
Key Points
-
Mandibular first molar root fillings have low failure rates over a five-year period.
-
Failure is most likely to occur in the first year following placement of the root filling.
-
Failure rates are similar for optimal versus sub-optimal appearance of root-fillings on radiographs.
-
Coronal restoration is an important predictor of survival with crowns performing better than plastic restorations.
Abstract
Objective To describe the quality and record the outcomes of root canal therapy on mandibular, first permanent molar teeth provided by GDPs working according to NHS contracts.
Design Descriptive, retrospective cohort study.
Setting Twelve general dental practices in Salford, North West England.
Subjects and method All patients aged 20-60 years attending the practices who had received a NHS-funded root filling in a mandibular first permanent molar between January 1998 and December 2003. The radiographic quality of root fillings in the teeth was assessed by an endodontic specialist and categorised into optimal, suboptimal and teeth which had no radiograph, or an unreadable radiograph. Teeth were also dichotomised into those restored with a crown and those restored with an intracoronal restoration. Failure as an outcome was defined as if a tooth was extracted, the root filling was replaced or periradicular surgery was performed on the tooth. Crude failure rates per 100 years were calculated for optimally, sub-optimally root filled teeth and for those with no or an unreadable radiograph, and according to how the tooth was coronally restored. Survival was assessed using Kaplan-Meier curves and Cox proportional hazards were used to determine factors linked with increased failures.
Results One hundred and seventy-four teeth were included in the study, of which 16 failed. The crude failure rates per 100 years with a root filled tooth were very low and differed little (p = 0.9699) for optimally (2.6), sub-optimally (2.5) root filled teeth and for those with no or an unreadable radiograph (2.9), with approximately one in 37 root filled mandibular first molar teeth failing each year. The majority of root fillings fail within the first two years (N = 10, 62.5%). Some 67 teeth (38.5%) were restored with a crown, none of which failed during the follow up period compared to those with a plastic restoration (p = 0.0004).
Conclusions The very low failure rates have significant implications for the design of research studies investigating outcomes of endodontic therapy. The similar failure rates for teeth that had optimal and suboptimal root fillings suggest that endodontic treatment is not as technique sensitive as previously thought. The results also support the notion that the coronal restoration is more important than radiographic appearance of the root filling.
Similar content being viewed by others
Introduction
In the UK endodontics has been recognised as a dental specialty since 1994.1 Over the last ten years there has been a growth in the number of specialist endodontic practices, many of which provide treatment on a private basis. However, the NHS remains the major provider of endodontic treatment; for example, in England in 2003 more than 800,000 endodontic treatments were provided by the NHS general dental practitioners (GDPs) at a cost of over £43 million.2 This represents a substantial amount of NHS resource dedicated to this type of treatment; yet we have little information on the outcomes of endodontic therapy delivered by GDPs.
Reviewing the outcomes of endodontic therapy in the literature is difficult as outcome measures are not standardised. The literature includes studies that report a range of different outcomes including radiological assessment, functionality of treated teeth and presence of signs and symptoms. In the USA a large epidemiological study of care provided by dentists participating in insurance plans3 reported that over 95% of teeth were retained in the oral cavity eight years after initial endodontic treatment. However, population-based studies4 suggest a higher failure rate, nearer 20%, than reported from studies of insured populations. In the UK we have no published longitudinal studies measuring outcomes of endodontic care provided by GDPs. Two studies have reported outcomes achieved by different services in the UK, for example Peak et al.5 in a study of endodontic care provided by Royal Air Force dentists reported that 88% of root fillings placed less than 2 mm from the apex had successful outcomes, but overfilled teeth had a slightly lower success rate (75%) than underfilled teeth (78%). Smith et al.6 in a study of patients attending the Eastman Dental Hospital reported similar figures with 87% success rate for root fillings placed less than 2 mm from the apex, 75% for those teeth root fillings beyond the apex and 77% for those teeth with short root fillings. A meta-analysis by Schaeffer et al.7 concluded that a better success rate is achieved when obturation is short of the apex rather than beyond the apex.
Although these results are interesting, they perhaps do not provide a comprehensive view of the outcomes of endodontic treatment. Recent literature suggests that the coronal restoration of root filled teeth is perhaps more important than the radiographic appearance of the root filling. Some studies have intimated that crowned root-filled teeth have better outcomes or survive longer than those with intra-coronal restorations.8,9,10 However, none of these studies have taken place in general dental practice and the results reported may not be representative of the outcomes of care delivered by general dental practitioners (GDPs).
To summarise, we have a situation in which large amounts of NHS resources are consumed in providing endodontic treatment and yet we have no information on the outcomes of this treatment. If we are to pursue an evidence-based approach to the provision of dental care, providing information on the outcomes of treatment provided by GDPs is a vital first step in this process.
The aim of this study was to describe the quality and record the outcomes of root canal therapy on mandibular, first permanent molar teeth provided by GDPs working according to NHS contracts. The objectives were to:
-
describe the technical quality and outcomes of the root fillings placed by GDPs in mandibular, first permanent molar teeth
-
calculate the crude failure rate in optimal and sub-optimal root fillings in mandibular first permanent molar teeth
-
calculate the crude failure rate in root filled mandibular first molars that were subsequently crowned and in those teeth which had been restored by other means.
Methods
A descriptive, retrospective cohort study design was used. The study inclusion criteria for participants were:
-
all patients aged 20-60 years attending 12 dental practices in Salford in the North West of England
-
who had received a NHS root filling in a left or right mandibular first permanent molar between January 1998 and December 2003.
Mandibular first permanent molar teeth were chosen for two reasons; first they are multi-rooted and are therefore more technically difficult to root fill than teeth with single root canals. Due to the technical difficulty, it was assumed that these teeth would produce adequate numbers of failures and sub-optimally root filled teeth to include in analyses. The second reason concerned outcome measurement; due to the anatomy of these teeth radiographs are easier to read than radiographs of, for example, maxillary permanent molar teeth.
Relevant ethical committee and research governance committee approval was obtained prior to commencement of the study. All dentists in Salford were invited to participate, but in order to be included in the study dentists had to have been practising on the same site for more than five years prior to January 2006 when data collection started. This was to ensure there was adequate follow up time for their patients. Additionally dentists included in the study must have been routinely providing molar endodontics according to NHS General Dental Service regulations during the period January 1998 to December 2003.
Each participating dentist sent a letter to the Dental Practice Board (DPB) requesting a list of their patients aged between 20-60 years who had received a root filling in a left or right mandibular first permanent molar between January 1998 and December 2003. A consent letter was sent from the dentists to their patients identified on the list, asking for permission to review and copy their dental records and take a copy of radiographs of their root filled teeth.
A research assistant visited all practices and photocopied the clinical notes of all participants using a portable photocopier. Post-operative periapical radiographs of the mandibular first permanent root filled molar teeth were copied using a high quality digital scanner. A trained dental nurse examined the photocopied case notes of participants and transcribed the date of placement of the root filling and the outcomes of the root filled teeth onto a data abstraction form. Failure of a root filing was defined as:
-
extraction of the tooth
-
replacement of the root filling
-
periradicular surgery performed on the tooth
in the period between placement of the root filling in January 1998 to December 2003 and the data collection period, which was January to March 2006. This was the date when the root filling was undertaken and the date of the outcome was recorded. For failed root fillings the outcome date was recorded as the date when a tooth was extracted, or the root filling was replaced or periradicular surgery was performed. A successful outcome was categorised as a tooth that was still present in the mouth and symptomless at the last visit recorded in the dental notes. The date of this last visit was recorded as the outcome date.
In a separate exercise, a single endodontic specialist (AQ) assessed all available radiographs of the root filled teeth and categorised the quality of the root fillings as being optimal or sub-optimal. Root fillings judged to be optimal were those which satisfied the Consensus Report of the European Society of Endodontology on quality guidelines for endodontic treatment.11 All other root fillings were categorised as sub-optimal. The teeth that did not have a radiograph or one that was unreadable were also recorded. The specialist was blinded to the outcomes of the root filled teeth. Radiographic appearance of the periapical areas of root-filled teeth was not used to assess outcomes, as the presence of radiolucencies is not diagnostic of active pathology. Data on outcomes and assessment of root filling quality were not attributed to individual dentists.
Data were entered onto a computer for analyses. Outcome measures were used to dichotomise the population of teeth into failed (the tooth being either extracted, the root filling replaced or periradicular surgery performed) or successful (the tooth present and symptomless in the mouth at the participant's last visit recorded in the dental notes). Teeth were also categorised in two ways:
-
1
Into three groups according to the status of the root filling:
-
optimally root filled
-
sub-optimally root filled
-
unavailable or unreadable radiograph
-
-
2
Into two groups depending on the type of restoration placed subsequent to root filling namely:
-
a crown
-
intra-coronal, plastic restoration.
-
Statistical analysis
A frequency distribution of failures by the number of years since the root filling was placed was calculated. Crude failure rates were determined, first for teeth according to their root filling status and then according to how the tooth was coronally restored. These calculations were performed by first identifying the number of person years with a root filled tooth, counted from the date the root filling was performed to the outcome date, either when the definition of failure was recorded in the participant's notes or, for those participants whose root filling was defined as successful, on the last recorded dental appointment. The crude failure rate was calculated by dividing the total number of failure events by the total number of years with a root filled tooth in each category. Crude failure rates per 100 years were calculated to enable like for like comparisons between the quality of the root filling and the type of coronal restoration. Finally, survival was assessed using Kaplan-Meier curves and Cox proportional hazards were used to determine factors linked with increased failures. Statistical differences between the subgroups were determined using log rank tests. All analyses were performed in SPSS (version 13.0) and STATA (version 8.0).
Results
All 94 dentists whose NHS contract was held by Salford Primary Care Trust were contacted and invited to participate in the study. Table 1 provides a breakdown of the responses obtained from the dentists. Over half of the dentists indicated that they would like to participate in the study, but only 12 (12.8%) of these were eligible for inclusion. The Dental Practice Board identified 315 patients of these 12 dentists who met the inclusion criteria. In total 196 (62%) patients responded and provided written consent to be included in the study. Of these subjects, case notes could not be found for 21 individuals and one patient failed to complete their root filling treatment and was excluded from the analyses, leaving 174 root filled first permanent molar teeth in 174 patients forming the study population.
The study population were made up of 76 (43.7%) male subjects and 98 (56.3%) females, with a mean age of 49.2 years (SD 10.3) on 31 March 2006. There was a range of years from placement of the root filling to outcome measurement was 0-7.7 years, with a mean of 3.5 (SD 3.5) years. Of the teeth included in the study 93 (53.4%) were mandibular left first permanent molars and 81 (46.6%) were mandibular right first permanent molars. Similar failure rates occurred for left and right teeth. In total less than 10% (n = 16) of all root filled teeth failed during the follow up period. Figure 1 shows a frequency distribution of endodontic failures in the mandibular first permanent molars in the population over a five-year period, half of root filling failures occurred within the first year after placement of the root filling. Of the 16 failures, 15 teeth were extracted and in one tooth the root filling was replaced.

Endodontic failures in mandibular first permanent molars over a five year period
Table 2 presents the crude rates for failure of root-filled teeth according to an assessment of the quality of the root filling, as well as the rate for those teeth for which a readable radiograph was not available. Approximately one quarter of teeth (n = 46, 26.6%) were judged to have been root filled to an optimal standard, whereas 38.2% (n = 66) of root fillings were considered to be sub-optimal. Just over one third of teeth (n = 61, 35.3%) had no post-operative radiograph or the radiograph available was unreadable by the specialist endodontist. The most surprising finding was that virtually the same proportions of teeth failed in those categorised as having optimal (8.7%) or sub optimal root fillings (9.1%) and in those teeth with no film or an unreadable film (9.8%). The rates take into account the different number of root filled tooth years within each group, and again showed that the outcomes in each group were very similar, with approximately one in 37 root filled mandibular first molar teeth failing each year. These results were also supported by a survival analysis (Fig. 2) which showed that there was no statistically significant difference (p = 0.9699 log rank test) in probability of failure between optimal and sub-optimal root-fillings.

Overall, there was no difference in survival based on the quality of root filling (log rank test 0.06, df = 2, p = 0.9699)
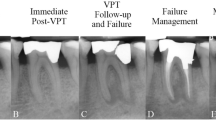
Table 3 summarises the outcomes of root filled teeth according to how each tooth was coronally restored. The difference in outcomes was stark; 67 (38.5 %) of teeth were restored with a crown and all of these teeth were present and symptomless at outcome measurement. The failure rate for teeth restored with an intracoronal restoration was still low at five failures per 100 root filled tooth years; meaning that one in 20 mandibular first molar root fillings restored with an intracoronal plastic restoration will fail each year. These results were again supported by a survival analysis (Fig. 3) which showed that there was a strong statistical difference (p = 0.0004 log rank test) in probability of failure between crowned and uncrowned root filled teeth.

Overall, survival was much better with a crown than a plastic restoration (log rank test 12.64, df = 1, p = 0.0004)
Further analyses were undertaken to determine if crown restorations were only placed on optimally root-filled teeth. These analyses revealed that 44.8% of crowned teeth were judged to be sub-optimally root filled (n = 30), 20.9% (n = 14) were optimally root filled and the remaining 23 crowned teeth (34.3%) had no or an unreadable radiograph.
Discussion
This is the first study to report the outcomes of NHS-funded molar endodontic treatment provided by GDPs. The study was conducted during a period when NHS GDPs were working to the 1990 GDS contract and endodontic care for adults was remunerated according to a fee for item system. When this system of remuneration was operating there were some concerns that the GDS fee for molar root treatment was insufficient to adequately reimburse dentists for the time taken to provide this complex form of therapy to a high standard. This fear seems to have been unwarranted, as this study shows that the quality of the root filling had little impact on outcomes.
The findings of this study have important implications for the provision of endodontic care and for dental education and training. Several fundamental questions arise from the results. If the majority of root filled teeth survive irrespective of whether or not a textbook-standard root filling is achieved, to what extent is it necessary to strive towards the ideal? Another important issue is raised by the finding that root filled teeth, which had no, or an unreadable post-operative radiograph, had similar outcomes as those teeth that had radiographs. Current guidance issued by the Faculty of General Dental Practitioners12 recommends all teeth should have radiographs taken immediately following obturation, with a further follow up radiograph to assess (radiographic) healing after one year and then annually until (radiographically judged) healing occurs. This and other studies13 demonstrate that most failures occur in the first year after obturation and that long term failure is rare, weakening the arguments for long term routine follow up radiographs. The outcomes measures used in this study did not include a radiographic assessment of the periapical area at outcome. An unequivocal, pragmatic approach to outcome measurement was used. GDPs are unlikely to extract teeth or replace a root filling unless the patient is experiencing recurrent and severe symptoms, and so the outcome measure used is most relevant to primary care practitioners and, importantly, to patients. There is a growing body of opinion that argues that subjective outcome measures, such as pain, are more important for patients than professionally assessed outcome measures.14,15,16 It is clear that a more lucid understanding of the relationship between radiographically judged pathology and subjectively assessed (patient judged) success of endodontic therapy is required. This information should be supplemented by a greater insight to the full costs and benefits of taking routine outcome radiographs to inform the future development of guidelines.
This study strongly suggests that root-filled teeth that were restored with crowns have a lower risk of failure than those with intra-coronal restorations. There were concerns that this outcome could be due to selection bias – dentists only crowning optimally root-filled teeth and therefore influencing the outcome. However, in this study dentists crowned more sub-optimally root filled teeth and teeth with no, or an unreadable radiograph than optimally root filled teeth, therefore this source of bias was unlikely. Better outcomes for crowned teeth have been reported by animal experiments8 and in community studies,3 and supports the hypothesis that the coronal restoration is more important than the radiographic appearance in determining the success of root filled teeth. One could argue that tooth fracture is more common in root filled teeth with intra-coronal restorations, and this rather than failure of the root-filling increased the risk of extraction in this group. However, the causes of failure are immaterial to the patient as the outcome has the same consequences: pain and extraction.
These findings indicate that endodontic treatment may not be as technique sensitive as previously thought and the coronal restoration of root filled teeth is more important than the perceived quality of the root filling. This is an important topic for the NHS, as the demand for endodontic care is likely to rise due to an ageing population with heavily restored dentitions17 that is reticent to having extractions.17 The findings are important to inform the conduct of future research in endodontics. This study was preliminary in nature and hypothesis generating rather than hypothesis testing. There are concerns about external validity of any study performed in general practice, as GDPs participating in practice-based studies are self-selecting. Ideally, multiple prospective cohort studies in different populations, measuring both the subjectively and radiologically assessed outcomes of root filled teeth should be undertaken to shed further light on the issues raised by this study. However, as the failure rates are very low, and similar in optimally and sub-optimally root filled teeth, this would mean that such studies would require very large sample sizes, particularly if the aim is to demonstrate equivalence. One beneficial finding of this study for future research design and management is that shorter-term follow up is appropriate, as the majority of root fillings fail within the first two years.
In conclusion this study reported low crude failure rates of mandibular first molar root fillings and very similar rates for teeth which had optimal and suboptimal root fillings. The results also support the notion that the coronal restoration is more important than radiographic appearance of root fillings. Restoration with a crown may imply a lower risk of post-operative tooth fracture and better coronal seal although this needs further investigation. The failure rates reported here are important to inform the power calculations and conduct of future studies.
References
Department of Health Training for Dental Specialists in the Future Department of Health, London (1994)
NHS Business Services Authority Dental Practice Division Digest of Statistics March 1997 to March 2003 http://www.dpb.nhs.uk/
Salehrabi R, Rotstein I . Endodontic treatment outcomes in a large patient population in the USA: an epidemiological study. J Endod 2004; 30: 846–850.
Tilashalski K R, Gilbert G H, Boykin M J, Shelton B J . Root canal treatment in a population-based adult sample: status of teeth after endodontic treatment. J Endod 2004; 30: 577–581.
Peak J D, Hayes S J, Bryant S T, Dummer P M . The outcome of root canal treatment. A retrospective study within the armed forces (Royal Air Force). Br Dent J 2001; 190: 140–144.
Smith C S, Setchell D J, Harty F J . Factors influencing the success of conventional root canal therapy-a five-year retrospective study. Int Endod J 1993; 26: 321–333.
Schaeffer M A, White R R, Walton R E . Determining the optimal obturation length: a meta-analysis of literature. J Endod 2005; 31: 271–274.
Sabeti M A, Nekofar M, Motahhary P, Ghandi M, Simon J H . Healing of apical periodontitis after endodontic treatment with and without obturation in dogs. J Endod 2006; 32: 628–633.
Teixeira F B . Ideal obturation using synthetic root-filling systems: coronal sealing and fracture resistance. Pract Proced Aesthet Dent 2006; 18: S7–S11.
Sritharan A . Discuss that the coronal seal is more important than the apical seal for endodontic success. Aust Endod J 2002; 28: 112–115.
Consensus Report of the European Society of Endodontology on quality guidelines for endodontic treatment Int Endod J 1994; 27: 115–124.
Faculty of General Dental Practitioners, Royal College of Surgeons of England. Selection criteria for dental radiography, 2nd ed. Pendlebury M E, Horner K, Eaton K A (eds). London: Royal College of Surgeons of England, 2004.
Orstavik D . Time-course and risk analyses of the development and healing of chronic apical periodontitis in man. Int Endod J 1996; 29: 150–155.
Kay E J . Risks and values in treatment decision making. Primary Dent Care 2001; 8: 105–109.
Sullivan M . The new subjective medicine: taking the patient's point of view on health care and health. Soc Sci Med 2003; 56: 1595–1604.
Marshall S, Haywood K, Fitzpatrick R . Impact of patient-reported outcome measures on routine practice: a structured review. J Eval Clin Pract 2006; 12: 559–568.
Kelly M, Steele J, Nuttall N et al. Adult dental health survey: oral health in the United Kingdom 1998. London: The Stationery Office, 2000.
Acknowledgements
The authors would like to thank Dr Fiona Blinkhorn and Louise Morris of Salford PCT and the GDPs who participated in the study.
Author information
Authors and Affiliations
Corresponding author
Additional information
Refereed paper
Rights and permissions
About this article
Cite this article
Tickle, M., Milsom, K., Qualtrough, A. et al. The failure rate of NHS funded molar endodontic treatment delivered in general dental practice. Br Dent J 204, E8 (2008). https://doi.org/10.1038/bdj.2008.133
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/bdj.2008.133
This article is cited by
-
A protocol for the Development of Core Outcome Sets for Endodontic Treatment modalities (COSET): an international consensus process
Trials (2021)
-
Novel tier 2 service model for complex NHS endodontics
British Dental Journal (2021)
-
Feasibility of assessing training of primary care dental practitioners in endodontics of moderate complexity: mapping process and learning
British Dental Journal (2018)
-
Assessing a training programme for primary care dental practitioners in endodontics of moderate complexity: Pilot data on skills enhancement and treatment outcomes
British Dental Journal (2018)
-
Blatant ignorance
British Dental Journal (2016)
