical significance. All statistical analysis in this study was conducted by the software package SAS 8.2 (SAS Institute Inc., Cary, NC, USA).
Results
Clinical data
From January 2013 to December 2018, the median age of patients with SAB in this study was 59 years (range: 7 months-97 years; interquartile range: 44–69 years), and the sex distribution (male/ female) was 67.5%/32.5%. The mortality of patients with SAB was 25.8%, while 15 (12.5%) patients were transferred with unknown outcomes.
The incidence of S. aureus accounting for BSIs was 7.4% at Ruijin Hospital in Shanghai from August 2015 to December 2018, for the system transferring in 2015 and data missing as described in materials and methods.
Antimicrobial resistance
Fifty-three (44.2%) S. aureus isolates were confirmed as MRSA in this study, and all 53 MRSA isolates were mecA-positive. We did not discover any isolate resistant to vancomycin, daptomycin, synercid, linezolid and ceftaroline. No isolate was found showing a reduced vancomycin susceptibility or intermediate to vancomycin among the 120 S. aureus isolates in this study (supplementary information). The resistance rates of antibiotics tested for overall 120 S. aureus isolates from 2013 to 2018 were presented in Table 1. All 53 MRSA isolates detected in the study were resistant to penicillin, and 51 (51/67, 76.1%) MSSA isolates were resistant to penicillin. Sixty-eight (56.7%) S. aureus isolates including 17 MRSA and 51 MSSA isolates were detected blaZ-positive, and all 51 MSSA isolates resistant to penicillin were blaZ-positive as well. Forty-six (46/53, 86.8%) MRSA isolates were observed showing multi-drug resistance in this study.
Virulence factors
The toxin genes etb and see were not discovered among all S. aureus isolates in this study. The seg was found most frequently among the toxin genes screened, occurring in 60 isolates (50.0%) as presented in Table 2. The tst, sec, seg and sei were found more frequently among MRSA isolates compared with MSSA isolates (all P < 0.0001). However, sed was observed more frequently among MSSA isolates (P = 0.0254), and sed was detected only among eight MSSA isolates as shown in Table 2. Besides, sej was found only among four MSSA isolates, but there was no significant difference statistically between MSSA and MRSA isolates (P = 0.1946).
Molecular types
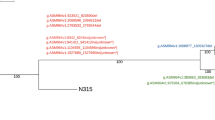
Twenty-nine sequence types (STs) were identified among all 120 S. aureus isolates as presented in Table 3. ST5 (28/120, 23.3%) was the most common ST, followed by ST398 (14/120, 11.7%) and ST764 (12/120, 10.0%); and t002 (12/120, 10.0%) was the most common spa type followed by t2460 (10/120, 8.3%) and t034 (7/120, 5.8%). One ST2959 MSSA isolate could not be spa typed (negative for certain PCR). Among 53 MRSA isolates, SCCmec II (39/53, 73.6%) was the most frequent SCCmec type as presented in Table 4, followed by SCCmec V (8/53, 15.1%), SCCmec IV (4/53, 7.5%) and SCCmec I (2/53, 3.8%). As shown in Fig. 1, produced by eBURST based on the ST data in this study, CC5 (ST5, ST764, ST965 and ST3066; 44/120, 36.7%) was the most common clonal complex (CC), followed by the livestock-associated (LA) clone CC398 (ST398, 14/120, 11.7%). Furthermore, MRSA-CC5 has been the dominant CC among MRSA isolates in this study and the percentage was as high as 69.8% (37/53), and all tst-positive MRSA isolates (n = 29) were CC5-MRSA as well. The agrI (66/120, 55%) was the most frequent agr group, followed by agrII (50/120, 41.7%), agrIII (2/120, 1.7%), and agrIV (2/120, 1.7%).

The diagram produced by eBURST with the stringent (default) group definition. Each number represents an MLST ST and the area of each circle indicates the prevalence of the ST in the MLST data of this study. MLST, multilocus sequence typing; ST, sequence type.
In 2013, the most common ST was ST5 (20.0%), followed by ST1801 (15.0%), ST7 (15.0%), ST764 (15.0%) and ST398 (10.0%); in 2014, the most common ST was ST5 (30.0%), followed by ST188 (15.0%), ST7 (15.0%) and ST764 (10.0%); in 2015, the most common ST was ST764 (25.0%), followed by ST1821 (15.0%), ST398 (10.0%), ST5 (10.0%) and ST199 (10.0%); in 2016, the most common ST was ST5 (40.0%), followed by ST398 (15.0%), ST59 (10.0%) and ST1921 (10.0%); in 2017, the most common ST was ST5 (20.0%), followed by ST1921 (10.0%); in 2018, the most common ST was ST398 (25.0%), followed by ST5 (20.0%). To sum up, ST5 (or CC5) has been highly prevalent among S. aureus isolates causing BSIs from 2013 to 2018 in Shanghai.
Eighty-one (67.5%) patients developed SAB 48 hours or more after admission to hospital that were considered as healthcare-associated (HA) infections, and 43 (53.1%) patients were infected with MRSA. ST5 (24/81, 29.6%) was the most common ST among HA-S. aureus isolates, and CC5 (36/81, 44.4%) was the most common CC as well. In addition, CC5-II MRSA (28/43, 65.1%) was the most frequent clone among HA-MRSA isolates.
Discussion
S. aureus or MRSA is an important pathogen and frequent cause of invasive infections as well as bloodstream infections around the world. In this study, SAB accounted for 7.4% of BSIs cases in Shanghai from 2013 to 2018, much lower than that in a regional burn center in Jiangxi province in China, which is 25.9% from 2012 to 20168. Coincidentally, in the United States, the incidence of MRSA BSIs in hospitals and communities dropped off 74% and 40% respectively from 2005 to 201617. According to the latest data provided by the European Antimicrobial Resistance Surveillance Network (EARSNet) (2013–2016), more than a third of countries with low and high MRSA prevalence have reported significantly decreasing trends among bloodstream infections, and the population-weighted average MRSA BSIs percentage has dropped from 18.1% in 2013 to 13.7% in 201618. The exact reasons for this specific decline among MRSA BSIs are not fully understood. However, in despite of these positive developments, S. aureus or MRSA still remains a priority for public health in Europe, with 10 of 30 countries reporting prevalence rates of MRSA > 25%, including Greece19.
The mortality rate of S. aureus BSIs in Shanghai was 25.8% from 2013 to 2018 in this study, similar to that reported in other published researches of adult patient with S. aureus BSIs (around 20–30%) in other countries3,5,20. However, it was much higher than that among infants with S. aureus BSIs both in Europe and USA which have shown overall mortality of 6.4–16%7,21,22. The prevalence of methicillin resistance among S. aureus isolates in Hong Kong has risen to >50% while the mortality rates of MRSA bloodstream infections are close to one-third as reported23. The proportion of MRSA among S. aureus BSIs in Shanghai was 44.2% in this study. Nevertheless, methicillin resistance is always significantly associated with higher mortality as well as comorbid conditions, intensive care unit admission, and prior exposure to antibiotics24. In addition, chronic lung disease, previous hospitalization and older patients (>79 years) are related with increased mortality as well23. The mortality in MSSA infections significantly declined and the average time to anti-staphylococcal therapy in MSSA infections decreased even though the mortality in MRSA infections was unchanged25. The declining mortality in MSSA infections might be related to the reduction in the duration of targeted therapy. These results emphasize the potential for rapid diagnostics and early optimization of treatment to impact outcomes in MSSA bacteremia. Nevertheless, it was revealed that the treatment failure rate of complicated MRSA bloodstream infections was as high as 40%26. MRSA might still need more attention when the patient was determined with MRSA bloodstream infections.
CC5 (S. aureus: 44/120, 36.7%; MRSA: 37/53, 69.8%) was the dominant clone among patients with SAB at Ruijin Hospital in Shanghai from 2013 to 2018 in this study, slightly different from our previous research conducted in Shanghai from 2009 to 2011 that CC8 (ST239) might be more common among patient with SAB before27. However, shifts may be occurring in the molecular epidemiology of S. aureus and MRSA among patients with bloodstream infections. As reported from a single-center surveillance in Greece, the widespread HA-MRSA clone ST239-III gradually decreased with the increase of the isolation frequency of these two CCs: HA-MRSA CC5, mostly belonging to ST5-II; and community-associated MRSA (CA-MRSA) CC80, mainly represented by ST80-IV-t04419. In this study, CC5- II MRSA was found in 34 isolates accounting for 91.9% (34/37) among CC5 MRSA isolates, suggesting that CC5 MRSA or CC5-II MRSA might be more frequent occurring among patients with MRSA BSIs in Shanghai. It has been suggested that CC5 has become an increasingly frequent cause of MRSA infections as well as bacteremia acquired by hospitalized patients from some other reports and that healthcare exposure is no longer a discriminator of USA100 vs USA300 infections28,29,30. An analysis of SAB conducted in Spain over 15 years (2002–2017) revealed that CC5 was the most prevalent CC and the proportion of CC5 among healthcare-associated S. aureus isolates was higher than that among community-associated S. aureus isolates, and CC5 was much more associated with methicillin resistance4. Simultaneously, CC5 MRSA was also prevalent in bloodstream infections in nine Latin American countries except in Colombia and Ecuador29. Clonal substitution appears to be a common phenomenon, and continuous surveillance is essential to identify molecular epidemiological changes in S. aureus and MRSA.
The livestock-associated clone CC398 was observed secondly frequent in this study. In our previous study, CC398 was the most common clone among patients with skin and soft tissue infections (SSTIs) especially where the livestock husbandry well developed in China31. In recent years in Denmark, the percentage of LA-MRSA CC398 among BSIs and SSTIs has been increasing and reached its peak in 2014, accounting for 16% and 21% in MRSA BSIs and SSTIs respectively32. The vast majority of patients with LA-MRSA CC398 BSIs had no history of exposure to livestock, which is similar to the ratio observed for other types of MRSA, and it demonstrates that the increase of LA-MRSA CC398 BSIs was accompanied by a large increase of LA-MRSA CC398 SSTIs and the expansion of porcine reservoir32. CC398 S. aureus resulted in an increasing incidence of bloodstream infections in a French hospital between 2010 and 2017 as well; the prevalence rate of CC398 isolates among S. aureus BSIs increased from 3.6% in 2010 to 20.2%in 2017 (P < 0.05)33. CC398 MRSA emerged but remains very sparse and CC398 MSSA disseminates in the community as suggested. In this study in Shanghai, 4 CC398 MRSA and 10 CC398 MSSA isolates were discovered. More recently, CC398 MSSA have been increasingly being reported as the cause of invasive infections among patients who have no contact with livestock, and CC398 MSSA bloodstream infections were always associated with high mortality34. It has been hypothesized that lysogeny may play an important role in increasing the ability of ST398 clone to cause human infections, and the significant risk calling for urgent attention is that ST398 clone family will still increase its threat to public health by continuing to obtain virulence and/or multidrug resistance genes from healthcare-associated S. aureus clones35. Therefore, it is deeply needed to monitor the extraordinary cloning of human adaptive S. aureus like CC398 and genomic studies might can figure out the determinants of its diffusion.
References
Laupland, K. B. Incidence of bloodstream infection: a review of population-based studies. Clinical microbiology and infection: the official publication of the European Society of Clinical Microbiology and Infectious Diseases 19, 492–500, https://doi.org/10.1111/1469-0691.12144 (2013).
Goto, M. & Al-Hasan, M. N. Overall burden of bloodstream infection and nosocomial bloodstream infection in North America and Europe. Clinical microbiology and infection: the official publication of the European Society of Clinical Microbiology and Infectious Diseases 19, 501–509, https://doi.org/10.1111/1469-0691.12195 (2013).
Guimaraes, A. O. et al. A Prognostic Model of Persistent Bacteremia and Mortality in Complicated Staphylococcus aureus Bloodstream Infection. Clin. Infect. Dis. 68, 1502–1511, https://doi.org/10.1093/cid/ciy739 (2019).
Perez-Montarelo, D. et al. Molecular Epidemiology of Staphylococcus aureus Bacteremia: Association of Molecular Factors With the Source of Infection. Frontiers in microbiology 9, 2210, https://doi.org/10.3389/fmicb.2018.02210 (2018).
Thomer, L., Schneewind, O. & Missiakas, D. Pathogenesis of Staphylococcus aureus Bloodstream Infections. Annual review of pathology 11, 343–364, https://doi.org/10.1146/annurev-pathol-012615-044351 (2016).
Deasy, E. C. et al. A molecular epidemiological investigation of methicillin-susceptible Staphylococcus aureus causing bloodstream infections in Ireland, 2006–2017. Eur. J. Clin. Microbiol. Infect. Dis. 38, 927–936, https://doi.org/10.1007/s10096-019-03523-0 (2019).
O’Reilly, D., O’Connor, C., McCallion, N. & Drew, R. J. A retrospective study (2001–2017) of acute and chronic morbidity and mortality associated with Staphylococcus aureus bacteraemia in a tertiary neonatal intensive care unit. Irish journal of medical science, https://doi.org/10.1007/s11845-019-01992-y (2019).
Liu, Y. et al. Molecular Epidemiology and Virulence Features of Staphylococcus aureus Bloodstream Isolates in a Regional Burn Center in China, 2012–2016. Microbial drug resistance (Larchmont, N.Y.) 24, 1354–1360, https://doi.org/10.1089/mdr.2017.0209 (2018).
de Kraker, M. E. et al. The changing epidemiology of bacteraemias in Europe: trends from the European Antimicrobial Resistance Surveillance System. Clinical microbiology and infection: the official publication of the European Society of Clinical Microbiology and Infectious Diseases 19, 860–868, https://doi.org/10.1111/1469-0691.12028 (2013).
Taylor, G. et al. Epidemiology of meticillin-resistant Staphylococcus aureus bloodstream infections in Alberta, Canada. J. Hosp. Infect. 89, 132–135, https://doi.org/10.1016/j.jhin.2014.11.008 (2015).
Sauget, M. et al. Increasing incidence of bloodstream infections due to Staphylococcus aureus clonal complex 398 in a French hospital between 2010 and 2017. European Journal of Clinical Microbiology & Infectious Diseases, https://doi.org/10.1007/s10096-019-03653-5 (2019).
Institute, C. A. L. S. Performance Standards for Antimicrobial Susceptibility Testing. CLSI document M100-S28, Wayne, PA, USA 38 (2018).
Jarraud, S. et al. Relationships between Staphylococcus aureus genetic background, virulence factors, agr groups (alleles), and human disease. Infect Immun 70, 631–641 (2002).
Koreen, L. et al. spa typing method for discriminating among Staphylococcus aureus isolates: implications for use of a single marker to detect genetic micro- and macrovariation. J Clin Microbiol 42, 792–799 (2004).
Chongtrakool, P. et al. Staphylococcal cassette chromosome mec (SCCmec) typing of methicillin-resistant Staphylococcus aureus strains isolated in 11 Asian countries: a proposal for a new nomenclature for SCCmec elements. Antimicrob Agents Chemother 50, 1001–1012, https://doi.org/10.1128/aac.50.3.1001-1012.2006 (2006).
El Feghaly, R. E., Stamm, J. E., Fritz, S. A. & Burnham, C.-A. D. Presence of the blaZ beta-lactamase gene in isolates of Staphylococcus aureus that appear penicillin susceptible by conventional phenotypic methods. Diagnostic Microbiology and Infectious Disease 74, 388–393, https://doi.org/10.1016/j.diagmicrobio.2012.07.013 (2012).
Kourtis, A. P. et al. Vital Signs: Epidemiology and Recent Trends in Methicillin-Resistant and in Methicillin-Susceptible Staphylococcus aureus Bloodstream Infections - United States. MMWR. Morbidity and mortality weekly report 68, 214–219, https://doi.org/10.15585/mmwr.mm6809e1 (2019).
(ECDC), E. C. f. D. C. a. P. Surveillance of antimicrobial resistance in Europe 2016. Annual Report of the European Antimicrobial Resistance Surveillance Network (EARS-Net). Stockholm, Sweden: ECDC (2017).
Nikolaras, G. P. et al. Changes in the rates and population structure of methicillin-resistant Staphylococcus aureus (MRSA) from bloodstream infections: A single-centre experience (2000–2015). Journal of global antimicrobial resistance 17, 117–122, https://doi.org/10.1016/j.jgar.2018.11.023 (2019).
Sherbuk, J. E., McManus, D., Topal, J. E. & Malinis, M. Improved mortality in Staphylococcus aureus bacteremia with the involvement of antimicrobial stewardship team and infectious disease consultation. Infect Control Hosp Epidemiol 40, 932–935, https://doi.org/10.1017/ice.2019.136 (2019).
Kempley, S. et al. Antibiotic treatment duration and prevention of complications in neonatal Staphylococcus aureus bacteraemia. Journal of Hospital Infection 91, 129–135, https://doi.org/10.1016/j.jhin.2015.07.002 (2015).
Dolapo, O., Dhanireddy, R. & Talati, A. J. Trends of Staphylococcus aureus bloodstream infections in a neonatal intensive care unit from 2000–2009. BMC Pediatrics 14, https://doi.org/10.1186/1471-2431-14-121 (2014).
You, J. H. S. et al. Disease Burden, Characteristics, and Outcomes of Methicillin-Resistant Staphylococcus aureus Bloodstream Infection in Hong Kong. Asia-Pacific journal of public health 29, 451–461, https://doi.org/10.1177/1010539517717365 (2017).
Yarovoy, J. Y., Monte, A. A., Knepper, B. C. & Young, H. L. Epidemiology of Community-Onset Staphylococcus aureus Bacteremia. The western journal of emergency medicine 20, 438–442, https://doi.org/10.5811/westjem.2019.2.41939 (2019).
Austin, E. D. et al. Reduced mortality of Staphylococcus aureus bacteremia in a retrospective cohort study of 2139 patients: 2007–2015. Clin Infect Dis., https://doi.org/10.1093/cid/ciz498 (2019).
You, J. H., Mak, M. M., To, L. Y. & Ip, M. Complicated infections with meticillin-resistant Staphylococcus aureus in Hong Kong. J Hosp Infect 78, 71–72, https://doi.org/10.1016/j.jhin.2010.11.023 (2011).
Chen, X. et al. Epidemiological and genetic diversity of Staphylococcus aureus causing bloodstream infection in Shanghai, 2009–2011. PLoS One 8, e72811, https://doi.org/10.1371/journal.pone.0072811 (2013).
Pomorska-Wesolowska, M. et al. Virulence and antimicrobial resistance of Staphylococcus aureus isolated from bloodstream infections and pneumonia in Southern Poland. Journal of global antimicrobial resistance 11, 100–104, https://doi.org/10.1016/j.jgar.2017.07.009 (2017).
Arias, C. A. et al. A Prospective Cohort Multicenter Study of Molecular Epidemiology and Phylogenomics of Staphylococcus aureus Bacteremia in Nine Latin American Countries. Antimicrob Agents Chemother 61, https://doi.org/10.1128/AAC.00816-17 (2017).
Toleman, M. S. et al. Prospective genomic surveillance of methicillin-resistant Staphylococcus aureus (MRSA) associated with bloodstream infection, England, 1 October 2012 to 30 September 2013. Euro surveillance: bulletin Europeen sur les maladies transmissibles = European communicable disease bulletin 24, https://doi.org/10.2807/1560-7917.ES.2019.24.4.1800215 (2019).
Gu, F. F. et al. Molecular Epidemiology of Staphylococcus aureus among Patients with Skin and Soft Tissue Infections in Two Chinese Hospitals. Chinese medical journal 129, 2319–2324, https://doi.org/10.4103/0366-6999.190673 (2016).
Larsen, J. et al. Emergence of Livestock-Associated Methicillin-Resistant Staphylococcus aureus Bloodstream Infections in Denmark. Clin Infect Dis 65, 1072–1076, https://doi.org/10.1093/cid/cix504 (2017).
Sauget, M. et al. Increasing incidence of bloodstream infections due to Staphylococcus aureus clonal complex 398 in a French hospital between 2010 and 2017. Eur. J. Clin. Microbiol. Infect. Dis., https://doi.org/10.1007/s10096-019-03653-5 (2019).
Bouiller, K. et al. Clonal complex 398 methicillin-susceptible Staphylococcus aureus bloodstream infections are associated with high mortality. Clin. Microbiol. Infect. 22, 451–455, https://doi.org/10.1016/j.cmi.2016.01.018 (2016).
Diene, S. M., Corvaglia, A. R., Francois, P. & van der Mee-Marquet, N., Regional Infection Control Group of the Centre, R. Prophages and adaptation of Staphylococcus aureus ST398 to the human clinic. BMC genomics 18, 133, https://doi.org/10.1186/s12864-017-3516-x (2017).
Acknowledgements
This study was supported by National Natural Science Foundation of China (grant numbers 81772245).
Author information
Authors and Affiliations
Contributions
Conceived and designed the experiments: L.H. and Y.N. Performed the experiments: F.G. and W.H. Analyzed the data F.G., W.H. and S.W. Contributed reagents/materials/analysis tools: S.X., X.L. and Q.Z. Wrote the paper: F.G., W.H. and L.H. Final approval of the submitted manuscript: All.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Gu, F., He, W., Xiao, S. et al. Antimicrobial Resistance and Molecular Epidemiology of Staphylococcus aureus Causing Bloodstream Infections at Ruijin Hospital in Shanghai from 2013 to 2018. Sci Rep 10, 6019 (2020). https://doi.org/10.1038/s41598-020-63248-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-020-63248-5
This article is cited by
-
Predictive models for sepsis in children with Staphylococcus aureus bloodstream infections: a retrospective cohort study
BMC Pediatrics (2023)
-
Emergence of microbial infections in some hospitals of Cairo, Egypt: studying their corresponding antimicrobial resistance profiles
BMC Infectious Diseases (2023)
-
Phenotypic and genotypic characterization of linezolid resistance and the effect of antibiotic combinations on methicillin-resistant Staphylococcus aureus clinical isolates
Annals of Clinical Microbiology and Antimicrobials (2023)
-
Molecular characterization of methicillin-resistant Staphylococcus aureus genotype ST764-SCCmec type II in Thailand
Scientific Reports (2022)
-
Clonality, virulence genes, and antibiotic resistance of Staphylococcus aureus isolated from blood in Shandong, China
BMC Microbiology (2021)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
