
Abstract
Background:
The health effects of bisphenol A (BPA) and di-(2-ethylhexyl) phthalate (DEHP) have been studied extensively in children. The impact of other chemicals in these two classes has not been investigated as fully.
Methods:
We conducted a cross-sectional pilot study of 10–13 y old healthy children. We assessed descriptive, univariable, and multivariable associations of urinary metabolites of bisphenols and phthalates with oxidant stress, insulin resistance, body mass, and endothelial dysfunction. Possible associations with brachial artery distensibility, pulse wave velocity (markers of vascular stiffness), and serum endothelial cell-derived microparticle levels were also assessed.
Results:
We enrolled 41 participants, 12.1 ± 1.0 y, most of whom were Mexican Americans (42%) or other Hispanics (34%). Increased BPA levels were associated with increased levels of F2-isoprostane (ng/ml) (P = 0.02), with a similar trend for DEHP metabolites. Each log unit increase of high molecular weight (HMW) phthalate metabolites was associated with a 0.550 increase in Homeostatic Model Assessment of insulin resistance (HOMA-IR) units (P = 0.019) and altered circulating levels of activated endothelial cell-derived microparticles (% per ml) (P = 0.026). Bisphenol S (BPS), a replacement for BPA, was associated with increased albumin (mg):creatinine (g) ratio (P = 0.04). Metabolites of HMW phthalates were also associated with decreased brachial artery distensibility (P = 0.047).
Conclusion:
Exposure to bisphenols and phthalates, including a BPA replacement, is associated with increased oxidant stress, insulin resistance, albuminuria, as well as disturbances in vascular function in healthy children.
Similar content being viewed by others

Main
The prevalence of obesity, insulin resistance, and diabetes in children has increased substantially over the past three decades. While there are many plausible causes, including changes in diet, food marketing, perinatal exposures, decreased physical activity, and thrifty genes (1), endocrine disrupting environmental chemicals such as bisphenols and phthalates may be another factor driving this epidemic. Given that dietary intake is the chief source of exposure to bisphenols and phthalates, children and adolescents are uniquely vulnerable to these chemicals as they have greater food consumption per unit body weight and will have prolonged exposure over the course of the lifespan (2).
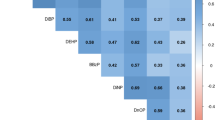
Bisphenol A (BPA) is a synthetic chemical comprised of two phenol rings connected by a methyl bridge, with two methyl groups attached to the bridge. BPA was initially designed as a synthetic estrogen. It is now widely used for its cross-linking properties in the manufacture of polycarbonate plastics and epoxy resin coatings used in food and beverage containers to prevent metal corrosion. It is present in intravenous tubing, including dialysis circuits. Incomplete polymerization and polymer degradation of BPA causes it to leach out of food and beverage containers and dental sealants (3). While ingestion of contaminated food is a major source of exposure to bisphenols, dental sealants, and thermal receipt papers represent other sources (4,5,6). Phthalates are esters of phthalic acid that can be either low-molecular weight (LMW) or high-molecular weight (HMW) ( Table 1 ). LMW phthalates, such as di-butyl phthalate (DBP), are frequently added to cosmetic products such as shampoos, perfume, aftershaves, lotions, and other personal hygiene products to preserve scent. HMW phathalates are used to soften and increase the flexibility of a wide range of consumer products such as vinyl plastics used in flooring, toys, plastic bags, food packaging, and intravenous tubing. Within the HMW category, di-2-ethylhexylphthalate (DEHP) is commonly found in plastic products used during industrial food production and packaging, and its metabolites are often considered a subcategory of phthalates (7). Since phthalates are not covalently bound, they can easily leach into their surrounding environment (8). While contaminated food is the major source of exposure to HMW phthalates, they can enter the human body through inhalation and dermal absorption (9).
Cross-sectional studies have associated BPA and phthalates with various cardio-metabolic risk factors including albuminuria, increased systolic blood pressure, increased waist circumference, and insulin resistance in children (10). While the mechanisms underlying these relationships are not completely understood, it is proposed that oxidant stress may be the pathophysiological link between environmental chemical exposures and metabolic dysregulation. Studies in adults have demonstrated an association between BPA, phthalate metabolites and increased systemic oxidant stress markers, including serum C-reactive protein and gamma glutamyltransferase and urinary malondialdehyde and 8-hydroxydeoxyguanosine (11,12). Moreover, Kim et al. observed that exposure to DEHP in the elderly population was associated with a concomitant increase in oxidative stress and insulin resistance (13). This association is corroborated by in vitro and animal studies that demonstrate BPA and DEHP metabolites increase oxidative stress by increasing the levels of reactive oxidant species, disrupting antioxidant defenses and inducing insulin resistance (14).
In light of these concerns and other adverse health effects, both BPA and DEHP were banned from use on children’s articles of care and toys. Six types of phthalates have been banned for use in children’s toys and certain child care articles (15). In addition, the FDA banned BPA from baby bottles and sippy cups in 2012. To comply with these restrictions, there is a general trend toward reformulating consumer products with newer compounds with similar chemical properties. In fact, the most recent reports from the CDC show a decline in DEHP exposures, while exposures to some other phthalates including di-isononyl phthalate and di-isodecyl phthalate have increased (16). Similarly, in the case of bisphenols, with manufacturers forced to respond to consumer concerns about the safety of BPA, Bisphenol S (BPS) has been introduced as a substitute in many plastic products. Although exposure to BPA has declined, exposure to BPS is on the rise (17). Very few studies have investigated these newer chemicals and their toxicity profiles.
In this study, we examined the relationship between exposure to bisphenols and phthalates, including the newer molecules, such as BPS, with oxidant stress, insulin resistance, and endothelial dysfunction in healthy children. Given that the endothelium is a major target for oxidant stress leading to arterial stiffness (18), we assessed the state of the vasculature by noninvasive techniques, namely, pulse wave velocity (PWV), brachial artery distensibility, and quantification of microparticles (MPs). The latter are small (<1.5 μm) vesicular fragments of endothelial cells released upon cell injury that have been associated with coronary artery disease and many of vascular risk factors (19). Our study is one of the first to examine these relationships in children.
Methods
Study Population
This was a cross-sectional pilot study that recruited healthy children between the ages of 10 and 13 y from September 2013 to June 2014 being seen in the General Pediatric Clinic at Bellevue Medical Center, New York, NY. The project was reviewed and approved by the NYU School of Medicine and Bellevue Medical Center Institutional Review Boards. The parents and participants provided informed consent and age-appropriate assent at the time of enrollment. Children were excluded from the study if they had: (i) BMI > 99% for age and gender; (ii) blood pressure > 99% for age and gender; (iii) chronic illness requiring medications, except asthma controlled by inhaled medications; or (iv) urological disorder interfering with voiding. Study visits were conducted at the NYU Center for Translational Science Institute (CTSI) at Bellevue Medical Center.
Participants were provided a polypropylene urine cup for collection and instructed to bring the first morning urine sample to the study visit. The urine specimens were aliquoted and stored in −80°C until analysis. Study visits were conducted in the early morning after patient had been fasting for at least 8 h. Each visit lasted between 2–2½ h, and included a range of procedures including brief medical history, 3-d diet and physical activity questionnaires administered to the child, anthropometric measures, blood sampling, brachial arterial distensibility, pulse wave analysis, and PWV. Dietary intake was determined by a 3-d record that was analyzed by a licensed nutritionist. The physical activity was scored by the study investigators using the International Physical Activity Questionnaire (IPAQ)- Short Form. Participants were categorized into three categories: inactive, minimally active, and highly activity.
Demographic and Anthropometric Measures
Age, gender, race/ethnicity, and socioeconomic status of children were self-reported by the parents. Age was rounded to the nearest year for the purposes of these analyses. Race/ethnicity was categorized into Mexican American, other Hispanic, Non-Hispanic Whites, Non-Hispanic Black, and other as per the NHANES. While family income information was not gathered, we assessed socioeconomic status by questioning parents about their child’s type of school, public or private and whether in school lunch status was free or paid. Participants attending public school and receiving free lunches were categorized in the low socioeconomic category. Body mass measurements were performed by the research nursing staff using the standard procedures and calibrated instruments in the clinic.
Urinary Bisphenol and Phthalate Metabolites
Twenty phthalate metabolites and eight bisphenol analogues were measured in the first morning urine sample at Wadsworth Center (Albany, NY) using high-performance liquid chromatography and tandem mass spectroscopy (HPLC-MS/MS) methods detailed elsewhere (17,20). Urinary phthalates biomarkers were grouped into LMW, HMW, and DEHP metabolites according to their use in product categories ( Table 1 ). Levels below the limit of detection were kept if a numerical value was reported but were otherwise replaced with the limit of detection divided by the square root of two.
Urine Creatinine
Urinary creatinine was analyzed at Wadsworth Center in the first morning sample, as described elsewhere (21). Briefly, the samples were diluted and analyzed using HPLC-MS/MS. The positive ion MRM transitions monitored were 114 > 44 for creatinine and 117 > 47 for creatinine-d3.
Measure of Oxidant Stress
Urinary levels of 8-OH-deoxyguanosine (8-OHdG) and 8-isoprostane as markers for oxidant stress were analyzed using DNA Damage ELISA Kits (Cell Biolabs, Atlanta, GA) and OxiSelect 8-iso-Prostaglandin F2α, respectively.
Measure of Insulin Resistance
Blood samples after fasting for at least 8 h were collected for measurement of fasting blood sugar (mg/dl) and insulin levels (uU/ml). The NYU Core labs processed the blood samples immediately after receipt of the specimens. To assess insulin resistance, we calculated Homeostatic Model Assessment of insulin resistance (HOMA-IR) using the following equation: (Fasting glucose (mmol/l) × Fasting insulin (uU/ml))/22.5 (22). A cut-off point of HOMA-IR ≥ 3.4 was used to assess insulin resistance as a categorical outcome. A recent study by Brar et al. showed that HOMA-IR cut-off value of 3.4 has the same sensitivity and specificity in screening for prediabetes as hemoglobin A1c of 5.7% (as defined by the American Diabetes Association) (23).
Microparticles
Microparticles were analyzed in the blood. Plasma (250 μl aliquots) was centrifuged at 20,000g for 2.5 h. The pellet was resuspended in Hank’s buffered saline solution containing 20 mmol/l HEPES and 5 mmol/l glucose. It was resuspended by vortexing the pellet for 1.5 min in buffer at a volume of 40% of the initial plasma volume. Microparticles may be distinguished based upon protein, lipid, and cholesterol composition. Multicolor fluorescence-activated cell sorting was performed to characterize the cellular source and activation state of the microparticles. An aliquot of microparticles was stained with antibodies to CD41a (Novus Biologicals) and CD31 (BD Biosciences) to identify whether they originated from platelets (cD41a+, CD31+) or endothelial cells (CD41a−CD31+). One micrometer beads (Molecular Probes) were used to gate the particles based on size. The number of microparticles from each cell type (platelet or endothelial) was measured in a 250 μl plasma sample. We measured CD62E levels (anti-E-selectin, Novus Biologicals) on the surface of the endothelial cell microparticles as an indicator of whether the cells that released the particles were activated.
Markers of Blood Pressure and Vascular Function
The DynaPulse Pathway (PulseMetric, San Diego, CA) instrument was used to obtain measurements of systolic blood pressure, diastolic blood pressure, heart rate, pulse pressure, and brachial artery distensibility. The latter was derived from arterial pressure signals obtained from a standard cuff sphygmomanometer (24). The pressure waveform is calibrated and incorporated into a physical model of the cardiovascular system, assuming a straight tube brachial artery and T-tube aortic system. DynaPulse has been previously validated with high correlation between compliance measurements obtained during cardiac catheterization and noninvasive brachial methods (r = 0.83) (24). Reproducibility studies using blind duplicates demonstrated good intraclass correlation coefficients for arterial compliance, from which distensibility is calculated (0.72) (25). All measurements were averaged. Calculation of systolic and diastolic blood pressure Z-scores utilized mixed-effects linear regression models described in The Fourth Report on the Diagnosis, Evaluation, and Treatment of High Blood Pressure in Children and Adolescents. Height Z-scores, gender, and age were input to compute expected systolic and diastolic blood pressures (derived from 1999–2000 NHANES data), and blood pressure Z-scores were then calculated from the measured values using the formula Zbp = (x −µ) / σ, where x is the measured blood pressure, µ is the expected blood pressure, and σ is derived from the National Health and Nutrition Examination Survey (NHANES) data (26). We categorized blood pressure outcomes as present or absent prehypertension (BP ≥ 90th percentile for age/height z-score/sex).
PWV, a noninvasive marker of arterial stiffness, was measured with a SphygmoCor SCOR-PVx System (Atcor Medical, Sydney, Australia). The average of three measures of PWV was used in analyses. Electrocardiogram leads are applied and then the distance from the carotid to the sternal notch to the distal artery of interest (femoral, radial, and dorsalis pedis) is entered into the software. A pressure tonometer, the size of a pencil is placed on the proximal artery (carotid) then the distal artery, the femoral artery in this study, to obtain arterial waveforms gated to the R-wave on the ECG tracing. PWV is the difference in the carotid-to-distal path length divided by the difference in R-wave-to-waveform foot times (m/s). Repeat measures in our laboratory showed excellent reproducibility with coefficients of variability <7% (27).
Statistical Analysis
We conducted univariable and multivariable analyses using Stata 12.0 (College Station, TX). Urinary metabolite concentrations were log-transformed to account for skew in the distribution of urinary phthalates. We performed univariable regressions of logs of the micromolar concentrations of metabolite groups against markers of oxidant stress, endothelial dysfunction markers (microparticles), insulin resistance, and arterial stiffness (brachial artery distensibility and PWV). We used multivariable linear regression analysis to model continuous dependent variables and logistic regression to model dichotomous variables in separate models. We adjusted all multivariable models for urinary creatinine, for BMI category, demographic characteristics (age and sex) and lifestyle characteristics (measures of caloric intake and physical activity).
Results
A total of 43 participants enrolled in the study. Two participants were excluded because they were taking medications to treat a chronic illness (attention deficit disorder), resulting in a sample size of 41 children. The blood sample for one participant was lost in transit to the laboratory but the participant was retained in the study because all other measurements were completed. Fifty-four percent of the children were female, mean age was 12.1 ± 1.0 y, and the majority identified as Mexican American or other Hispanics ( Table 2 ).
The concentrations of the environmental chemicals in the study population are summarized in Table 3 . Table 4 reports the results of univariable regression analyses of oxidant stress markers, insulin resistance, and endothelial dysfunction markers against potential confounders. Female sex was associated with increased levels of 8-OHdG (42.5 ng/ml, P = 0.038, confidence interval (CI) 2.4, 82.5), whereas low socioeconomic status showed an association with decreased levels of 8-OHdG (−57.3 ng/ml, P = 0.031, CI −109.1, −5.4). With respect to race/ethnicity, Non-Hispanic Whites showed increased levels of 8-OHdG (100.1 ng/ml, P < 0.001, CI 47.9, 152.2), whereas other Hispanics showed increase in the levels of the endothelial-derived microparticles, CD144 + 63e+ (0.2% increase per ml, P = 0.009, CI 0.6, 0.4). Being overweight was associated with increased levels of F2-isoprostane (12.4 ng/ml, P = 0.010, CI 3.1, 21.8). Participants in the other Hispanic category had lower HOMA-IR (−0.5 units, P = 0.015, CI −0.9, −0.1) ( Table 4 ). Obesity was also associated with higher HOMA-IR (−0.7 units, P = 0.003, CI 0.2, 1.1).
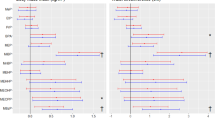
Multivariable linear regression analysis showed that each log unit increase in BPA concentration was associated with higher levels of F2-isoprostane while controlling for confounding factors (P = 0.02, CI 1.819, 19.86) ( Table 5 ). A similar association was detected for each log unit increase of DEHP metabolites, although this did not reach statistical significance (P = 0.051).
Mean levels of fasting glucose, insulin and HOMA-IR were 81.1 mg/dl, 10.2 μIU/ml, and 2.07 respectively. Eight patients had HOMA-IR > 3.4 and were categorized as insulin resistant. Linear regressions examining HOMA-IR as a continuous variable showed a positive association between each log unit increase of HMW metabolites and HOMA-IR (P = 0.010). In multivariable models, which controlled for age, sex, BMI-z score (except when the outcome examined was BMI), daily caloric intake and physical activity, each log unit increase of HMW phthalates was associated with an increased likelihood of being overweight (P = 0.028) and having a higher BMI (P = 0.041) ( Table 6 ). In addition, for each log unit increase in HMW phthalate metabolite levels, we observed a 0.050 increase in HOMA-IR (P = 0.019) ( Table 6 ). Bisphenols were not associated with body weight or insulin resistance. No significant associations were detected between bisphenol or phthalate exposure and blood pressure.
The mean level of microalbuminuria in the sample was 0.97 ± 1.96 mg/g creatinine and the value was below 10 mg/g in all participants. Other than a significant relationship between BPS exposure and albumin:creatinine ratio (P = 0.040, CI: 0.18, 7.32) ( Table 6 ), there was no association between exposure to any of the environmental chemicals and albuminuria whether considered as a continuous or categorical variable.
With respect to circulating plasma levels of activated endothelial cell-derived microparticles, each log unit increase of BPS and metabolites of HMW phthalates was associated with decreased levels of the endothelial microparticle CD 144 + 63e+, expressed as a percentage of total microparticles per ml (P = 0.021 and P = 0.026, respectively) ( Table 6 ).
With the exception of DEHP metabolites, which were associated with decreased brachial artery distensibility (P = 0.047, CI: −1.475, −0.010), multivariable regressions indicated that there were no relevant associations between the degree of exposure to any of the other environmental chemicals and brachial artery distensibility or PWV ( Table 6 ).
Discussion
In this pilot study, we have assessed exposure to a broad range of bisphenols and phthalates in a cohort of healthy, preadolescent children living in the metropolitan New York City area. We have confirmed that these molecules are associated with alterations in body weight, insulin resistance, albuminuria, markers of vascular structure and function, and indices of oxidant stress. These findings expand on prior cross sectional data extracted from NHANES surveys of children and adolescents (28,29). They demonstrate that replacement compounds like BPS are also associated with adverse effects in children.
BPA and DEHP metabolites, which were comparable to levels reported in previous studies (28,29), were associated with significantly higher urinary levels of F2-isoprostane. Our data are consistent with work by Yang et al. in which BPA was associated with increased levels of various oxidant stress markers in women (12). Oxidant stress has been implicated as mechanism of action for various BPA-associated health outcomes in children, including obesity, microalbuminuria, and increased blood pressure (30). Over the past decade, manufacturers have replaced BPA with BPS in some consumer products, resulting in increased BPS exposure. This is a cause for concern as our findings suggest that these newer substitutes may be as harmful as the ones they are replacing (31). Of note, we did not document any adverse effects of bisphenol F (BPF) exposure; however, this finding should be considered tentative in light of our limited sample size.
The 8-OHdG and F2-isoprostane are well-studied biomarkers of systemic oxidative stress and have been associated with a range of adverse health outcomes. Urinary levels of 8-OHdG and F2-isoprostane represent two distinct cellular processes. The 8-OHdG is a DNA adduct formed in the presence of excess reactive oxidative species, such as hydroxyl radicals and is indicative of DNA excision repair (32). F2-isoprostane is formed in a nonenzymatic reaction between reactive oxidative species and arachidonic acid and it is very specific for lipid oxidation. It is not affected by dietary lipid intake and is highly detectable in urine samples (33). The differences in the mechanism of formation of these two molecules may explain why studies, including ours, observe several strong associations with F2-isoprostane, compared with 8-OHdG (11). First, the level of oxidant stress induced by these environmental chemicals in children may not involve DNA damage and therefore, we are unable to identify any significant findings with 8-OHdG. Second, individuals may vary in their DNA repair capacity and this may lead to interindividual variability in urinary 8-OHdG levels.
We found that levels of HMW phthalate metabolites were associated with an increase in HOMA-IR. This is consistent with previous cross-sectional studies in adolescent NHANES participants (28,29). In contrast to previous reports, we could not confirm this relationship with insulin resistance when we analyzed DEHP metabolites (13,34,35). This may be a consequence of the modest sample size of our sample and may also reflect the fact that di-isononyl phthalate is replacing DEHP and, therefore, exposure to di-isononyl phthalate is increasing in the general population. Considering that there are few studies investigating the toxicity profiles of these newer chemicals, our results indicate the need to study the potential adverse health effects of di-isononyl phthalate.
While the mechanism(s) underlying the association of phthalates with insulin resistance are not well-understood, oxidative stress may be the missing link by inducing alterations in insulin signaling pathways. In preclinical investigations, Rajesh et al. showed that DEHP-induced production of reactive oxidative species and lipid peroxidation disrupted insulin-mediated signal transduction. These effects were mitigated if rats were supplemented with Vitamin C and E (36). Although oxidative stress and insulin resistance have been linked and oxidative stress increases with phthalate exposure (36,37), it was unclear if exposure to environmental phthalates at the community level contributes to the development of insulin resistance by inducing oxidative stress. The findings in our sample suggest that BPA and DEHP metabolites are associated with increased levels of F2-isoprostane, although the latter association fell just short of statistical significance. Metabolites of HMW phthalates are associated with body weight and increased HOMA-IR. This suggests that, at the community level, exposure to bisphenols and phthalates could induce oxidant stress, which may then contribute to development of insulin resistance in otherwise healthy children.
Oxidant stress plays a pivotal role in endothelial dysfunction and arterial stiffness. Albuminuria is an early manifestation of endothelial dysfunction. Consistent with our earlier studies using NHANES data (28,29), we documented a relationship between BPS exposure and the albumin:creatinine ratio. This suggests that childhood exposure to bisphenols may promote endothelial dysfunction, which, contributes to microvascular and atherosclerotic disease burden during adulthood. We did not detect a relationship between exposure to other bisphenols or phthalates and albuminuria, which is likely due to the limited size of our sample.
Oxidant stress-induced injury to the endothelium also contributes to arterial stiffness and subsequently to a higher risk of cardio-metabolic disease (38). We detected a relationship between exposures to DEHP metabolites and reduced brachial artery distensibility. This change may lead to an increased risk of developing large vessel disease in later life. No relationship between exposures and increased PWV were noted. This may reflect the young age of our sample and the need for prolonged exposure to the chemicals with increased oxidant stress before there are consistent changes in vascular structure and function. In addition, the environmental chemical exposures may act differently on central, large, more elastic arteries, vs. medium-size, muscular arteries that are assessed by the brachial artery distensibility test.
We measured endothelial-derived microparticles to enable a more direct localization of endothelial dysfunction and found an inverse relationship between circulating levels of activated microparticles derived from activated endothelial cells and BPS and HMW phthalates. This observation is at variance with our hypothesis that exposure to environmental chemicals may result in oxidant stress and endothelial dysfunction. The latter state would be characterized by increased release of activated endothelial microparticles. Our data points to the opposite direction but, considering that microparticles are a fairly new method of assessing the state of the endothelium, especially in children, there are gaps in our own knowledge of mechanisms of microparticles. In general, very few studies have investigated microparticles in children, and they have shown increased activation of microparticles to be associated with obesity, chronic kidney disease, and Henoch-Schonlein vasculitis (39,40,41). Our findings need to be confirmed in further studies with larger samples containing a more diverse patient population.
There are several limitations to our study, including the sample size and cross-sectional study design, which prevents us from inferring causality. In addition, reverse causation cannot be ruled out. Thus, an alternative explanation for our findings would be that insulin-resistant children have unhealthy eating behaviors, including more packaged food consumption, and thus have higher urinary levels of phthalates. In addition, we did not collect data on some potential confounders such as exposure to tobacco, which is known to affect the levels of oxidant stress.
In conclusion, our study suggests BPA and DEHP metabolites were associated with increased levels of F2-isoprostane in children, a marker of systemic oxidant stress. Metabolites of HMW phthalates are associated with higher body weight and increased risk of insulin resistance in otherwise healthy children. Exposure to BPS was associated with albuminuria and altered plasma levels of endothelial-derived microparticles. Brachial artery distensibility was reduced in association with DEHP metabolites. The evidence suggesting links between endocrine disruptors and adverse cardiorenal health effects is increasing, and our findings add to the current body of evidence. Bisphenols alter glucose transport, inhibit adiponectin release, stimulate the release of inflammatory cytokines and stimulate lipolysis in human adipose tissue (42). Phthalates simultaneously affects multiple cellular targets, and produce changes in the metabolic and oxidant stress profile of cardiac cells. In light of the emerging evidence that these persistent organic pollutants adversely impact cardiorenal function at a young age, there is a need for increased regulatory consideration and policy initiatives to limit exposure to ubiquitous environmental chemicals with the potential to increase cardiometabolic risk.
Statement of Financial Support
This work was supported by awards from the NYU CTSI (Targeted resource allocation program) grant UL1 TR001445 from the NCATS, NIH, the NYU-NIEHS Center (Pilot study program); the Immune Monitoring Core, NYU-HHC CTSI Grant; and the NYU Cancer Institute’s Cancer Center Support Grant, P30CA016087.
Disclosure:
There are no financial ties to products or potential/perceived conflicts of interest to report in the study.
References
Ebbeling CB, Pawlak DB, Ludwig DS. Childhood obesity: public-health crisis, common sense cure. Lancet 2002;360:473–82.
2008 US Environmental Protection Agency. Child-specific exposure factors handbook. National Center for Environmental Assessment. https://cfpub.epa.gov/ncea/risk/recordisplay.cfm?deid=199243&CFID=68250450&CFTOKEN=69849824.
Schecter A, Malik N, Haffner D, et al. Bisphenol A (BPA) in US food. Environ Sci Technol 2010;44:9425–30.
Carwile JL, Ye X, Zhou X, Calafat AM, Michels KB. Canned soup consumption and urinary bisphenol A: a randomized crossover trial. JAMA 2011;306:2218–20.
Fleisch AF, Sheffield PE, Chinn C, Edelstein BL, Landrigan PJ. Bisphenol A and related compounds in dental materials. Pediatrics 2010;126:760–8.
Schwartz AW, Landrigan PJ. Bisphenol A in thermal paper receipts: an opportunity for evidence-based prevention. Environ Health Perspect 2012;120:A14–5; author reply A15.
Guo Y, Kannan K. A survey of phthalates and parabens in personal care products from the United States and its implications for human exposure. Environ Sci Technol 2013;47:14442–9.
Silva MJ, Barr DB, Reidy JA, et al. Urinary levels of seven phthalate metabolites in the US population from the National Health and Nutrition Examination Survey (NHANES) 1999–2000. Environ Health Perspect 2004;112:331–8.
Wormuth M, Scheringer M, Vollenweider M, Hungerbühler K. What are the sources of exposure to eight frequently used phthalic acid esters in Europeans? Risk Anal 2006;26:803–24.
Khalil N, Ebert JR, Wang L, et al. Bisphenol A and cardiometabolic risk factors in obese children. Sci Total Environ 2014;470-471:726–32.
Ferguson KK, Loch-Caruso R, Meeker JD. Urinary phthalate metabolites in relation to biomarkers of inflammation and oxidative stress: NHANES 1999-2006. Environ Res 2011;111:718–26.
Yang YJ, Hong YC, Oh SY, et al. Bisphenol A exposure is associated with oxidative stress and inflammation in postmenopausal women. Environ Res 2009;109:797–801.
Kim JH, Park HY, Bae S, Lim YH, Hong YC. Diethylhexyl phthalates is associated with insulin resistance via oxidative stress in the elderly: a panel study. PLoS One 2013;8:e71392.
Kasahara E, Sato EF, Miyoshi M, et al. Role of oxidative stress in germ cell apoptosis induced by di(2-ethylhexyl)phthalate. Biochem J 2002;365(Pt 3):849–56.
Consumer Product Safety Improvement Act of 2008, CPSIA. Section 108. https://www.cpsc.gov/Business--Manufacturing/Business-Education/Business-Guidance/Phthalates-Information#p-2.
2013 CDC. Fourth National Report on Human Exposure to Environmental Chemicals, Updated Tables. Atlanta, GA: Centers for Disease Control.
Liao C, Liu F, Alomirah H, et al. Bisphenol S in urine from the United States and seven Asian countries: occurrence and human exposures. Environ Sci Technol 2012;46:6860–6.
Guo X, Lu X, Yang J, Kassab GS. Increased aortic stiffness elevates pulse and mean pressure and compromises endothelial function in Wistar rats. Am J Physiol Heart Circ Physiol 2014;307:H880–7.
Horstman LL, Jy W, Jimenez JJ, Ahn YS. Endothelial microparticles as markers of endothelial dysfunction. Front Biosci 2004;9:1118–35.
Asimakopoulos AG, Thomaidis NS, Kannan K. Widespread occurrence of bisphenol A diglycidyl ethers, p-hydroxybenzoic acid esters (parabens), benzophenone type-UV filters, triclosan, and triclocarban in human urine from Athens, Greece. Sci Total Environ 2014;470-471:1243–9.
Zhang Z, Alomirah H, Cho HS, et al. Urinary bisphenol A concentrations and their implications for human exposure in several Asian countries. Environ Sci Technol 2011;45:7044–50.
Haffner SM, Kennedy E, Gonzalez C, Stern MP, Miettinen H. A prospective analysis of the HOMA model. The Mexico City Diabetes Study. Diabetes Care 1996;19:1138–41.
Brar PC, Mengwall L, Franklin BH, Fierman AH. Screening obese children and adolescents for prediabetes and/or type 2 diabetes in pediatric practices: a validation study. Clin Pediatr (Phila) 2014;53:771–6.
Brinton TJ, Cotter B, Kailasam MT, et al. Development and validation of a noninvasive method to determine arterial pressure and vascular compliance. Am J Cardiol 1997;80:323–30.
Urbina EM, Kimball TR, Khoury PR, Daniels SR, Dolan LM. Increased arterial stiffness is found in adolescents with obesity or obesity-related type 2 diabetes mellitus. J Hypertens 2010;28:1692–8.
National High Blood Pressure Education Program Working Group on High Blood Pressure in Children and Adolescents. The fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescents. Pediatrics 2004;114:555–576.
Urbina EM, Dolan LM, McCoy CE, Khoury PR, Daniels SR, Kimball TR. Relationship between elevated arterial stiffness and increased left ventricular mass in adolescents and young adults. J Pediatr 2011;158:715–21.
Trasande L, Attina TM, Trachtman H. Bisphenol A exposure is associated with low-grade urinary albumin excretion in children of the United States. Kidney Int 2013;83:741–8.
Trasande L, Sathyanarayana S, Trachtman H. Dietary phthalates and low-grade albuminuria in US children and adolescents. Clin J Am Soc Nephrol 2014;9:100–9.
Kataria A, Trasande L, Trachtman H. Environmental chemicals and renal function. Nat Rev Nephrol 2015;11:610–625.
Yang CZ, Yaniger SI, Jordan VC, Klein DJ, Bittner GD. Most plastic products release estrogenic chemicals: a potential health problem that can be solved. Environ Health Perspect 2011;119:989–96.
Wu LL, Chiou CC, Chang PY, Wu JT. Urinary 8-OHdG: a marker of oxidative stress to DNA and a risk factor for cancer, atherosclerosis and diabetics. Clin Chim Acta 2004;339:1–9.
Roberts LJ, Morrow JD. Measurement of F(2)-isoprostanes as an index of oxidative stress in vivo. Free Radic Biol Med 2000;28:505–13.
Stahlhut RW, van Wijngaarden E, Dye TD, Cook S, Swan SH. Concentrations of urinary phthalate metabolites are associated with increased waist circumference and insulin resistance in adult US males. Environ Health Perspect 2007;115:876–82.
Trasande L, Spanier AJ, Sathyanarayana S, Attina TM, Blustein J. Urinary phthalates and increased insulin resistance in adolescents. Pediatrics 2013;132:e646–55.
Rajesh P, Sathish S, Srinivasan C, Selvaraj J, Balasubramanian K. Phthalate is associated with insulin resistance in adipose tissue of male rat: role of antioxidant vitamins. J Cell Biochem 2013;114:558–69.
Ferguson KK, McElrath TF, Chen YH, Mukherjee B, Meeker JD. Urinary phthalate metabolites and biomarkers of oxidative stress in pregnant women: a repeated measures analysis. Environ Health Perspect 2015;123:210–6.
Anderson TJ. Arterial stiffness or endothelial dysfunction as a surrogate marker of vascular risk. Can J Cardiol 2006;22 Suppl B:72B–80B.
Dursun I, Düsünsel R, Poyrazoglu HM, et al. Circulating endothelial microparticles in children with Henoch-Schönlein purpura; preliminary results. Rheumatol Int 2011;31:1595–600.
Dursun I, Poyrazoglu HM, Gunduz Z, et al. The relationship between circulating endothelial microparticles and arterial stiffness and atherosclerosis in children with chronic kidney disease. Nephrol Dial Transplant 2009;24:2511–8.
Gündüz Z, Dursun İ, Tülpar S, et al. Increased endothelial microparticles in obese and overweight children. J Pediatr Endocrinol Metab 2012;25:1111–7.
Gore AC. Endocrine-disrupting chemicals. JAMA Intern Med 2016;176:1705–6.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Kataria, A., Levine, D., Wertenteil, S. et al. Exposure to bisphenols and phthalates and association with oxidant stress, insulin resistance, and endothelial dysfunction in children. Pediatr Res 81, 857–864 (2017). https://doi.org/10.1038/pr.2017.16
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/pr.2017.16
This article is cited by
-
Resveratrol, Endocrine Disrupting Chemicals, Neurodegenerative Diseases and Depression: Genes, Transcription Factors, microRNAs, and Sponges Involved
Neurochemical Research (2023)
-
Association of urinary bisphenols with thyroid function in the general population: a cross-sectional study of an industrial park in China
Environmental Science and Pollution Research (2023)
-
Biodegradation of phthalates and metabolic pathways: an overview
Environmental Sustainability (2023)
-
Association of urine phthalate metabolites, bisphenol A levels and serum electrolytes with 24-h blood pressure profile in adolescents
BMC Nephrology (2022)
-
The association of phthalate metabolites with childhood waist circumference and abdominal obesity
European Journal of Pediatrics (2022)
