
Abstract
Background
Evidence suggests that fronto-limbic brain regions and connecting white matter fibre tracts in the left hemisphere are more sensitive to glucocorticoids than in the right hemisphere. It is unknown whether treatment with glucocorticoids in childhood is associated with microstructural differences of the uncinate fasciculus and cingulum bundle, which connect fronto-limbic brain regions. Here, we tested the hypothesis that prior glucocorticoid treatment would be associated with differences in fractional anisotropy (FA) of the left relative to right uncinate fasciculus and cingulum bundle.
Methods
We performed diffusion-weighted imaging in 28 children and adolescents aged 7–16 years previously treated with glucocorticoids for nephrotic syndrome or rheumatic disease and 28 healthy controls.
Results
Patients displayed significantly different asymmetry in the microstructure of uncinate fasciculus with higher left but similar right uncinate fasciculus FA and axial diffusivity compared to controls. No apparent differences were observed for the cingulum. Notably, higher cumulative glucocorticoid doses were significantly associated with higher uncinate fasciculus FA and axial diffusivity bilaterally.
Conclusions
Our findings indicate that previous glucocorticoid treatment for non-cerebral diseases in children and adolescents is associated with long-term changes in the microstructure of the uncinate fasciculi, and that higher cumulative glucocorticoid doses have a proportional impact on the microstructure.
Impact
-
It is unknown if treatment with glucocorticoids in childhood have long-term effects on fronto-limbic white matter microstructure.
-
The study examined if children and adolescents previously treated with glucocorticoids for nephrotic syndrome or rheumatic disorder differed in fronto-limbic white matter microstructure compared to healthy controls.
-
The nephrotic and rheumatic patients had higher left but similar right uncinate fasciculus FA and axial diffusivity.
-
Higher bilateral uncinate fasciculus FA and axial diffusivity was associated with higher cumulative glucocorticoid doses.
-
We revealed new evidence suggesting that previous glucocorticoid treatment for non-cerebral diseases in children and adolescents is associated with long-term changes in uncinate fasciculi microstructure.
Similar content being viewed by others


Introduction
Exogenous glucocorticoids are used with great benefit in the treatment of many diseases due its anti-inflammatory and immunosuppressive properties.1 However, the question as to whether glucocorticoid therapy may trigger persistent changes in the cellular microstructure of the maturing brain remains unresolved.2 Endogenous glucocorticoids are released into the bloodstream by the adrenal glands following activation of the hypothalamic-pituitary-adrenal axis (HPA axis) in response to a stressor such as perceived danger or pain. Glucocorticoids target mineralocorticoid and glucocorticoid receptors in most tissues and organs, including the brain, to facilitate metabolic, endocrine and immune functions through genomic, epigenomic and rapid non-genomic mechanisms.3,4 Glucocorticoid receptors are widely distributed across the brain, while mineralocorticoid receptors primarily are found in the hippocampus, amygdala and dorsolateral septum.5 Prenatal exposure to stress and excess levels of glucocorticoids may have detrimental effects on developing neurons and glia cells in the brain.6 Because postnatal brain maturation is characterized by dendritic and axonal arborization, and myelination of axons,7 the developing brain may show a heightened susceptibility to circulating glucocorticoids through childhood and adolescence as well.
Magnetic resonance imaging (MRI) studies on the associations between glucocorticoids and the brain in children and adolescents have mainly focused on variations in endogenous cortisol levels. Accumulating evidence suggests that higher levels of glucocorticoids predominantly impact fronto-limbic brain structures such as orbitofrontal cortex (OFC), ventro- and dorsomedial prefrontal cortex (PFC), anterior cingulate cortex (ACC), amygdala and hippocampus. Functional MRI (fMRI) studies have observed that exposure to heightened levels of cortisol is coupled to differences in fronto-limbic functional connectivity in infants8,9 and children and adolescents.10,11 Resting-state fMRI was recently used in infants to show that higher maternal cortisol levels during pregnancy were associated with weaker functional connectivity between the hippocampus and ACC,9 as well as stronger functional connectivity between amygdala and the dorsal attention network and default mode network in infant girls, with the opposite relationship being apparent in infant boys.8 Heightened cortisol levels in preschool children were observed to predict decreased resting-state functional connectivity between the left amygdala and medial OFC in late adolescence.10 Furthermore, a task-based fMRI study observed higher cortisol levels to be associated with stronger negative coupling between the right amygdala and bilateral medial PFC, when viewing fearful facial expressions, in previously institutionalized children compared to never institutionalized controls.11 Structural MRI studies in school-aged children have also reported associations between glucocorticoids and fronto-limbic brain structures. Higher evening cortisol levels and posttraumatic symptoms have been associated with smaller left ventromedial PFC volume,12 and with reduced right hippocampal volume at 12–18 months follow-up.13 Lastly, prenatal exposure to increased levels of glucocorticoids was coupled to sustained reductions in cortical thickness in fronto-limbic brain regions in children assessed at school age.14 To the best of our knowledge, no studies have so far examined the effect of glucocorticoid treatment for extra-cerebral diseases during childhood on white matter microstructure.
Studies across species suggest that glucocorticoids may impact the two brain hemispheres differently, with the left hemisphere being more sensitive to high levels of glucocorticoids than the right hemisphere.15,16 In rodents, exposure to high doses of exogenous glucocorticoids has been related to smaller left but not right ACC volume.17 Moreover, adult rats exposed to chronic psychosocial stress displayed suppressed cell proliferation and survival rate of newborn cells to a greater extent in left relative to the right medial PFC.18 In humans, children with higher evening cortisol levels had proportionally smaller left ventromedial PFC.12 Furthermore, diffusion-weighted imaging (DWI) studies in healthy adults have linked endogenous cortisol levels to hemispheric asymmetry in fronto-limbic grey and white matter microstructure. Specifically, higher daily cortisol levels were shown to be associated with higher left relative to right hippocampal mean diffusivity.19 In addition, a higher cortisol awakening response (CAR) was linked to hemispheric asymmetry in uncinate fasciculus and cingulum fractional anisotropy (FA),20 a measure that reflects the degree of directionality of water diffusion in tissue that is influenced by differences in such as axonal count, diameter, myelination and organization.21 The uncinate fasciculus and the cingulum bundle are major fronto-limbic fibre tracts connecting, respectively, the OFC and ventromedial PFC, and the dorsomedial PFC and ACC with the amygdala and hippocampus.22 Because the uncinate fasciculus and the cingulum bundle show considerable maturation throughout childhood and adolescence,23 it seems plausible that these fronto-limbic fibre tracts are vulnerable to excessive glucocorticoid levels in children and adolescents.
The current study aimed to investigate the possible long-term effects of previous glucocorticoid treatment in childhood and adolescence on the microstructure of the uncinate fasciculus and the cingulum using DWI. To address this question, we compared children and adolescents previously treated with glucocorticoids for nephrotic syndrome or rheumatic disease, both non-cerebral diseases, to healthy controls. Nephrotic syndrome is related to the loss of protein through the kidneys,24 whereas rheumatic disease is characterized by inflammation of the muscles or joints.25 We included these two patient groups, which differ considerably in disease aetiology and symptomatology because we wished to control for possible disease-specific effects, unrelated to the glucocorticoid treatment. Our rationale was that the disease-specific effects of nephrotic syndrome and rheumatic disease would not cause similar microstructural changes in the same white matter fibre tracts. Thus, observed differences between patients and controls should largely be explained by exposure to glucocorticoids rather than the course of illness.
Methods
Participants
Twenty-eight patients (19 girls, 9 boys), aged 7–16 years, previously treated with glucocorticoids for rheumatic disease (n = 17) or nephrotic syndrome (n = 11), and 28 healthy controls matched on age, sex and parental education were included in the study. Initially, 38 patients with rheumatic disease (n = 24) or nephrotic syndrome (n = 14), and 42 healthy controls were recruited to the study.26 Ten patients and 13 controls were subsequently excluded from the DWI analysis, because they did not complete the MR scan (seven patients, six controls), had reduced image quality (two patients, two controls), or had resumed glucocorticoid treatment prior to the scan (one patient). In addition, six controls were excluded to ensure that groups were matched on age, sex and parental education. Demographic data are presented in Table 1 and patient diagnoses are presented in Table 2.
Patients were recruited from outpatient clinics in Denmark. Healthy controls were recruited in collaboration with public schools in the Capital Region of Denmark. Participants and their parents received thorough information regarding the project and written consent was obtained from all parents before study initiation. The study was approved by the Committee on Biomedical Research Ethics for the Capital Region of Denmark (protocol no. H-KF-01-131/03) and was conducted in accordance with the Declaration of Helsinki.
All subjects underwent a standardized neurological examination by a medical doctor (S.K.H.). Exclusion criteria for all participants were parent-reported preterm birth, perinatal treatment with glucocorticoids or any known neurological or psychiatric disorders or psychiatric disorders of first-degree relatives. Control subjects reporting any systematically glucocorticoid treatment or atypical medical history were excluded. The patients’ hospital case notes were reviewed, and patients were excluded if they had resumed glucocorticoid treatment at the time of the study, or if there was any record of neurological complications. We have previously reported that the nephrotic and rheumatic patients in present study displayed reduced verbal skills,26 had smaller total brain volumes,27 reduced subcortical grey matter volumes and lower right hippocampal mean diffusivity,28 and showed sex-dependent higher diurnal cortisol levels.29
Glucocorticoid treatment variables
Body weight and glucocorticoid doses were recorded from the children’s hospital case notes. The weight-adjusted daily prednisone equivalent doses were summed to estimate the weight-adjusted cumulative glucocorticoid dose. The median and mean of the weight-adjusted daily glucocorticoid dose was estimated based on all daily doses. Glucocorticoid dose calculations are described in detail elsewhere.26 Secondary treatment variables were furthermore calculated to adjust for confounding factors related to the course of treatment and to provide descriptive treatment data on the patients. Treatment variables are presented in Table 3.
Control variables
Measures of the participant’s pubertal development, verbal intellectual abilities, stressful life events (SLEs) and diurnal cortisol levels were included as possible confounders that might mediate possible group differences in fronto-limbic fibre tract asymmetry. Control variables are shown in Table 1 and have previously been reported elsewhere for larger sample sizes.26,29
Subjects were assessed on two separate days. On day 1, subjects underwent a standardized neurological examination and assessment of pubertal development using Tanner staging by a medical doctor (S.K.H.). The participants’ verbal intellectual abilities were assessed by a psychologist (M.V.) and estimated with the verbal comprehension index (VCI) based on the Information and Vocabulary sub-tasks from the Wechsler Intelligence Scale for Children, Third Edition (WISC III). Previously experienced SLEs during the child’s lifetime were assessed with a parent-reported questionnaire. One male control and one male patient with rheumatic disease had missing SLE data. On day 2, subjects underwent MR scanning. The number of days between the two assessment days ranged from 0 to 67 days (median = 22.5).
Participants’ endogenous cortisol levels were assessed at home on two consecutive schooldays using oral swabs. On each sampling day, participants collected eight saliva samples at 0, 15, 30, 45 and 60 min after morning awakening and around noon, and 4 and 8 p.m. Area under the curve ground was used to estimate daily cortisol output using the first morning sample, and the three samples collected from noon to evening adjusting for the sampling time (nmol/L/min). CAR was estimated as the relative difference between the morning peak sample and the area under the curve ground of the five morning samples adjusted for sampling time. One male control had missing data for CAR and one female patient with rheumatic disease had missing data for daily cortisol output and CAR. For further details on the procedures and calculations see ref. 29.
Magnetic resonance imaging
All subjects were scanned using a 3 Tesla Siemens Magnetom Trio MR scanner (Siemens, Erlangen, Germany) with an eight-channel head coil (Invivo, FL). Whole-brain 3D T1-weighted magnetization prepared rapid gradient echo images were acquired (echo time (TE) = 3.04 ms, repetition time (TR) = 1550 ms, matrix = 256 × 256 mm2, 192 sagittal slices, no gap, 1 mm3 voxels). DW images of the whole brain were acquired using a twice-refocused balanced spin echo sequence to minimize eddy current distortion.30 Ten non-DW images (b = 0) and 61 DW images (b = 1200), encoded along independent collinear diffusion gradient orientations, were acquired (TR = 8200 ms, TE = 100 ms, field of view = 220 × 220 mm2, matrix = 96 × 96, GRAPPA: factor 2, 48 lines, 61 perpendicular slices with no gap, 2.3 mm3 voxels). A gradient echo field map was acquired to correct for B0 field distortions (TR = 530 ms, TE[1] = 5.19 ms and TE[2] = 7.65 ms, field of view = 256 × 256 mm2, matrix = 128 × 128, 47 perpendicular slices with no gap, 2 × 2 × 3 mm3 voxels). Images were oriented parallel to the anterior–posterior commissure line.
Image preprocessing
Images were preprocessed using pipelines implemented in Matlab, using mainly SPM8 routines. First, the T1-weighted images were rigidly oriented to MNI (Montreal Neurosciences Institute) space (six-parameter mutual information) and corrected for spatial distortions due to non-linearity in the gradient system of the scanner.31 Then, the mean b0 image was rigidly registered to the T1-weighted image. Next, all DW images were rigidly coregistered with no re-slicing to the mean b0 image and corrected for geometric distortions using a voxel displacement map based on both the acquired B0 field map32 and the scanner specific gradient non-linearity distortions.31 Subsequently, all DW images were resliced using tri-linear interpolation. Importantly, the above procedure ensures that only one re-slicing step was employed. The diffusion gradient orientations were adjusted to account for any rotation applied during registration. A brain mask was created by applying BET33 on each non-DW image and taking the median of the individual masks. The resulting mask was applied to all DW images. The diffusion tensor was fitted using a least-squares fit by non-linear optimization employing a Levenburg–Marquardt algorithm34 and constrained to be positively definite by fitting its Cholesky decomposition implemented in Camino.35 FA, axial diffusivity (AD) and radial diffusivity (RD) were calculated.
Inter-subject spatial normalization of fibre tracts
Tract-based spatial statistics (part of FSL 4.1.4) was used for spatial normalization and alignment of fibre tracts.36 Subjects’ FA images were aligned into a common space using the non-linear registration tool FNIRT.37 The most representative subject was identified by non-linearly registering the FA images of all participants to the FA images of every other participant, and then used as a study-specific target. The target FA image was then aligned to MNI space using affine registration. Subsequently, the entire data set was aligned and transformed into 1 mm3 MNI space by combining the non-linear and affine registrations in one re-slicing step using tri-linear interpolation (default). A mean cross-subject FA image was created and thinned to create a study-specific mean FA skeleton thresholded at FA > 0.25, containing 132,162 1 mm3 interpolated isotropic voxels. Each subject’s aligned FA image was then projected onto the mean skeleton. The non-linear warps and the skeleton projections were also applied to the AD and RD data.
Regions of interest
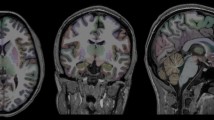
Regions of interest (ROIs) of the left and right cingulum and uncinate fasciculi were drawn onto the mean skeleton using the white MRI atlas of Human White Matter38 and the JHU White Matter Tractography Atlas implemented in FSLview39 for guidance together with the target’s FA image. Only skeleton segments from the main cingulum tract were included in the left and right cingulum ROIs, which included 712 and 799 voxels, respectively. The uncinate fasciculus ROIs included the central body of the uncinate fasciculus excluding segments extending towards the frontal pole, inferior frontal gyrus and the temporal pole. Left and right uncinate fasciculi ROIs included 477 and 478 voxels, respectively. The ROIs are displayed in Fig. 1. Mean FA, AD and RD were extracted from each ROI and the whole skeleton and summarized in Table 4.

ROIs in the cingulum (red) and uncinate fasciculus (blue) depicted on the tract-based spatial statistics (TBSS) skeleton (green) overlaid on the group mean fractional anisotropy (FA) map. Axial (Z), coronal (Y) and sagittal (X) views of the ROIs are shown with the corresponding MNI coordinates.
Statistical analyses
Statistical analyses were done using SPSS 25 (IBM Statistics). A two-tailed p value <0.05 was considered significant in all analyses. The Shapiro–Wilk test was used to test for non-normal distributions of continuous variables. Significantly non-normally distributed variables were normalized using Rankit transformation. Significantly non-normally distributed variables are displayed in Tables 1, 3 and 4 with medians and quartiles. Group differences in sex distribution were tested with χ2 tests and continuous matching variables and control variables with two-tailed t tests.
Test of hypothesis
We hypothesized that patients would differ from controls in FA of the left relative to the right uncinate fasciculus and cingulum bundle. Our hypotheses were tested with repeated-measures analysis of covariance (ANCOVA) in separate models for uncinate fasciculus and cingulum, respectively. The left and right ROIs were included as within-subject variables with group as between-subject factor, controlled for age, sex and whole skeleton FA. The contrast of main interest was the group-by-hemisphere interaction. In subsequent analyses, sex was modelled as a between-subject variable to test for group-by-sex-by-hemisphere interactions, since earlier studies in children reported sex-dependent associations between previous exposure to increased cortisol levels and fronto-limbic morphology and neural activity.10,40
Planned follow-up analyses
Contingent on significant effects in the primary models, several planned follow-up analyses were conducted. First, we examined the contribution of left and right fronto-limbic fibre tract FA using one-way ANCOVA models predicting either left or right fibre tract FA with group, controlling for age, sex and whole skeleton FA. Second, we tested whether significant group differences in fronto-limbic fibre tract FA asymmetry persisted when additional controlling for potential confounding variables, including parental education, VCI score, SLE lifetime, Tanner stage, CAR and daily cortisol output. Third, we used repeated-measures ANCOVA to examine group differences in fibre tract asymmetry of AD and RD because higher FA could be linked to lower RD and/or higher AD. Fourth, using repeated-measures ANCOVA, we examined whether the nephrotic and rheumatic patient subgroups significantly differed from each other and from the control group in fibre tract FA asymmetry, controlling for age, sex and whole skeleton FA.
Glucocorticoid dose–response relationships
Repeated-measures ANCOVA, within patients, tested for possible dose–response relationships between previous glucocorticoid treatment measures and the fronto-limbic fibre tract microstructure asymmetries that significantly differed between controls and patients. Three separate models tested for interactions between, respectively, cumulative glucocorticoid dose, median daily glucocorticoid dose or mean daily glucocorticoid and hemisphere (left and right fibre tract FA), controlling for age, sex, whole skeleton FA and time since treatment to adjust for inter-individual variations in the time elapsed since the end of glucocorticoid treatment. Models examining effects of median or mean daily glucocorticoid dose were additionally controlled for treatment duration. In case of significant interaction effects, we tested if observed effects remained when additionally controlling for parental education, VCI score, SLE lifetime, pubertal development, CAR and daily cortisol output.
Results
Demographic and control measures
Patients and controls did not significantly differ in age, sex, handedness, parental education, Tanner stage or whole skeleton FA (p > 0.26). Consistent with our previous findings in a larger cohort,26 patients had significantly lower VCI scores (t(54) = −3.926, p < 0.001) and higher number of SLE (t(52) = −2.342, p = 0.024) relative to controls. When two of the 20 questions that assessed disease-related stress were excluded, group difference disappeared (p = 0.85). We did not observe significantly higher CAR in female patients relative to female controls (p = 0.16) or increased daily cortisol output in male patients compared to male controls (p = 0.06), as we recently observed in the larger cohort.29 Moreover, the nephrotic and rheumatic subgroups did not differ significantly from each other (p > 0.05) on any of the matching or control variables displayed in Table 1.
Glucocorticoid treatment variables in patients
Children with nephrotic syndrome received higher glucocorticoid doses than children with rheumatic disease, while the two disease subgroups did not differ on the remaining treatment variables shown in Table 3.
Group differences in fronto-limbic fibre tract FA
Our hypothesis was confirmed as the ANCOVA showed a significant interaction between group and hemisphere (F(1,51) = 5.239, p = 0.026; ηp2 = 0.093, Fig. 2a, d). Healthy controls appeared to have lower FA in left relative to right uncinate fasciculus, whereas patients did not display any hemispheric asymmetry. Instead, patients had higher left and similar right uncinate fasciculus FA as compared to controls. We did not observe a main effect of group, or group-by-sex or group-by-sex-by-hemisphere interaction for uncinate fasciculi FA (p ≥ 0.25). We did not observe a significant group-by-hemisphere interaction for cingulum FA (p = 0.3), nor a significant main effect of group or group-by-sex or group-by-sex-by-hemisphere interaction (p ≥ 0.16).

The line plots in the top row show the estimated marginal means and 95% confidence interval for the group-by-hemisphere interaction in the left and right uncinate fasciculi for a fractional anisotropy (FA), b axial diffusivity (AD) and c radial diffusivity (RD) based on the repeated-measures ANCOVA. The scatter plots in the bottom row display the predicted values for the group-by-hemisphere interaction in the left and right uncinate fasciculi for d FA, e AD and f RD based on the repeated-measures ANCOVA. The mean for each group is represented with a horizontal line in the scatter plots (d–f).
Planned follow-up analyses
Compared to controls, patients displayed higher, although not statistically significant, left uncinate fasciculus FA (p = 0.059), while groups did not differ in right uncinate fasciculus FA (p = 0.85). Moreover, the observed group-by-hemisphere interaction for uncinate fasciculus FA persisted (F(1,40)=4.930, p = 0.032, ηp2 = 0.110), when further controlling for parental education, handedness, VCI score, SLE, pubertal development, CAR and daily cortisol output.
We observed a significant group-by-hemisphere interaction effect for uncinate fasciculus AD (F(1,51) = 4.766, p = 0.034, ηp2 = 0.085; Fig. 2b, e) with patients having higher AD in the left relative to right uncinate fasciculus, whereas controls did not show hemispheric asymmetry in uncinate fasciculus AD. We did not observe a group-by-hemisphere effect for RD (p = 0.12; Fig. 2c, f). No main effects for group were observed for AD or RD (p ≥ 0.13). Post hoc one-way ANCOVA analyses showed that patients had significantly higher left uncinate fasciculus AD compared to controls F(1,51) = 4.399, p = 0.041, ηp2 = 0.079) but comparable right uncinate fasciculus AD (p = 0.64). Moreover, the observed group-by-hemisphere interaction effect for AD largely persisted (F(1,40) = 3.707, p = 0.061, ηp2 = 0.085) when simultaneously controlling for parental education, handedness, VCI score, SLE lifetime, pubertal development, CAR and daily cortisol output.
Nephrotic and rheumatic patients did not significantly differ in uncinate fasciculus FA asymmetry or average uncinate fasciculi FA (p ≥ 0.55). Furthermore, nephrotic patients differed significantly from controls in uncinate fasciculus FA asymmetry, and did not display any apparent asymmetry, while controls had lower left relative to right uncinate fasciculus FA (group-by-hemisphere interaction: F(1,34) = 5.614, p = 0.024, ηp2 = 0.142). We observed a similar group-by-hemisphere interaction for rheumatic patients, but this effect did not reach statistical significance (F(1,40) = 2.247, p = 0.142, ηp2 = 0.053). Finally, we did not observe any significant main effects of group for either nephrotic or rheumatic patients (p ≥ 0.33).
Glucocorticoid dose–response associations with uncinate fasciculi FA and diffusivities
Cumulative glucocorticoid dose was not significantly associated with left-right differences in uncinate fasciculi FA (p = 0.24). However, we observed a significant positive relationship between cumulative glucocorticoid dose and bilateral uncinate fasciculi FA (F(1,22) = 5.527; p = 0.028, ηp2 = 0.201; Fig. 3a). This effect largely remained (F(1,13) = 3.825; p = 0.072, ηp2 = 0.227) when additionally controlling for parental education, handedness, VCI score, SLE lifetime, pubertal development, CAR and daily cortisol output. We did not observe any significant dose-by-hemisphere interaction or main effects for mean daily glucocorticoid dose or median daily glucocorticoid dose (p ≥ 0.22).

Partial regression plots of a fractional anisotropy (FA) and b axial diffusivity (AD) in the bilateral uncinate fasciculus as a function of cumulative weight-adjusted glucocorticoid dose in patients. The bold straight lines represent the linear fits between cumulative glucocorticoid dose and uncinate fasciculus FA or AD, corrected for age, sex, whole skeleton FA or AD and time since treatment. The dotted lines correspond to the 95% confidence interval of the group mean. Note that the values displayed on the Y- and X-axis are the model residuals.
Finally, we examined if cumulative glucocorticoid dose was associated with uncinate fasciculus AD, since AD appeared to mediate the observed group-by-hemisphere interaction effect in FA. As for uncinate FA, we did not observe a significant cumulative glucocorticoid dose-by-hemisphere interaction effect (p = 0.59). However, higher cumulative glucocorticoid dose was significantly associated with higher bilateral uncinate fasciculi AD (F(1,22) = 6.859; p = 0.016, ηp2 = 0.238, Fig. 3b). This association remained significant (F(1,13) = 11.479; p = 0.005, ηp2 = 0.469) when controlling for parental education, handedness, VCI score, SLE lifetime, pubertal development, CAR and daily cortisol output.
Effect-size maps
To provide further information about possible differences between patients and controls in FA and cumulative dose–response associations with FA within patients across the white matter skeleton, two effect-size maps are presented in the supplementary material. The unthresholded t-maps have been uploaded to NeuroVault.org41 available at https://neurovault.org/collections/8377/.
Discussion
The present study is, to the best of our knowledge, the first to report on associations between white matter microstructure and glucocorticoid treatment in preschool and school-aged children due to non-cerebral diseases. Children and adolescents previously treated with synthetic glucocorticoids did not show hemispheric asymmetry in uncinate fasciculus FA as seen in healthy controls, who displayed lower FA in the left relative to the right uncinate fasciculus. This difference in hemispheric asymmetry was mainly driven by patients having higher FA and higher AD in left uncinate fasciculus relative to controls, with no apparent differences in right uncinate fasciculus. Notably, in patients we observed a linear dose–response relationship with higher cumulative glucocorticoid dose being associated with higher bilateral uncinate fasciculi FA and AD. These associations persisted when controlling for mean FA and AD in the whole skeleton, which suggests that the observed effects are specific to uncinate fasciculi and are not linked to global microstructural differences in cerebral white matter. Moreover, the observed associations remained significant after controlling for present daily cortisol output and CAR, which indicates that variability in present endogenous cortisol levels did not mediate our findings.
The sparsity of neuroimaging studies investigating the effects of previous glucocorticoid treatment during the preschool- and school-aged years makes it difficult to assess the validity and significance of our findings. In the present study, children and adolescents previously treated with glucocorticoids displayed reduced hemispheric asymmetry in uncinate fasciculus FA as well as higher FA and AD in left uncinate fasciculus relative to controls. Our results are almost mirrored by a previous study that observed a positive linear relationship between increased CAR and higher left relative to right uncinate fasciculus FA in healthy adults.20 However, in Madsen et al.,19 the differences in asymmetry were mainly driven by RD, with no significant difference in AD, whereas in the current study, the differences were mainly caused by AD, but with no apparent differences in RD. This discrepancy in diffusivity between studies might be related to the different age ranges that were examined. In the current study, we investigated children in the age range of 7–16 years, in which RD and to a lesser degree AD decrease with age,42 whereas Madsen et al.19 included healthy adults in the age range of 19–86 years, where only minor age-related increases in AD and RD occur.42 Thus, it might be that superimposed maturational changes mask or change the effects of glucocorticoids on the uncinate fasciculus microstructure. In addition, various lines of cross-species evidence suggest that left fronto-limbic brain regions are more vulnerable to increased levels of stress and glucocorticoids than the corresponding brain structures in the right hemisphere,15,16 supporting our findings of group differences in the left uncinate fasciculus. Furthermore, higher cortisol reactivity has been linked to differences in hemispheric asymmetry in monkeys. Monkeys with low cortisol reactivity had larger right relative to left grey matter volume, whereas monkeys with high cortisol reactivity displayed an absence in hemispheric asymmetry.43 While our findings align well with the available literature, it is not possible to disentangle whether our findings are mediated by the effects of glucocorticoid treatment, increased stress associated with the previous illness or to disease-specific mechanisms. However, we did not observe any significant differences in uncinate fasciculus microstructure asymmetry between the two patient groups, and the observed group differences between patients and controls were largest in the nephrotic patients who received the highest glucocorticoid doses. Moreover, although we are not aware of the existence of studies that have compared rheumatic to nephrotic patients on measures of pain and distress related to the disease, rheumatic patients arguably experience more pain than children with nephrotic syndrome.24,25 Furthermore, in case of disease-specific effects, we would not have expected to observe a linear association between cumulative glucocorticoid dose and microstructure in the uncinate fasciculi across the entire patient cohort. Given the above, we think it is unlikely that the observed group differences in uncinate fasciculus microstructure were mediated by disease-specific effects. Nevertheless, future prospective studies are needed to disentangle the effects of glucocorticoid treatment from potential disease-specific effects.
We observed a dose–response effect with higher exogenous cumulative glucocorticoid doses being associated with higher FA and AD in the bilateral uncinate fasciculi in patients. Previous neuroimaging studies have linked higher endogenous cortisol levels to lower FA in the uncinate fasciculi.44,45 Adult patients with a history of chronic elevated endogenous cortisol levels due to Cushing’s disease displayed lower FA in multiple fibre tracts including the bilateral uncinate fasciculi.44,45 Because these studies differ from each other, and with the present study, in experimental set-up, study population and/or examined age range, it is unclear whether the apparent inconsistencies in the directional relationship between glucocorticoid levels and FA are mediated by different neuroendocrinological events and/or study design. Notably, one study in adult rats observed higher FA in multiple white matter tracts after being exposed to repeated inescapable stress for two weeks,46 suggesting that chronic stress and potentially long-term increases in circulating glucocorticoids may also trigger cellular events associated with increased FA. Because maturation of the uncinate fasciculi during childhood and adolescence is characterized by increases in FA,23,47 it is possible that the higher FA in our patients is caused by accelerated fronto-limbic fibre tract maturation. However, increases in FA associated with white matter maturation are typically driven by decreases in RD, with no changes or only minor decreases in AD.23,47 In contrast, higher FA values in the present study appeared to be driven primarily by increased AD rather than decreased RD. Therefore, we think it is unlikely that our findings reflect accelerated maturation in children exposed to synthetic glucocorticoid treatment. Another possibility is that high levels of glucocorticoids may affect the white matter differently depending on the age of exposure. This point is illustrated by a recent neuroimaging study in adult men that examined the relationship between exposure to stress at different developmental periods and white matter myelination, indexed by magnetization transfer ratio (MTR) and myelin water fraction. Adult men of mothers, who reported a higher incidence of SLEs during pregnancy, had lower MTR and myelin water fraction in the genu and/or splenium of the corpus callosum, whereas increased exposure to SLEs during childhood and adolescents were associated with higher MTR in the genu or splenium.48 Clearly, more studies are needed to clarify whether exposure to increased levels of glucocorticoids affect the white matter differently depending on the developmental period in life.
Our study is limited by the relatively small sample size, particular for the male group. Thus, future studies are needed to confirm our results. Moreover, because of the cross-sectional study design, we cannot infer causality of the previous glucocorticoid treatment, nor possible disease-related mechanisms. Furthermore, since we examined children and adolescents with chronic non-cerebral diseases, we cannot exclude the possibility that the reported group differences in uncinate fasciculus microstructure asymmetry are secondary to increased stress, pain, discomfort, hospitalization or decreased immune function associated with the patients’ disease. It would have been optimal to include a control group with a similar disease history as the nephrotic and/or rheumatic patients, who had not received glucocorticoid treatment. However, such a control group could not be identified due to differences in disease mechanisms, course of illness, disease severity and treatment. Therefore, we included two different non-cerebral disease groups, with substantially different pathology, as we reasoned that effects common to both groups as well as dose–response associations would likely reflect effects of glucocorticoid treatment more than disease-specific effects.
In conclusion, we observed that children and adolescents previously treated with glucocorticoids for non-cerebral diseases lacked the typical right–left asymmetry due to higher FA and AD in the left uncinate fasciculus relative to healthy controls. Notably, patients displayed a significant dose–response relationship with higher cumulative glucocorticoid doses being associated with higher bilateral uncinate fasciculi FA and AD. The present study provides novel results that glucocorticoid treatment in the children may trigger long-term differences in the microstructure of the uncinate fasciculi. However, future studies including larger cohorts and preferably prospective in design are needed to infer causality as well as disentangle the effects of glucocorticoid treatment and disease-specific mechanisms.
Change history
09 February 2022
A Correction to this paper has been published: https://doi.org/10.1038/s41390-021-01736-8
References
Coutinho, A. E. & Chapman, K. E. The anti-inflammatory and immunosuppressive effects of glucocorticoids, recent developments and mechanistic insights. Mol. Cell Endocrinol. 335, 2–13 (2011).
Damsted, S. K., Born, A. P., Paulson, O. B. & Uldall, P. Exogenous glucocorticoids and adverse cerebral effects in children. Eur. J. Paediatr. Neurol. 15, 465–477 (2011).
de Kloet, E. R., Joels, M. & Holsboer, F. Stress and the brain: from adaptation to disease. Nat. Rev. Neurosci. 6, 463–475 (2005).
Gray, J. D., Kogan, J. F., Marrocco, J. & McEwen, B. S. Genomic and epigenomic mechanisms of glucocorticoids in the brain. Nat. Rev. Endocrinol. 13, 661–673 (2017).
de Kloet, E. R. et al. Brain mineralocorticoid receptors and centrally regulated functions. Kidney Int. 57, 1329–1336 (2000).
Harris, A. & Seckl, J. Glucocorticoids, prenatal stress and the programming of disease. Hormones Behav. 59, 279–289 (2011).
Jernigan, T. L., Baare, W. F., Stiles, J. & Madsen, K. S. Postnatal brain development: structural imaging of dynamic neurodevelopmental processes. Prog. Brain Res. 189, 77–92 (2011).
Graham, A. M. et al. Maternal cortisol concentrations during pregnancy and sex-specific associations with neonatal amygdala connectivity and emerging internalizing behaviors. Biol. Psychiatry 85, 172–181 (2019).
Scheinost, D., Spann, M. N., McDonough, L., Peterson, B. S. & Monk, C. Associations between different dimensions of prenatal distress, neonatal hippocampal connectivity, and infant memory. Neuropsychopharmacology 45, 1272–1279 (2020).
Burghy, C. A. et al. Developmental pathways to amygdala-prefrontal function and internalizing symptoms in adolescence. Nat. Neurosci. 15, 1736–1741 (2012).
Gee, D. G. et al. Early developmental emergence of human amygdala-prefrontal connectivity after maternal deprivation. Proc. Natl Acad. Sci. USA 110, 15638–15643 (2013).
Carrion, V. G., Weems, C. F., Richert, K., Hoffman, B. C. & Reiss, A. L. Decreased prefrontal cortical volume associated with increased bedtime cortisol in traumatized youth. Biol. Psychiatry 68, 491–493 (2010).
Carrion, V. G., Weems, C. F. & Reiss, A. L. Stress predicts brain changes in children: a pilot longitudinal study on youth stress, posttraumatic stress disorder, and the hippocampus. Pediatrics 119, 509–516 (2007).
Davis, E. P., Sandman, C. A., Buss, C., Wing, D. A. & Head, K. Fetal glucocorticoid exposure is associated with preadolescent brain development. Biol. Psychiatry 74, 647–655 (2013).
Ocklenburg, S., Korte, S. M., Peterburs, J., Wolf, O. T. & Gunturkun, O. Stress and laterality - the comparative perspective. Physiol. Behav. 164, 321–329 (2016).
Cerqueira, J. J., Almeida, O. F. & Sousa, N. The stressed prefrontal cortex. Left? Right! Brain Behav. Immun. 22, 630–638 (2008).
Cerqueira, J. J. et al. Corticosteroid status influences the volume of the rat cingulate cortex - a magnetic resonance imaging study. J. Psychiatr. Res. 39, 451–460 (2005).
Czeh, B. et al. Chronic social stress inhibits cell proliferation in the adult medial prefrontal cortex: hemispheric asymmetry and reversal by fluoxetine treatment. Neuropsychopharmacology 32, 1490–1503 (2007).
Madsen, K. S. et al. Hypothalamic-pituitary-adrenal axis tonus is associated with hippocampal microstructural asymmetry. Neuroimage 63, 95–103 (2012).
Madsen, K. S. et al. Cortisol awakening response and negative emotionality linked to asymmetry in major limbic fibre bundle architecture. Psychiatry Res. 201, 63–72 (2012).
Beaulieu, C. in Diffusion MRI: From Quantitative Measurement to In-Vivo Neuroantomy (eds Johansen-Berg, H. & Behrens, T. E. J.) 105–126 (Elsevier, 2009).
Schmahmann, J. D. et al. Association fibre pathways of the brain: parallel observations from diffusion spectrum imaging and autoradiography. Brain 130, 630–653 (2007).
Lebel, C. & Beaulieu, C. Longitudinal development of human brain wiring continues from childhood into adulthood. J. Neurosci. 31, 10937–10947 (2011).
Eddy, A. A. & Symons, J. M. Nephrotic syndrome in childhood. Lancet 362, 629–639 (2003).
Ravelli, A. & Martini, A. Juvenile idiopathic arthritis. Lancet 369, 767–778 (2007).
Holm, S. K. et al. Children and adolescents previously treated with glucocorticoids display lower verbal intellectual abilities. Acta Paediatr. 104, 784–791 (2015).
Holm, S. K. et al. Total brain, cortical, and white matter volumes in children previously treated with glucocorticoids. Pediatr. Res. 83, 804–812 (2018).
Holm, S. K. et al. Previous glucocorticoid treatment in childhood and adolescence is associated with long-term differences in subcortical grey matter volume and microstructure. Neuroimage Clin. 23, 101825 (2019).
Vestergaard, M. et al. Glucocorticoid treatment earlier in childhood and adolescence show dose-response associations with diurnal cortisol levels. Dev. Psychobiol. 59, 1010–1020 (2017).
Reese, T. G., Heid, O., Weisskoff, R. M. & Wedeen, V. J. Reduction of eddy-current-induced distortion in diffusion MRI using a twice-refocused spin echo. Magn. Reson. Med. 49, 177–182 (2003).
Jovicich, J. et al. Reliability in multi-site structural MRI studies: effects of gradient non-linearity correction on phantom and human data. Neuroimage 30, 436–443 (2006).
Andersson, J. L. R., Hutton, C., Ashburner, J., Turner, R. & Friston, K. Modeling geometric deformations in EPI time series. Neuroimage 13, 903–919 (2001).
Smith, S. M. Fast robust automated brain extraction. Hum. Brain Mapp. 17, 143–155 (2002).
Jones, D. K. & Basser, P. J. “Squashing peanuts and smashing pumpkins”: how noise distorts diffusion-weighted MR data. Magn. Reson. Med. 52, 979–993 (2004).
Cook, P. A. et al. Camino: open-source diffusion-MRI reconstruction and processing. In 14th Scientific Meeting of the International Society for Magnetic Resonance in Medicine, Seattle, WA, USA, p. 2759 (2006).
Smith, S. M. et al. Tract-based spatial statistics: voxelwise analysis of multi-subject diffusion data. Neuroimage 31, 1487–1505 (2006).
Andersson, L. L. R., Jenkinson, M. & Smith, S. Non-linear Registration, aka Spatial Normalisation. FMRIB technical report no. TR07JA2 (FMRIB Centre, 2007).
Mori, S., Wakana, S., Nagae-Poetscher L. M. & Van Zijl, P.C.M. MRI Atlas of Human White Matter 1st edn (Elsevier, 2005).
Hua, K. et al. Tract probability maps in stereotaxic spaces: analyses of white matter anatomy and tract-specific quantification. Neuroimage 39, 336–347 (2008).
Buss, C. et al. Maternal cortisol over the course of pregnancy and subsequent child amygdala and hippocampus volumes and affective problems. Proc. Natl Acad. Sci. USA 109, E1312–1319 (2012).
Gorgolewski, K. J. et al. NeuroVault.org: a web-based repository for collecting and sharing unthresholded statistical maps of the human brain. Front. Neuroinform. 9, 8 (2015).
Lebel, C. et al. Diffusion tensor imaging of white matter tract evolution over the lifespan. Neuroimage 60, 340–352 (2012).
Short, S. J. et al. Population variation in neuroendocrine activity is associated with behavioral inhibition and hemispheric brain structure in young rhesus monkeys. Psychoneuroendocrinology 47, 56–67 (2014).
van der Werff, S. J. et al. Widespread reductions of white matter integrity in patients with long-term remission of Cushing’s disease. Neuroimage Clin. 4, 659–667 (2014).
Pires, P. et al. White matter alterations in the brains of patients with active, remitted, and cured cushing syndrome: a DTI study. Am. J. Neuroradiol. 36, 1043–1048 (2015).
Magalhaes, R. et al. White matter changes in microstructure associated with a maladaptive response to stress in rats. Transl. Psychiatry 7, e1009 (2017).
Lebel, C., Walker, L., Leemans, A., Phillips, L. & Beaulieu, C. Microstructural maturation of the human brain from childhood to adulthood. Neuroimage 40, 1044–1055 (2008).
Jensen, S. K. G. et al. Associations between prenatal, childhood, and adolescent stress and variations in white-matter properties in young men. Neuroimage 182, 389–397 (2018).
Acknowledgements
The work was funded by the Danish Council for Independent Research (grant no.r: 09-071546), Gangstedfonden, Ville Heises Legat, Hvidovre Hospital’s Research Fund and the Lundbeck Foundation, and the Centre of Excellence grant to The Centre for Integrated Molecular Brain Imaging. H.R.S. holds a 5-year professorship in precision medicine at the Faculty of Health Sciences and Medicine, University of Copenhagen, which is sponsored by the Lundbeck Foundation (grant no. R186-2015-2138).
Author information
Authors and Affiliations
Contributions
Conceived and designed the study: M.V., W.F.C.B., S.K.H., O.B.P., A.P.B., P.U., H.R.S. and K.S.M. Performed the experiments: M.V. and S.K.H. Evaluated the data: M.V., W.F.C.B., S.K.H., C.G.M. and K.S.M. Analysed the data: M.V., W.F.C.B. and K.S.M. Contributed to writing the paper: M.V., W.F.C.B., S.K.H., O.B.P., A.P.B., P.U., H.R.S. and K.S.M.
Corresponding author
Ethics declarations
Competing interests
H.R.S. has received honoraria as speaker from Sanofi Genzyme, Denmark and Novartis, Denmark, as consultant from Sanofi Genzyme, Denmark and as senior editor (NeuroImage) from Elsevier Publishers, Amsterdam, The Netherlands. He has received royalties as book editor from Springer Publishers, Stuttgart, Germany. The other authors reported no competing interests.
Patient consent
Participants and their parents received thorough information regarding the project and written consent was obtained from all parents before study initiation. The study was approved by the Committee on Biomedical Research Ethics for the Capital Region of Denmark (protocol no. H-KF-01-131/03) and was conducted in accordance with the Declaration of Helsinki.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original online version of this article was revised: Figure 3 has been corrected.
Supplementary information
Rights and permissions
About this article

Cite this article
Vestergaard, M., Baaré, W.F.C., Holm, S.K. et al. Glucocorticoid treatment for non-cerebral diseases in children and adolescents is associated with differences in uncinate fasciculus microstructure. Pediatr Res 91, 879–887 (2022). https://doi.org/10.1038/s41390-021-01394-w
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41390-021-01394-w

{kind=link}
{kind=link}