
Abstract
Objective
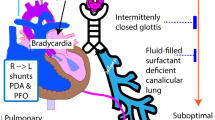
To study cardiovascular response to minimally invasive surfactant therapy in preterm infants with and without foetal growth restriction (FGR).
Design
Poractant alfa was administered and echocardiograms were performed before and 30 min after. FGR infants were compared with those appropriate for gestational age (AGA).
Results
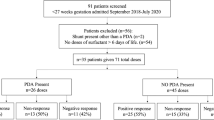
Ten FGR infants were compared with 20 AGA infants (gestation [weeks], 28.9 ± 2 vs. 28.6 ± 1, p = 0.55 and birthweight [g], 813 ± 157 vs. 1141 ± 257, p = 0.01, respectively). The change in echocardiographic parameters was more prominent in AGA infants ([global contractility] fractional area change [FAC, %], FGR, 24.7 ± 2.2 to 27.9 ± 0.4, p = 0.08 vs. AGA, 26.6 ± 3 to 30.5 ± 1, p < 0.01, and [longitudinal contractility] tricuspid annular plane systolic excursion [mm], FGR, 3.9 ± 0.3 to 4.6 ± 0.5, p = 0.003 vs. AGA, 4.6 ± 0.3 to 5.5 ± 0.4, p = 0.0001). Significant difference was noted for change in FAC (%), FGR 2.1 ± 1.7 vs. AGA 4.1 ± 1.2, p = 0.02.
Conclusions
Differential cardiovascular response to minimally invasive surfactant therapy amongst FGR infants may reflect an in-utero maladaptive state.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout

Similar content being viewed by others

References
Jobe AH. The new bronchopulmonary dysplasia. Curr Opin Pediatr. 2011;23:167–72.
Aldana-Aguirre JC, Pinto M, Featherstone RM, Kumar M. Less invasive surfactant administration versus intubation for surfactant delivery in preterm infants with respiratory distress syndrome: a systematic review and meta-analysis. Arch Dis Child Fetal Neonatal Ed. 2017;102:F17–23.
Göpel W, Kribs A, Ziegler A, Laux R, Hoehn T, Wieg C, et al. Avoidance of mechanical ventilation by surfactant treatment of spontaneously breathing preterm infants (AMV): an open-label, randomised, controlled trial. Lancet. 2011;378:1627–34.
Kanmaz HG, Erdeve O, Canpolat FE, Mutlu B, Dilmen U. Surfactant administration via thin catheter during spontaneous breathing: randomized controlled trial. Pediatrics. 2013;131:e502–9.
Kribs A, Roll C, Göpel W, Wieg C, Groneck P, Laux R, et al. Non-intubated surfactant application during CPAP-assisted spontaneous breathing versus conventional therapy in extremely preterm infants—a randomised controlled trial. JAMA Pediatr. 2015;169:723–30.
Clyman R, Jobe A, Heymann M, Ikegami M, Roman C, Payne B, et al. Increased shunt through the patent ductus arteriosus after surfactant replacement therapy. J Pediatr. 1982;100:101–7.
Sehgal A, Mak W, Dunn M, Kelly E, Redington A, Whyte H, et al. Haemodynamic changes after delivery room surfactant administration to very low birth weight infants. Arch Dis Child Fetal Neonatal Ed. 2010;95:F345–51.
Kääpä P, Seppänen M, Kero P, Saraste M. Pulmonary haemodynamics after synthetic surfactant replacement in neonatal respiratory distress syndrome. J Pediatr. 1993;123:115–9.
Sehgal A, Bhatia R, Roberts CT. Cardiorespiratory physiology following minimally invasive surfactant therapy in preterm infants. Neonatology. 2019;116:278–85.
Yzydorczyk C, Armengaud JB, Peyter AC, Chehade H, Cachat F, Juvet C, et al. Endothelial dysfunction in individuals born after fetal growth restriction: cardiovascular and renal consequences and preventive approaches. J Dev Orig Health Dis. 2017;8:448–64.
Sehgal K, Sehgal K, Tan K, Sehgal A. Impaired in-utero growth: an important risk factor for chronic lung disease [abstract]. Pediatr Acad Soc. 2019;E-PAS2019:442.
Lal MK, Manktelow BN, Draper ES, Field DJ. Chronic lung disease of prematurity and intrauterine growth retardation: a population-based study. Pediatrics. 2003;111:483–7.
Rabinovitch M, Gamble W, Nadas AS, Miettinen OS, Reid L. Rat pulmonary circulation after chronic hypoxia: hemodynamic and structural features. Am J Physiol. 1979;236:H818–27.
Ziino AJA, Ivanovska J, Belcastro R, Kantores C, Xu EZ, Lau M, et al. Effects of Rho-kinase inhibition on pulmonary hypertension, lung growth, and structure in neonatal rats chronically exposed to hypoxia. Pediatr Res. 2010;67:177–82.
Abman SH, Shanley PF, Accurso FJ. Failure of postnatal adaptation of the pulmonary circulation after chronic intrauterine pulmonary hypertension in fetal lambs. J Clin Invest. 1989;83:1849–58.
Goldberg SJ, Levy RA, Siassi B, Betten J. The effects of maternal hypoxia and hyperoxia upon the neonatal pulmonary vasculature. Pediatrics. 1971;48:528–33.
Dargaville PA, Aiyappan A, Cornelius A, Williams C, De Paoli AG. Preliminary evaluation of a new technique of minimally invasive surfactant therapy. Arch Dis Child Fetal Neonatal Ed. 2011;96:F243–8.
Hayabuchi Y, Ono A, Kagami S. Pulmonary annular motion velocity assessed using Doppler tissue imaging. Circ J. 2016;80:168–76.
Evans NJ, Archer LN. Doppler assessment of pulmonary artery pressure and extra pulmonary shunting in the acute phase of hyaline membrane disease. Arch Dis Child. 1999;66:6–11.
Howard LS, Grapsa J, Dawson D, Bellamy M, Chambers JB, Masani ND, et al. Echocardiographic assessment of pulmonary hypertension: standard operating procedure. Eur Respir Rev. 2012;21:239–48.
Milnor WR, Conti CR, Lewis KB, O’Rourke MF. Pulmonary arterial pulse wave velocity and impedance in man. Circ Res. 1969;25:637–49.
Fenton TR, Kim JH. A systematic review and meta-analysis to revise the Fenton growth chart for preterm infants. BMC Pediatr. 2013;13:59. https://doi.org/10.1186/1471-2431-13-59.
Skinner JR, Boys RJ, Hunter S, Hey EN. Pulmonary and systemic arterial pressure in hyaline membrane disease. Arch Dis Child. 1992;67:366–73.
Vitali F, Galletti S, Aceti A, Aquilano G, Fabi M, Balducci A, et al. Pilot observational study on haemodynamic changes after surfactant administration in preterm newborns with respiratory distress syndrome. Ital J Pediatr. 2014;40:26.
Pike K, Jane Pillow J, Lucas JS. Long term respiratory consequences of intrauterine growth restriction. Semin Fetal Neonatal Med. 2012;17:92–8.
Briana DD, Malamitsi-Puchner A. Small for gestational age birth weight: impact on lung structure and function. Paediatr Respir Rev. 2013;14:256–62.
Maritz GS, Morley CJ, Harding R. Early developmental origins of impaired lung structure and function. Early Hum Dev. 2005;81:763–71.
Orgeig S, Crittenden TA, Marchant C, McMillen IC, Morrison JL. Intrauterine growth restriction delays surfactant protein maturation in the sheep fetus. Am J Physiol Lung Cell Mol Physiol. 2010;298:L575–83.
Leung DY, Glagov S, Mathews MB. Elastin and collagen accumulation in rabbit ascending aorta and pulmonary trunk during postnatal growth. Correlation of cellular synthetic response with medial tension. Circ Res. 1977;41:316–23.
Giussani DA, Camm EJ, Niu Y, Richter HG, Blanco CE, Gottschalk R, et al. Developmental programming of cardiovascular dysfunction by prenatal hypoxia and oxidative stress. PLoS ONE. 2012;7:e31017.
Gien J, Seedorf GJ, Balasubramaniam V, Markham N, Abman SH. Intrauterine pulmonary hypertension impairs angiogenesis in vitro: role of vascular endothelial growth factor nitric oxide signalling. Am J Respir Crit Care Med. 2007;176:1146–53.
Grover TR, Parker TA, Markham NE, Abman SH. rhVEGF treatment preserves pulmonary vascular reactivity and structure in an experimental model of pulmonary hypertension in fetal sheep. Am J Physiol Lung Cell Mol Physiol. 2005;289:L315–21.
Rozance PJ, Seedorf GJ, Brown A, Roe G, O’Meara MC, Gien J, et al. Intrauterine growth restriction decreases pulmonary alveolar and vessel growth and causes pulmonary artery endothelial cell dysfunction in vitro in fetal sheep. Am J Physiol Lung Cell Mol Physiol. 2011;301:L860–71.
Braems GA, Yao LJ, Inchley K, Brickenden A, Han VK, Grolla A, et al. Ovine surfactant protein cDNAs: use in studies on fetal lung growth and maturation after prolonged hypoxemia. Am J Physiol Lung Cell Mol Physiol. 2000;278:L754–64.
Weinberg CE, Hertzberg JR, Ivy DD, Kirby KS, Chan KC, Valdes-Cruz L, et al. Extraction of pulmonary vascular compliance, pulmonary vascular resistance, and right ventricular work from single-pressure and Doppler flow measurements in children with pulmonary hypertension: a new method for evaluating reactivity—in vitro and clinical studies. Circulation. 2004;110:2609–17.
Sehgal A, Gwini SM, Menahem S, Allison BJ, Miller S, Polglase GR. Preterm growth restriction and bronchopulmonary dysplasia: the vascular hypothesis and related physiology. J Physiol. 2019;597:1209–20.
Hung MW, Yeung HM, Lau CF, Poon AMS, Tipoe GL, Fung ML. Melatonin attenuates pulmonary hypertension in chronically hypoxic rats. Int J Mol Sci. 2017;18:1125. https://doi.org/10.3390/ijms18061125.
Garcia JJ, López-Pingarrón L, Almeida-Souza P, Tres A, Escudero P, García-Gil FA, et al. Protective effects of melatonin in reducing oxidative stress and in preserving the fluidity of biological membranes: a review. J Pineal Res. 2014;56:225–37.
Mauriz JL, Collado PS, Veneroso C, Reiter RJ, González-Gallego J. A review of the molecular aspects of melatonin’s anti-inflammatory actions: recent insights and new perspectives. J Pineal Res. 2013;54:1–14.
Girouard H, Chulak C, Lejossec M, Lamontagne D, de Champlain J. Vasorelaxant effects of the chronic treatment with melatonin on mesenteric artery and aorta of spontaneously hypertensive rats. J Hypertens. 2001;19:1369–77.
Anwar MM, Meki AR, Rahma HH. Inhibitory effects of melatonin on vascular reactivity: possible role of vasoactive mediators. Comp Biochem Physiol C Toxicol Pharm. 2001;130:357–67.
Torres F, González-Candia A, Montt C, Ebensperger G, Chubretovic M, Serón-Ferré M, et al. Melatonin reduces oxidative stress and improves vascular function in pulmonary hypertensive newborn sheep. J Pineal Res. 2015;58:362–73.
Sehgal A, Krishnamurthy MB, Clark M, Menahem S. ACE inhibition for severe bronchopulmonary dysplasia—an approach based on physiology. Physiol Rep. 2018;6:e13821. https://doi.org/10.14814/phy2.13821.
Author information
Authors and Affiliations
Contributions
AS—conception of the study, data acquisition, analysis and interpretation. Wrote the first draft and revised critically. RB—conception of the study and the protocol for MIST. Data analysis and interpretation. Revised draft for important intellectual content. CTR—conception of the study and the protocol for MIST. Data analysis and interpretation. Revised draft for important intellectual content.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Sehgal, A., Bhatia, R. & Roberts, C.T. Cardiovascular response and sequelae after minimally invasive surfactant therapy in growth-restricted preterm infants. J Perinatol 40, 1178–1184 (2020). https://doi.org/10.1038/s41372-020-0682-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41372-020-0682-5
This article is cited by
-
Hemodynamic consequences of respiratory interventions in preterm infants
Journal of Perinatology (2022)
