
Abstract
It is indicated that lipids profiles are associated with carotid plaque and Atherosclerosis. However, studies about the relationship between serum lipid profiles and carotid plaque composition in Chinese Population is limited. We conducted a cross-sectional study among 3,214 participants between January 2015 and December 2017 in China, to investigate the association between various lipid profiles and the prevalence of carotid plaque. Logistic regression model was used to investigate the association between plasma lipid profiles and odds of carotid plaque. Analysis of covariance (ANCOVA) was used to compare the mean plasma lipid profiles among different number and composition of carotid artery plaques. HDL-C, Non-HDL-C levels, TC/HDL-C, LDL-C/HDL-C were significantly associated with the presence of carotid plaque; HDL-C, LDL-C, Non-HDL-C levels, TC/HDL-C, LDL-C/HDL-C were significantly associated with the presence of common carotid artery (CCA) plaque. Compare with participants without carotid plaque, increased level of LDL-C/HDL-C was found in those with echolucent/polytype plaque. Similarly, compared with participants without CCA plaque, increased level of LDL-C/HDL-C was found in those with echolucent plaque. In conclusion, we found that serum HDL-C, Non-HDLc level, TC/HDLc, and LDLc/HDLc were all associated with the prevalence of carotid plaque, and LDL-C/HDL-C differed among different group of carotid plaque composition.
Similar content being viewed by others

Introduction
Cardiovascular disease (CVD), caused 17.7 million deaths in 2015, is the major cause of death worldwide1. Atherosclerosis is the leading contributor to CVD, and treatment of atherosclerosis is an essential step towards appropriate management and prevention of CVD2. Atherosclerosis is a systemic progression starting at young age and typically remains asymptomatic until late life, which could manifest in multiple vascular beds. Some researchers have demonstrated that atherosclerosis of peripheral vascular like carotid artery is one of the most significant prognostic predictors of cardiovascular morbidity and mortality3,4. Therefore, early detection and treatment of patients with carotid plaque may promote the prevention of CVD. Currently, the majority of carotid ultrasound studies have used carotid intima-medial thickness (IMT) as a surrogate marker for atherosclerosis. However, IMT is not as solid evidence for atherosclerotic infiltration in the arterial wall as significant plaque is5. Several studies indicated that the presence of plaque predicted the onset of cardiovascular and cerebrovascular diseases more accurately than the mean IMT, and the accuracy of this prediction was equivalent to that from pulse wave velocity in hypertensive patients6,7,8.
Lipid profiles have a pivotal role in the CVD pathophysiology and is an important modifiable risk factor for CVD9. Previous studies suggested that lipid profiles (i.e. TC, TG, HDL-C, LDL-C) were significantly associated with carotid plaque10,11,12,13,14. Other studies found that lipid profiles were associated with common carotid artery- intima-media thickness (CCA-IMT) thickening15, carotid intima-media thickness13, carotid femoral-pulse wave velocity (CF-PWV)16, or carotid intima-media roughness17. However, there have been few studies about the relationship between serum lipid profile and carotid plaque composition in Chinese Population. We therefore conducted the current study to investigate the association between various lipid profiles and the prevalence of carotid plaque and carotid plaque composition in a general Chinese population.
Results
Clinical data
A total of 3,214 participants (male: 2,212, females: 1,002) were included in the analysis. The characteristic of study participants are summarized by gender in Table 1. The mean age was 50.5 ± 10.8 years for men and 51.2 ± 10.8 years for women, respectively. Compared with women, men had generally higher glucose (mean: 5.38 vs. 5.16 mmol/L), TG (mean: 1.97 vs. 1.42 mmol/L), TC/HDL-C (mean: 3.91 vs. 3.38 mmol/L), LDL-C/HDL-C (mean: 2.47 vs. 2.17 mmol/L), TG/HDL-C (mean: 1.78 vs. 1.09 mmol/L), and CCA IMT (mean: 0.83 vs. 0.82 mm); lower HDL-C (mean: 1.30 vs. 1.50 mmol/L); and higher prevalence of carotid plaque (40.5% vs. 32.5%), CCA plaque (46.5% vs. 29.7%), ICA plaque (14.3% vs. 6.5%), and ECA plaque (3.7% vs. 1.4%). Additionally, the distribution of counts and the compositions of carotid artery plaques/CCA plaques were also different between genders (P < 0.001).
Associations between lipid profiles and the odds of carotid plaque/CCA plaque
The associations between lipid profiles and the odds of carotid plaque/CCA plaque are presented in Table 2. For all participants, we detected statistically significant associations between: (1) higher HDL-C with lower odds of carotid plaque (fourth versus first quartile: OR, 0.63; 95% CI, 0.47–0.85; P-trend = 0.001) and CCA plaque (fourth versus first quartile: OR, 0.69; 95% CI, 0.52–0.93; P-trend = 0.009); (2) higher LDL-C with higher odds of CCA plaque (fourth versus first quartile: OR, 1.41; 95% CI, 1.09–1.84; P-trend = 0.001); (3) higher Non-HDL-C with higher odds of carotid plaque (fourth versus first quartile: OR, 1.36; 95% CI, 1.04–1.78; P-trend = 0.018) and CCA plaque (fourth versus first quartile: OR, 1.49; 95% CI, 1.13–1.97; P-trend = 0.002); (4) higher TC/HDL-C with higher odds of carotid plaque (fourth versus first quartile: OR, 1.47; 95% CI, 1.12–1.94; P-trend = 0.004) and CCA plaque (fourth versus first quartile: OR, 1.49; 95% CI, 1.13–1.97; P-trend = 0.002); (5) higher LDL-C/HDL-C with higher odds of carotid plaque (fourth versus first quartile: OR, 1.74; 95% CI, 1.32–2.29; P-trend < 0.001) and CCA plaque (fourth versus first quartile: OR, 1.72; 95% CI, 1.31–2.26; P-trend < 0.001).
Association between lipid profiles and carotid plaque composition
The covariate-adjusted mean lipid profiles according to composition of carotid artery/CCA plaques were presented in Tables 3 and 4. Compare with participants without carotid plaque, increased level of LDL-C/HDL-C was found in those with echolucent/polytype plaque. Similarly, compared with participants without CCA plaque, increased level of LDL-C/HDL-C was found in those with echolucent plaque.
Association between lipid profiles and carotid plaque number
The covariate-adjusted mean lipid profiles according to number of carotid artery/CCA plaques were presented in Tables S1, S2. Compare with participants without carotid plaque, increased level of LDLc/HDLc was found in those with ≥3 carotid plaque. Similarly, compared with participants without CCA plaque, increased level of LDL-C/HDL-C was found in those with ≥3 CCA plaque.
Subgroup analyses
The subgroup analyses generally yielded results consistent with the above findings (Table S3). There was no significant effect modification by sex or BMI on the association between lipid profiles and carotid plaque/CCA plaque (all P-values were greater than 0.10).
Discussion
To the best of our knowledge, this is the largest study in China to investigate the association between lipid profiles and the prevalence of carotid plaque and carotid plaque composition. The main results are as follows: serum HDL-C level was negatively associated with odds of carotid plaque and CCA plaque; serum LDL-C level was positively associated with odds of CCA plaque; serum Non-HDLc level, TC/HDLc, and LDLc/HDLc were positively associated with odds of both carotid plaque and CCA plaque. LDL-C/HDL-C differed among different group of carotid plaque composition.
Advanced atherosclerotic plaques are characterized as lipid nucleus which were covered with fibrous caps consisting of extracellular matrix and smooth muscle cells18. Several procedure associated with the progression of the atherosclerotic lesions(e.g. lipids accumulation, thrombosis, proteolysis, inflammation, and apoptosis) might be relevant with the development of plaque. It has been demonstrated that carotid plaque, especially the thick and irregular ones were risks factor for cardiovascular disease19,20,21. Therefore, identification of serum biomarkers related to the presence of plaque would be of great advantage in the prevention of atherosclerosis and CVD. The various lipid profiles examined in our study were related with carotid plaque, thus might be correlated with CVD. Previous studies suggested that lipid profiles have pivotal roles in the pathophysiology of carotid plaque10,11,12,13,14,15,16,17, which is consistent with our study. In contrast, one study in USA found no significant association between HDL-C or TG and carotid plaque, but the authors reported that higher TC, LDL, or non-HDL was associated with higher risk of carotid plaque22. An Algeria cross-sectional study also suggested inconsistent findings: lower HDL-C is associated with higher prevalence level of carotid plaque, but not LDL-C23. The inconsistency might be ascribed to many factors, including the study population heterogeneity, various study regions and different study designs.
Ultrasound (US), a non-radiative and cost-effective technique, is a patient-friendly an ideal method for immediate diagnosis and follow-up24. Previous studies have demonstrated that hypoechoic plaques (echolucent) are more often associated with cardiovascular symptoms than hyperechoic ones (echorich). The meta-analysis conducted by Jashari et al. demonstrated that carotid plaque echogenicity was associated with increased risk of CV events25. However, evidence regarding the relationship between serum lipid profile and carotid plaque composition in Chinese Population is limited. Our study found that LDL-C/HDL-C level was increased in those with echolucent plaque than those without carotid plaque. The analysis from our study provides new evidence for the associations between plaque characterization/features and health related outcomes.
The potential pathophysiological mechanisms through which lipid profiles might increase the risk of carotid plaque are not fully understood. First, the main beneficial effect of HDL cholesterol is to reverse the transport of cholesterol, remove free cholesterol from endothelial macrophages, and return it to the liver for excretion into bile, thus preventing the formation of atherosclerotic plaques26. Second, it has been demonstrated that HDL-C has both direct and indirect anti-inflammatory effects with potential antithrombotic results27.Third, the LDL-C/HDL-C ratio is closely correlated with the distribution of HDL-C subclasses. With the increase of LDL-C/HDL-C ratio, the size of HDL-C particles generally decreases, suggesting that the maturation process of high density lipoprotein is blocked, which may be one of the contributors for the progress of atherosclerosis28.
There were some strengths in this study. First, we collected information on several potential confounders, and the potential effects of them were taken into account. Second, we firstly investigated the association of various lipid parameters and carotid plaque composition in Chinese Population. Third, subgroup analyses generally yielded similar results, indicating that the associations are robust.
Despite these strengths, the study also had several limitations. First, this is a cross-sectional analysis, thus it is difficult to detect the temporal relationship. Second, our study was carried out in a single-center, and these finding should be verified in multi-center study with larger populations. Last, we used ultrasound to assess the presence of plaque, which may be less reliable than the high-resolution magnetic resonance imaging (MRI) or computed tomography (CT). However, one study investigating the accuracy of ultrasound, CT, and MRI in diagnosis of carotid plaque morphology found that ultrasound has higher accuracy for diagnostics of carotid plaque morphology than CT or MRI29. In addition, compared with CT or MRI, ultrasound is safe, noninvasive, and inexpensive30.
In summary, our study demonstrated that serum HDL-C level was associated with lower odds of carotid plaque and CCA plaque; serum LDL-C level was associated with higher odds of CCA plaque; serum non-HDL-C level, TC/HDL-C ratio, and LDL-C/HDL-C ratio were associated with higher odds of carotid plaque and CCA plaque. LDL-C/HDL-C differed among different group of carotid plaque composition. Further prospective studies with larger sample size are needed to verify these associations.
Methods
Study population
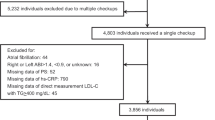
During January 2015 and December 2017, 3,214 consecutive participants (2,212 men, 1,002 women) who underwent a standard medical screening at the Physical Center of the First Affiliated Hospital of Zhengzhou University, China, were included. We excluded participants with the following conditions that might seriously influence carotid plaque and lipid profiles: (1) aged less than 18 years old; (2) with a history of cardiovascular disease, peripheral arterial disease, oncology disease, infectious disease, or serious liver or renal disease; (3) without data on lipid profiles or carotid ultrasound measurements; (4) taking medicine when undergoing the medical examination.
Lipid profiles assessment
Overnight fast blood samples were collected in the morning. Plasma levels of TC, triglycerides (TG), HDL-C, and LDL-C were measured by a fully automatic analyzer, ROCHE (Roche Molecular Systems, Inc. Basel, Switzerland) module Cobas 8000 (C701/C702/C502), and kits were procured by ROCHE. Quality control is maintained by the laboratory with standard procedures. The coefficient of variation for repeated measurements on samples from individual hospitalized patients is maintained at ≤2.5%.
Carotid ultrasound assessment
Carotid ultrasound was assessed by B-mode ultrasound with an Aplio 300 ultrasound system (Toshiba Medical Systems, Tokyo, Japan) by trained and certified technologists. With the subject lying in a supine position, the extracranial carotid arteries were imaged in the longitudinal (anterior, lateral, and posterior views) and transverse planes, the common carotid artery (CCA), the internal carotid artery (ICA), and the external carotid artery (ECA) on both sides were carefully scanned under B-mode imaging from multiple directions. The IMT was defined as the distance between the leading edge of the lumen-intima echo and the leading edge of the media adventitia echo. The carotid intima-media thickness (CIMT) was defined as the mean of the right and left IMT of the CCA.
Carotid plaque is defined as the presence of focal wall thickening that is at least 0.5 mm, or 50% greater than that of the surrounding vessel wall, or as a focal region with CIMT greater than 1.5 mm that protrudes into the lumen that is distinct from the adjacent boundary31. Plaques were classified as echolucent (low grayscale median, lipid rich), echogenic (high grayscale median, mostly occupied by calcified areas), and heterogeneous (mixed echolucent and echogenic)32. If all the plaques had the same composition, the participant was classified as plaque composition, those who had different composition were defined as polytype plaques. All carotid artery plaque measurement was conducted by the same trained physician using the same B-mode ultrasound. The study adopted strict quality control procedures for monitoring and testing consistency in image acquisition and image analysis.
Covariates
A standard physician-administered questionnaire was used to collected information on the demographic characteristics, lifestyle factors, and medical history by trained physicians. Participants who smoked at least one cigarette per day or drank alcohol once a week for at least six months were defined as smokers or drinkers. Weight and height were measured on an auto-anthropometer with subjects wearing light clothing and no shoes. Body mass index (BMI) was calculated as the weight (kg) divided by the square of the height (m). Blood pressure was measured using an electronic device by trained physicians after the subjects sitting relaxed for 10 mins.
Statistical analyses
Descriptive data are presented as mean (standard deviation) for continuous variables and number (percentage) for categorical variables.
Logistic regression model was used to examine the association between plasma lipid profiles and odds of carotid plaque. And two models were developed: Model 1: adjusted for age (years, continuous variable), sex (male or female), and BMI (continuous variable, kg/m2); Model 2: further adjusted for systolic blood pressure (SBP), diastolic blood pressure (DBP), fasting plasma glucose, uric acid, TC (not for TC vs. carotid plaque), TG (not for TG vs. carotid plaque), HDL-C (not for HDL-C vs. carotid plaque) and LDL-C (not for LDL-C vs. carotid plaque).
Analysis of covariance (ANCOVA) was used to compare the mean plasma lipid profiles among different number and composition of carotid artery plaques. The two aforementioned models were also adopted. Subgroup analyses were conducted to investigate whether the relationships between plasma lipid profiles and carotid plaque were modified by sex (men or women) or BMI (<25 kg/m2 or ≥25 kg/m2). Each potential modifier was examined in a separate model by adding a multiplicative interaction term (i.e. potential modifier * lipid profiles).
All analyses were performed with SPSS 21.0 for Windows (SPSS, Inc., Chicago, USA). Two-sided bonferroni correction P values < 0.01 for the difference of covariate-adjusted mean (SEM) among different composition/number of carotid plaque (i.e. None, Echolucent, Echogenic, Heterogeneous, and Polytype). Two-side P values < 0.05 were considered statistically significant for the other associations.
Ethical approval
Ethical approvals for the study were obtained from the ethics committees of the First Affiliated Hospital of Zhengzhou University. Informed consent was obtained from all participants before they participate the study. And all procedures were performed in accordance with the approved guidelines laid down in the Declaration of Helsinki.
Data availability
Additional data are available from the corresponding author for reasonable requesting.
References
Word Health Organization, Fact sheet on Cardiovascualr disease, http://www.who.int/cardiovascular_diseases/en/. Accessed on May 2019., 2017.
Hirata, T. et al. Carotid Plaque Score and Risk of Cardiovascular Mortality in the Oldest Old: Results from the TOOTH Study. Journal of atherosclerosis and thrombosis 25, 55–64 (2018).
Bhatt, D. L. et al. International prevalence, recognition, and treatment of cardiovascular risk factors in outpatients with atherothrombosis. JAMA 295, 180–189 (2006).
JM, U. K.-I., Young, V. & Gillard, J. H. Carotid-artery imaging in the diagnosis and management of patients at risk of stroke. The Lancet. Neurology 8, 569–580 (2009).
Sturlaugsdottir, R. et al. Prevalence and determinants of carotid plaque in the cross-sectional REFINE-Reykjavik study. BMJ open 6, e012457 (2016).
Kawai, T. et al. Carotid plaque score and intima media thickness as predictors of stroke and mortality in hypertensive patients. Hypertension Research: official journal of the Japanese Society of Hypertension 36, 902–909 (2013).
Nambi, V. et al. Carotid intima-media thickness and presence or absence of plaque improves prediction of coronary heart disease risk: the ARIC (Atherosclerosis Risk In Communities) study. Journal of The American College of Cardiology 55, 1600–1607 (2010).
Inaba, Y., Chen, J. A. & Bergmann, S. R. Carotid plaque, compared with carotid intima-media thickness, more accurately predicts coronary artery disease events: a meta-analysis. Atherosclerosis 220, 128–133 (2012).
Grundy, S. M. Small LDL, atherogenic dyslipidemia, and the metabolic syndrome. Circulation 95, 1–4 (1997).
Wang, W. et al. Prediction value of blood lipid levels on newly identified carotid plaque in middle-aged and elderly Chinese population. Zhonghua Xin Xue Guan Bing Za Zhi 38, 1118–1122 (2010).
Zhang, X. T. et al. Association between both triglyceride level, newly identified carotid plaque and middle-aged and elderly population, Beijing. Zhonghua Liu Xing Bing Xue Za Zhi 33, 455–459 (2012).
Luo, Y., Li, J., Guan, D. & Xu, Y. Change and significance of blood lipids during the course of carotid artery plaque formation induced by diabetes mellitus in patients with ischemic cerebral vascular disease. Zhonghua Yi Xue Za Zhi 94, 2279–2281 (2014).
Hou, Q., Li, S., Gao, Y. & Tian, H. Relations of lipid parameters, other variables with carotid intima-media thickness and plaque in the general Chinese adults: an observational study. Lipids Health Dis 17, 107 (2018).
Yang, C. et al. The correlation between serum lipid profile with carotid intima-media thickness and plaque. BMC Cardiovascular Disorders 14, 181 (2014).
Wang, H. M., Chen, T. C., Jiang, S. Q., Liu, Y. J. & Tian, J. W. Association of conventional risk factors for cardiovascular disease with IMT in middle-aged and elderly Chinese. The International Journal of Cardiovascular Imaging 30, 759–768 (2014).
Zhao, X. et al. Serum lipid level and lifestyles are associated with carotid femoral pulse wave velocity among adults: 4.4-year prospectively longitudinal follow-up of a clinical trial. Clinical and Experimental Hypertension (New York, N.Y.: 1993) 40, (487–494 (2018).
Wu, Y. et al. Correlation between carotid intima-media roughness and cardiovascular risk factors. Experimental And Therapeutic. Medicine 18, 49–56 (2019).
Hermus, L., Lefrandt, J. D., Tio, R. A., Breek, J. C. & Zeebregts, C. J. Carotid plaque formation and serum biomarkers. Atherosclerosis 213, 21–29 (2010).
Gepner, A. D. et al. Comparison of Carotid Plaque Score and Coronary Artery Calcium Score for Predicting Cardiovascular Disease Events: The Multi-Ethnic Study of Atherosclerosis. Journal of The American Heart Association 6, e005179 (2017).
Naqvi, T. Z. & Lee, M. S. Carotid intima-media thickness and plaque in cardiovascular risk assessment. JACC. Cardiovascular Imaging 7, 1025–1038 (2014).
Bea, A. M. et al. Association Between the Presence of Carotid Artery Plaque and Cardiovascular Events in Patients With Genetic Hypercholesterolemia. Revista Espanola De Cardiologia (English ed.) 70, 551–558 (2017).
Gardener, H., Della Morte, D., Elkind, M. S., Sacco, R. L. & Rundek, T. Lipids and carotid plaque in the Northern Manhattan Study (NOMAS). BMC Cardiovascular Disorders 9, 55 (2009).
Abi-Ayad, M., Abbou, A., Abi-Ayad, F. Z., Behadada, O. & Benyoucef, M. HDL-C, ApoA1 and VLDL-TG as biomarkers for the carotid plaque presence in patients with metabolic syndrome. Diabetes & Metabolic Syndrome 12, 175–179 (2018).
Picano, E. & Paterni, M. Ultrasound tissue characterization of vulnerable atherosclerotic plaque. International Journal of Molecular Sciences 16, 10121–10133 (2015).
Jashari, F. et al. Carotid plaque echogenicity predicts cerebrovascular symptoms: a systematic review and meta-analysis. European Journal of Neurology 23, 1241–1247 (2016).
Davidson, M. H. & Toth, P. P. High-density lipoprotein metabolism: potential therapeutic targets. The American Journal of Cardiology 100, n32–40 (2007).
Barter, P. J. et al. Antiinflammatory properties of HDL. Circulation Research 95, 764–772 (2004).
Tian, L. et al. Association of the low-density lipoprotein cholesterol/high-density lipoprotein cholesterol ratio and concentrations of plasma lipids with high-density lipoprotein subclass distribution in the Chinese population. Lipids in Health and Disease 9, 69 (2010).
Lukanova, D. V., Nikolov, N. K., Genova, K. Z., Stankev, M. D. & Georgieva, E. V. The Accuracy of Noninvasive Imaging Techniques in Diagnosis of Carotid Plaque Morphology. Open Access Maced J Med Sci 3, 224–230 (2015).
Negi, S. I. & Nambi, V. The role of carotid intimal thickness and plaque imaging in risk stratification for coronary heart disease. Current Atherosclerosis Reports 14, 115–123 (2012).
Stein, J. H. et al. Use of carotid ultrasound to identify subclinical vascular disease and evaluate cardiovascular disease risk: a consensus statement from the American Society of Echocardiography Carotid Intima-Media Thickness Task Force. Endorsed by the Society for Vascular Medicine. Journal of the American Society of Echocardiography: official publication of the American Society of Echocardiography 21, 93–111 (2008).
Vigili de Kreutzenberg, S. et al. Carotid plaque calcification predicts future cardiovascular events in type 2 diabetes. Diabetes Care 38, 1937–1944 (2015).
Acknowledgements
The present study was supported by the National Natural Science Foundation of China (81602852).
Author information
Authors and Affiliations
Contributions
Y.R.X. was the project lead for the current study. Y.H.L., Y.J.Z., W.R.J., D.S., C.Z., C.C.W. and Y.R.X. collected the data. Y.H.L. and Y.J.Z. conducted the data analysis. Y.H.L., Y.J.Z. and Y.C.B. drafted the manuscript. Y.R.X., L.Z., S.X.F., and G.Y.C. revised the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Liu, Y., Zhu, Y., Jia, W. et al. Association between lipid profiles and presence of carotid plaque. Sci Rep 9, 18011 (2019). https://doi.org/10.1038/s41598-019-54285-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-019-54285-w
This article is cited by
-
Relationship between the circulating N-terminal pro B-type natriuretic peptide and the risk of carotid artery plaque in different glucose metabolic states in patients with coronary heart disease: a CSCD-TCM plus study in China
Cardiovascular Diabetology (2023)
-
The predictive value of nontraditional lipid parameters for intracranial and extracranial atherosclerotic stenosis: a hospital-based observational study in China
Lipids in Health and Disease (2023)
-
Association between the atherogenic index of plasma and carotid artery plaques in patients with coronary heart disease in different glucose metabolism states: an RCSCD-TCM study in Tianjin, China
Endocrine (2023)
-
Association between triglyceride glucose index and carotid artery plaque in different glucose metabolic states in patients with coronary heart disease: a RCSCD-TCM study in China
Cardiovascular Diabetology (2022)
-
Effects of Apolipoprotein E polymorphism on carotid intima-media thickness, incident myocardial infarction and incident stroke
Scientific Reports (2022)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
