
Abstract
Background
A body shape index (ABSI) is an emerging anthropometric indicator, challenging two traditional parameters: body mass index (BMI) and waist circumference (WC). We aimed to systematically compare and validate the capability of anthropometric indicators for determining pediatric high blood pressure (HBP).
Methods
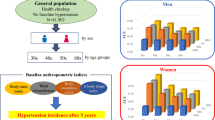
A total of 3150 participants aged 7–17 years were enrolled from Suzhou, China. Areas under the receiver operating characteristic curve (AUC) were obtained to evaluate the performance of anthropometric indicators in detecting HBP. DeLong’s test was used to examine whether the AUCs of anthropometric indicators in contrast to BMI or original ABSI were statistically different. Furthermore, a meta-analysis was performed to combine results from this study and five similar articles from databases.
Results
In Suzhou population, BMI exhibited the largest AUC (AUC = 0.705), followed by WC (AUC = 0.669) and original ABSI (AUC = 0.514). Modified ABSI (AUC: 0.537–0.681), although had slightly better performance than original ABSI, was still less valuable than BMI (P < 0.05), either in the total sample or in boys. The meta-analysis with 21108 children and adolescents subsequently confirms the results derived from Suzhou population.
Conclusions
In predicting pediatric HBP, original ABSI and modified ABSI underperform BMI and WC.
Impact
-
The current study is the first to evaluate whether original ABSI or modified ABSI is comparable to BMI and WC for screening HBP in children and adolescents.
-
In predicting pediatric HBP, original ABSI and modified ABSI do not perform as well as traditional anthropometric indicators, such as BMI and WC.
-
BMI remains the optimal indicator in pediatric HBP screening.
-
This study provides a theoretical basis for the early identification of HBP in children and adolescents by adopting effective predictors.
Similar content being viewed by others


Introduction
High blood pressure (HBP) is recognized as one of the most critical risk factors for cardiovascular disease (CVD)1, and it is gradually becoming more prevalent in youths2. In China, it is reported that the systolic blood pressure (SBP) and diastolic blood pressure (DBP) of children and adolescents aged 7–17 years increased by 6.6 and 4.8 mmHg from 1991 to 2015, respectively, while the prevalence of HBP elevated from 5.7% to 12.8%3. A growing body of evidence indicates that persistent pediatric HBP greatly enhanced the risk of specific target organ damage, HBP, and even CVD in adulthood4,5. Additionally, pediatric HBP is frequently asymptomatic, making it usually underdiagnosed and underestimated6,7. Thus, early identification and effective intervention of HBP in children and adolescents are critical to their long-term health conditions.
In epidemiological studies, there is a dynamic linear relationship between HBP and the epidemic of obesity8,9. The risk of HBP in obese children and adolescents is 4–10 times higher than their normal-weight counterparts10. In general, anthropometric indicators are convenient, practical measurements for clinical applications and routine public health screening for obesity and body shape11. Body mass index (BMI) and waist circumference (WC) are the most common anthropometric indicators12,13. However, as single rough indicators, these two parameters are limited in evaluating full-body (particularly abdominal obesity), potentially resulting in inadequate identification of HBP14,15. For instance, BMI fails to discriminate among fat distributions13. At the same time, WC ignores the effect of height on BP; thus, it may misestimate the risk of HBP to some extent16.
Given this situation, a body shape index (ABSI) has been developed to standardize WC for BMI and height in recent years, estimating abdominal obesity independent of height, weight, or BMI17,18. Therefore, ABSI was suggested to have additional predictive power to compensate for the existing deficiencies of the BMI and WC17,19. Previous studies had shown that ABSI appeared to be a substantial risk factor for premature deaths17 and the onset of diabetes20. A study found a strong association between ABSI and several cardiometabolic markers, such as total cholesterol, triglycerides, and low-density lipoprotein cholesterol21. However, the recent meta-analysis, including 24 retrospective cohort studies and 14 cross-sectional studies conducted in adults, showed that ABSI was superior to BMI and WC in predicting all-cause mortality but inferior in predicting HBP, CVD, and type 2 diabetes22.
Doubts existed that original ABSI, which was developed for American adults, might not be well suited to the rapidly developing body shape conditions of children and adolescents during puberty11,19. Thus, Xu et al.11 and Tong et al.23 had created two modified ABSI equations by standard contour analysis, particularly for the Chinese pediatric population. In contrast to the abundant evidence of ABSI in adults, there are relatively few historical studies exploring this novel indicator among children and adolescents. Meanwhile, regarding the predictive performance for HBP, comparisons between ABSI and traditional obesity measurement indicators, as well as original ABSI versus modified ABSI indicators, are not well-documented and far from conclusion. For example, some studies supported the usage of BMI instead of ABSI23,24,25,26,27, whereas one study28 among Portuguese concluded that ABSI was a better predictor of BP than BMI and WC.
Therefore, the current study were: (1) to compare the ability of different anthropometric indicators, including original ABSI, modified ABSI, BMI, and WC, in discriminating HBP by using school-based data from Suzhou, China; (2) to pool the results of similar studies to determine whether original ABSI or modified ABSI was the optimal predictor of HBP in children and adolescents by a subsequent meta-analysis.
Materials and methods
A cross-sectional study in Suzhou, China
Study design and population
The current study was a cross-sectional study, based on the national surveillance project of common diseases and health influencing factors of students in China, involving children and adolescents aged 7–17 years from Suzhou, Jiangsu Provence. This study adopted a method of multistage, stratified random cluster-sampling from September to October 2019, which was conducted in three steps: firstly, two counties (cities, districts) were selected as the initial sampling unit in Suzhou; secondly, two streets (townships and towns) were selected from each county (city, district); finally, one primary school, one junior high school, and one senior high school were selected from each street (township and town), and all students in two classes were randomly selected from each grade. After excluding incomplete data and students with serious organ diseases, physical disabilities, developmental abnormalities, and other serious metabolic diseases, 3150 children (aged 7–12 years) and adolescents (aged 13–17 years) agreed to participate in the study.
For the recruited participants, informed consent forms in writing duly signed by their guardians were collected before their examination. The project was reviewed by the ethics committees of Suzhou Center for Disease Prevention and Control. All works were carried out with the consent of the students and their parents.
Anthropometric measurements
All measurements were carried out by professionally trained health professionals, using the same equipment and following the same procedures to ensure accuracy. When measuring height and weight, participants were asked to wear light clothing, remove their shoes and hats, and stand erect with heels together with an accuracy of 0.1 cm and 0.1 kg, respectively. WC was measured by exposing the abdomen and breathing gently, using soft anthropometric tape and circumscribing it horizontally around the midpoint between the lower border of the 12 ribs and the upper edge of the iliac crest on both sides precision of 0.1 cm. BMI was calculated as weight (kg) divided by the square of the height (m), and original ABSI was calculated using the following Eq. (1)17. Two modified ABSI, ABSI-ch for children and ABSI-ad1 for adolescents, were calculated using the following Eqs. (2) and (3) by Tong et al.23, while another modified ABSI, ABSI-ad2, was calculated for adolescents using the following Eq. (4) by Xu et al.11.
BP measurement
Surveyors were in strict accordance with the standard requirements to measure BP using an Electronic Blood Pressure Monitor (Omron HBP-1300) of the right size for children and adolescents. All participants were told to sit upright with their backs supported and relax for 15 min simultaneously. The cuff was placed on the non-dominant arm at the heart level, with the balloon’s midline above the brachial pulse. BP was measured twice, and participants rested for at least 2 min between measurements. The average of the two measurements as the final result was recorded. When the difference in BP between two measurements exceeded 10 mmHg, additional measurements were taken, and two similar blood pressure measurements were averaged.
HBP levels were defined as SBP and/or DBP above 95th percentile according to age, sex, and percentile of height, based on the Chinese standard “Reference of screening for elevated Blood pressure among children and adolescents aged 7~18 years” (WS/T 610-2018)29.
Statistical analysis
The basic information about the participants was described in the total sample and by age and sex. Continuous and categorical variables were expressed as [mean ± standard deviation (SD)] and n (%) and were correspondingly compared by using Student’s t-test and Chi-square test, respectively. Receiver operating characteristic (ROC) curves analysis was used to compare the validity of different anthropometric indicators in predicting HBP, resulting in the area under the curve (AUC), corresponding 95% confidential interval (95% CI), cut-off value, sensitivity, and specificity. AUC > 0.7 indicates acceptable screening power30. Meanwhile, DeLong’s test was used to examine whether the AUCs of anthropometric indicators contrast to BMI or original ABSI was meaningfully different31. The Youden index was calculated to determine the optimal cut-off values for different indicators. A two-tailed P value < 0.05 was considered to be statistically significant. All analyses were conducted using SAS statistical software (version 9.4, SAS Institute).
Meta-analysis
Search strategy
Systematic research was conducted on papers published in Medline, PubMed, Embase, Scopus, Ovid, and Web of Science databases and involved in BMI, WC, original ABSI, and modified ABSI in screening HBP up to June 20, 2021. Researchers used the following search strategies: (body mass index OR BMI) AND (waist circumference OR WC) AND (a body shape index OR ABSI) AND (anthropometric indexes) AND (high blood pressure OR HBP OR hypertension OR elevated blood pressure) AND (child OR children OR adolescents OR teenager OR young) AND (receiver operating characteristic curve OR ROC OR area under curve OR AUC).
Two reviewers (W.G. and C.X.) made an independent primary screening of the title and abstract, and then obtained the relevant articles’ full text to determine inclusion eligibility. Disagreements were discussed by the team or adjudicated by the third researcher (J.H.). References to related studies were browsed to identify additional valuable studies.
Inclusion/exclusion criteria
Articles were included if they satisfied the following criterias: (1) status of HBP was assessed; (2) subjects between 7 and 18 years old; (3) either original ABSI using Eq. (1) or modified ABSI using Eqs. (2–4) as mentioned above were calculated, and was compared to BMI; (4) AUC and corresponding 95%CI were reported. The language of articles was restricted to English. Duplicated articles based on the same study, conference abstracts, reviews, and intervention studies were not included.
Data extraction and quality assessments
Study characteristics of the included literature were extracted independently by two investigators (W.G. and C.X.), including the type of study design, sample size, country, ethnicity, the definition of HBP, equations of ABSI, as well as age, sex distribution of the included participants. Meanwhile, the AUC (95% CI) of each anthropometric indicator for identifying HBP was also extracted.
Furthermore, QUADAS-2 was used to evaluate the study quality32. The included study was evaluated in two aspects: risk of bias (patient selection, index test, reference standard, and flow and time) and applicability concerns (patient selection, index test, and reference standard). The study quality was described as “high,” “low,” or “unclear“32.
Statistical analysis
Stata 15.0 was used to pool AUCs and 95% CIs together. I2 statistics and Cochrane’s Q statistics were used to assess the heterogeneity33. If there was no heterogeneity between studies (I2 ≤ 50% and P ≥ 0.1), a fixed-effect model was used; otherwise, a random-effect model was applied. The standard deviation of the difference between BMI and other anthropometric indicators of AUC was calculated assuming a correlation of 0.95 (ref. 34).
Results
A cross-sectional study in Suzhou, China
Baseline characteristics of the participants
Table 1 demonstrates the basic characteristics of the Suzhou population according to HBP status. Among the 3150 participants, 1944 children aged 7–12 years and 1206 adolescents aged 13–17 years; meanwhile, boys accounted for 50.86%. The prevalence of HBP in the total sample, children, and adolescents were 11.27%, 10.60%, and 12.35%, respectively. Participants with HBP had significantly higher SBP, DBP, weight, BMI, and WC than participants without HBP (all P < 0.05). Interestingly, original ABSI and modified ABSI (i.e., ABSI-ch, ABSI-ad1, and ABSI-ad2) did not always differ between HBP and Non-HBP groups in the total sample or the subsets divided by age and sex.
ROC analysis of the anthropometric indicators for predicting HBP
As shown in Table 2, BMI had the highest AUC for HBP (AUC: 0.672–0.747), followed by WC (AUC: 0.624–0.720) and ABSI (AUC: 0.498–0.591). The optimal cut-off values for original ABSI, ABSI-ch, ABSI-ad1, and ABSI-ad2 were relatively small and quite close to each other. Although the predictive powers for HBP of ABSI-ch (AUC: 0.613, 95% CI: 0.570, 0.655) among children, ABSI-ad1 (AUC: 0.624, 95% CI: 0.573, 0.675), and ABSI-ad2 (AUC: 0.642, 95% CI: 0.592, 0.692) among adolescent, had significantly improved compared to original ABSI, they were still weaker than BMI (P < 0.05). Meanwhile, in girls, the ability of modified ABSI (i.e., ABSI-ch, ABSI-ad1, and ABSI-ad2) to predict HBP in contrast to original ABSI was not significantly improved.
Meta-analysis
Eligible studies
According to the search strategy, we got 99 relevant articles, of which 44 were excluded for duplicate articles. After browsing the title and abstract, 40 papers were excluded because they were irrelevant to the research purpose. Fifteen papers were retained after full-text evaluation. For the two articles11,23 that adopted data from the same study, the report23 with the larger sample size was finally included. Three papers21,28,35 were excluded because they did not report the results of AUC and 95% CI. Finally, five papers23,24,25,26,27 were included for the meta-analysis, and the selective process is shown in Fig. 1.

ABSI a body shape index, ROC receiver operating characteristic, AUC area under the curve, CI confidential interval.
Characteristics of included papers and quality assessment
Table 3 presents the characteristics and outcome definitions of the current study and other five studies with 17958 participants aged 7–18 years. All included studies were published from 2018 to 2020 and had a cross-sectional design. In summary, three studies were conducted in Asia23,25,26, and the others were from South America27 and Europe24. In total, four papers23,24,26,27 analyzed original equation of ABSI (Eq. 1), two papers25,27 calculated ABSI using modified equation for adolescents (Eq. 4); another one23 used a different modified equation for children (Eq. 2) and adolescents (Eq. 3), respectively. The quality assessment of included studies is shown in Table S1. The risk of bias for the current and other studies were evaluated as “low” in all domains. For studies that adopted original ABSI (Eq. 1)24,26 and a modified ABSI (Eq. 4)25,27 for Chinese adolescents, the results for assessing applicability were uncertain.
Figures 2 and 3 show the pooled AUCs of anthropometric indicators for screening HBP in children and adolescents by sex. Forrest plots present the pooled AUC values of BMI (AUC: 0.652–0.710), WC (AUC: 0.605–0.688), and ABSI (AUC: 0.492–0.547). In adolescents, the pooled AUC value for modified ABSI in boys was 0.646 (95% CI: 0.584, 0.709), and corresponding pooled AUC value in girls was 0.577 (95% CI: 0.520, 0.633). In children, BMI offered superior performance in predicting pediatric HBP than both original ABSI and ABSI-ch (Table S2). In adolescents, BMI remained to be the best indicator (Table S3).

Panel A: boys and panel B: girls. cUsed the modified ABSI equation for Chinese children by Tong et al.23.

Discussion
Based on a cross-sectional survey in Suzhou city and a subsequent meta-analysis, we compared the predictive power for HBP of BMI, WC, original ABSI, and modified ABSI in children and adolescents. We found that ABSI was inferior to BMI in screening pediatric HBP, which was consistent with a similar meta-analysis on adults22. Although the predictive powers of modified ABSI for HBP were improved after modifying the scale exponents in children and adolescents, they were still weaker than BMI. The current study suggested that BMI was still the optimal choice for evaluating the effect of obesity on HBP in children and adolescents.
The cardiovascular risks contributed by overweight and obesity in children and adolescents were well documented10. As we know, the risk of disease associated with obesity involves increased amounts and the distribution of fat tissue. In adults, the indicator of abdominal obesity (i.e., WC) has been suggested to be more tightly associated with the development and progression of CVD than BMI36. Our meta-analysis further supported the most excellent BMI effect on HBP than WC regardless of age and sex. The results were consistent with a recent meta-analysis that compared obesity indicators for predicting pediatric HBP36. The above evidence supports the view that in the pediatric population, BMI may provide sufficient information on visceral fat37. A reasonable biological explanation could be that subcutaneous fat accounts for nearly 90% of abdominal obesity in the pediatric population, while visceral fat accounts for a relatively small percentage38. Simultaneously, BMI was better associated with subcutaneous fat than visceral fat39. Therefore, BMI remains the optimal indicator in pediatric HBP screening.
ABSI, a novel supplement to the abdominal obesity indicator, was highly expected to predict chronic diseases17. Previous studies had found a high correlation between ABSI and age17. However, in the current study, it was found that original ABSI had insufficient predictive power in predicting pediatric HBP than BMI and WC, even in subgroups stratified for age. Notably, the predictive power of modified ABSI (i.e., ABSI-ch, ABSI-ad1, and ABSI-ad2) for HBP was unsatisfactory. It was reported that the curve of ABSI had a high peak but a small standard deviation22, making it challenging to define an optimal cut-off value for clinical practice. It should also be kept in mind that Chung et al.18 proposed a log-transformed ABSI with z-score (LBSIZ), which was revealed to be significantly associated with hypertension in adults. However, it remained unclear whether LBSIZ was appropriate for children and adolescents. Overall, the complexity in calculation and the inferior performance in prediction hamper the usage of ABSI in screening pediatric HBP.
To the best of our knowledge, the current study is the first to evaluate whether original ABSI or modified ABSI is comparable to BMI and WC for screening HBP in children and adolescents, through new original data from a cross-sectional study in Suzhou and meta-analysis. The large sample size and racial variety of similar studies largely increase the generalizability and robustness of our findings. However, we should admit that there were some shortcomings in our study. First, all the included studies had a cross-sectional design that could not reveal the causal relationship between ABSI and HBP. Therefore, future longitudinal studies on the current topic are warranted. Second, the included papers are mainly from Asia, making it difficult to conduct an ethnically stratified meta-analysis. Finally, the incomplete concordance of the diagnostic criteria for HBP in children and adolescents may potentially impact our results.
In summary, the current study found that ABSI may not be a favorable indicator for predicting HBP in children and adolescents. In comparison, BMI remains a crucial anthropometric indicator for detecting HBP at present. Further studies are required to verify the current results’ accuracy and whether the results are consistent across race and sex.
References
Joseph, P. et al. Reducing the global burden of cardiovascular disease, Part 1: The epidemiology and risk factors. Circ. Res. 121, 677–694 (2017).
Flynn, J. T. et al. Clinical practice guideline for screening and management of high blood pressure in children and adolescents. Pediatrics 140, e20171904 (2017).
Ma, S. J., Yang, L., Zhao, M. & Xi, B. Changing trends in the level of blood pressure and prevalence of hypertension among children and adolescents from 1991 to 2015. Chin. J. Epidemiol. 41, 178–183 (2020) (in Chinese).
Kollias, A., Dafni, M., Poulidakis, E., Ntineri, A. & Stergiou, G. S. Out-of-office blood pressure and target organ damage in children and adolescents: a systematic review and meta-analysis. J. Hypertens. 32, 2315–2331 (2014). Discussion 2331.
Kollias, A. et al. Adiposity, blood pressure, and carotid intima-media thickness in greek adolescents. Obesity (Silver Spring) 21, 1013–1017 (2013).
Brady, T. M., Solomon, B. S., Neu, A. M., Siberry, G. K. & Parekh, R. S. Patient-, provider-, and clinic-level predictors of unrecognized elevated blood pressure in children. Pediatrics 125, e1286–e1293 (2010).
Hansen, M. L., Gunn, P. W. & Kaelber, D. C. Underdiagnosis of hypertension in children and adolescents. JAMA 298, 874–879 (2007).
Okafor, C., Anyaehie, U. & Ofoegbu, E. The magnitude of obesity and its relationship to blood pressure among the residents of enugu metropolis in South East Nigeria. Ann. Med. Health Sci. Res. 4, 624–629 (2014).
Chandra, A. et al. The relationship of body mass and fat distribution with incident hypertension: observations from the Dallas Heart Study. J. Am. Coll. Cardiol. 64, 997–1002 (2014).
Koebnick, C. et al. High blood pressure in overweight and obese youth: implications for screening. J. Clin. Hypertens. (Greenwich) 15, 793–805 (2013).
Xu, Y., Yan, W. & Cheung, Y. B. Body shape indices and cardiometabolic risk in adolescents. Ann. Hum. Biol. 42, 70–75 (2015).
Wang, M. et al. Body mass index percentiles and elevated blood pressure among children and adolescents. J. Hum. Hypertens. 34, 319–325 (2020).
Ononamadu, C. J. et al. Comparative analysis of anthropometric indices of obesity as correlates and potential predictors of risk for hypertension and prehypertension in a population in Nigeria. Cardiovasc. J. Afr. 28, 92–99 (2017).
Wang, S. et al. A novel quantitative body shape score for detecting association between obesity and hypertension in China. BMC Public Health 15, 7 (2015).
Jung, C., Fischer, N., Fritzenwanger, M. & Figulla, H. R. Anthropometric indices as predictors of the metabolic syndrome and its components in adolescents. Pediatr. Int. 52, 402–409 (2010).
Song, L. et al. Height and prevalence of hypertension in a middle-aged and older Chinese population. Sci. Rep. 6, 39480 (2016).
Krakauer, N. Y. & Krakauer, J. C. A new body shape index predicts mortality hazard independently of body mass index. PLoS ONE 7, e39504 (2012).
Chung, W., Park, C. G. & Ryu, O. H. Association of a new measure of obesity with hypertension and health-related quality of life. PLoS ONE 11, e0155399 (2016).
Cheung, Y. B. “A body shape index” in middle-age and older Indonesian population: scaling exponents and association with incident hypertension. PLoS ONE 9, e85421 (2014).
He, S. & Chen, X. Could the new body shape index predict the new onset of diabetes mellitus in the Chinese population? PLoS ONE 8, e50573 (2013).
Mameli, C. et al. The association between a body shape index and cardiovascular risk in overweight and obese children and adolescents. PLoS ONE 13, e0190426 (2018).
Ji, M., Zhang, S. & An, R. Effectiveness of a body shape index (ABSI) in predicting chronic diseases and mortality: a systematic review and meta-analysis. Obes. Rev. 19, 737–759 (2018).
Tong, Y. & Han, E. Associations between body shape, body adiposity and other indices: a case study of hypertension in Chinese children and adolescents. Ann. Hum. Biol. 46, 460–466 (2019).
Perona, J. S. et al. Waist circumference and abdominal volume index are the strongest anthropometric discriminators of metabolic syndrome in spanish adolescents. Eur. J. Clin. Invest. 49, e13060 (2019).
Tee, J. Y. H., Gan, W. Y. & Lim, P. Y. Comparisons of body mass index, waist circumference, waist-to-height ratio and a body shape index (ABSI) in predicting high blood pressure among Malaysian adolescents: a cross-sectional study. BMJ Open 10, e032874 (2020).
Yazdi, M. et al. Validity of anthropometric indices in predicting high blood pressure risk factors in Iranian children and adolescents: Caspian-V Study. J. Clin. Hypertens. (Greenwich) 22, 1009–1017 (2020).
Cristine Silva, K., Santana Paiva, N., Rocha de Faria, F., Franceschini, S. & Eloiza Piore, S. Predictive ability of seven anthropometric indices for cardiovascular risk markers and metabolic syndrome in adolescents. J. Adolesc. Health 66, 491–498 (2020).
Duncan, M. J., Mota, J., Vale, S., Santos, M. P. & Ribeiro, J. C. Associations between body mass index, waist circumference and body shape index with resting blood pressure in Portuguese adolescents. Ann. Hum. Biol. 40, 163–167 (2013).
National Health Commission of the People’s Republic of China. WS/T 610-2018 Reference of Screening for Elevated Blood Pressure among children and adolescents aged 7~18 years (Standards Press of China, 2018).
Metz, C. E. Some practical issues of experimental design and data analysis in radiological ROC studies. Invest. Radiol. 24, 234–245 (1989).
DeLong E. R., D D., Clarke-Pearson D. L. Comparing the areas under two or more correlated receiver operating characteristic curves: a nonparametric approach. Biometrics 44, 837–845 (1988).
Whiting, P. F., R, A., Westwood, M. E. & Mallett, S. Quadas-2: a revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 155, 529–536 (2011).
Baker, W. L. et al. Understanding heterogeneity in meta-analysis: the role of meta-regression. Int J. Clin. Pract. 63, 1426–1434 (2009).
Ashwell, M., Gunn, P. & Gibson, S. Waist-to-height ratio is a better screening tool than waist circumference and BMI for adult cardiometabolic risk factors: systematic review and meta-analysis. Obes. Rev. 13, 275–286 (2012).
Lek, N., Yan, W., Zhang, Y., Wang, Q. & Cheung, Y. B. Indices of central and general obesity and cardiometabolic risk among adolescents in three ethnic groups in North-West China. Ann. Hum. Biol. 43, 18–24 (2016).
Lo, K., Wong, M., Khalechelvam, P. & Tam, W. Waist-to-height ratio, body mass index and waist circumference for screening paediatric cardio-metabolic risk factors: a meta-analysis. Obes. Rev. 17, 1258–1275 (2016).
Koren, D. et al. Anthropometric predictors of visceral adiposity in normal-weight and obese adolescents. Pediatr. Diabetes 14, 575–584 (2013).
Brambilla, P. et al. Crossvalidation of anthropometry against magnetic resonance imaging for the assessment of visceral and subcutaneous adipose tissue in children. Int J. Obes. (Lond.) 30, 23–30 (2006).
Benfield, L. L. et al. Magnetic resonance imaging of abdominal adiposity in a large cohort of british children. Int. J. Obes. (Lond.) 32, 91–99 (2008).
Acknowledgements
This study was supported by the National Natural Science Foundation of China (grant: 81602911), Natural Science Foundation of Jiangsu Province-Youth Project (BK20160337), Priority Academic Program Development of Jiangsu Higher Education Institutions (PAPD), Gusu Health Talents Program Training Project in Suzhou, China (GSWS2020100).
Author information
Authors and Affiliations
Contributions
J.Y.Y. and J.H. contributed to the design and concept of the manuscript. W.X.G., C.Q.X., and L.P.Y. were responsible for the analysis, interpretation of data, and manuscript drafting. Y.X., J.Y.L., and F.L. were responsible for the critical revision of the manuscript for intellectual content. All authors were involved in writing the paper and had final approval of the submitted and published versions.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Consent statement
For the recruited participants, informed consent forms in writing duly signed by their guardians were collected before their examination. The project was reviewed by the ethics committees of the Suzhou Center for Disease Prevention and Control.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Ge, W., Yi, L., Xiao, C. et al. Effectiveness of a body shape index in predicting pediatric high blood pressure. Pediatr Res 92, 871–879 (2022). https://doi.org/10.1038/s41390-021-01844-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41390-021-01844-5
This article is cited by
-
Tri-ponderal mass index and left ventricular hypertrophy in a cohort of caucasian children and adolescents with obesity
Italian Journal of Pediatrics (2024)
