



There are currently no safe and effective approved medications for behavioral and psychological symptoms of dementia (BPSD). Cannabidiol (CBD), a non-intoxicating cannabinoid, with anti-anxiety and anti-psychotic properties shows promise (Bhattacharyya et al., Reference Bhattacharyya, Wilson, Appiah-Kusi, O’Neill, Brammer, Perez, Murray, Allen, Bossong and McGuire2018; McGuire et al., Reference McGuire, Robson, Cubala, Vasile, Morrison, Barron, Taylor and Wright2018; O’Neill et al., Reference O’Neill, Wilson, Blest-Hopley, Annibale, Colizzi, Brammer, Giampietro and Bhattacharyya2020), with evidence of good tolerability and acceptability of formulations containing CBD alone, as opposed to those containing delta-9-tetrahydrocannabinol, a cannabinoid with psychotomimetic effects (Velayudhan et al., Reference Velayudhan, McGoohan and Bhattacharyya2021a; Velayudhan et al., Reference Velayudhan, McGoohan and Bhattacharyya2021b).
To evaluate the feasibility and obtain preliminary evidence in support of a future fully powered efficacy trial of CBD, we carried out a phase 2a, single-site, parallel-group, double-blind, placebo-controlled, randomized trial in patients with Alzheimer’s disease (AD) and BPSD (EudraCT Number - 2019-002106-52). Participants of either sex aged 55 years or older with possible or probable AD (McKhann et al., Reference McKhann, Drachman, Folstein, Katzman, Price and Stadlan1984) were eligible, if they had BPSD with total score on Neuropsychiatric Inventory (NPI) (Cummings, Reference Cummings1997) ≥4 and at least 1 item with score of 2 or more (frequency × severity) on one of the domains of anxiety, agitation, hallucinations, or delusions. The primary endpoints were acceptability, adherence to treatment, and retention rates from baseline to week 6, while secondary outcomes included safety/tolerability and clinical and cognitive measures (more details in Supplementary Methods). Ethical approval was obtained from the NHS Health Research Authority (20/EE/0014) and regulatory approval from the Medicines and Healthcare products Regulatory Agency, UK. Written informed consent from participants or their legally authorized representative was obtained.
Between May 20, 2021, and March 4, 2022, 22 participants were screened, 16 of whom were randomly assigned and 15 received treatment (n = 8 CBD and n = 7 placebo) (Figure 1). One of the 16 randomized patients dropped out immediately after randomization before starting treatment. In total, 93% were females, mean age of 77.91 years (±8.08), and two were from Afro-Caribbean ethnicity with the rest White Caucasians. Participants were randomly assigned to receive either oral capsules of CBD (200 mg) or placebo, starting with one capsule/day and titrated upwards to 3 capsules/day (see Supplementary Methods). The two treatment groups were mostly comparable in terms of baseline sociodemographic and clinical characteristics, except that placebo-treated patients had more severe delusions and better quality of life at baseline (Supplementary Table 1).
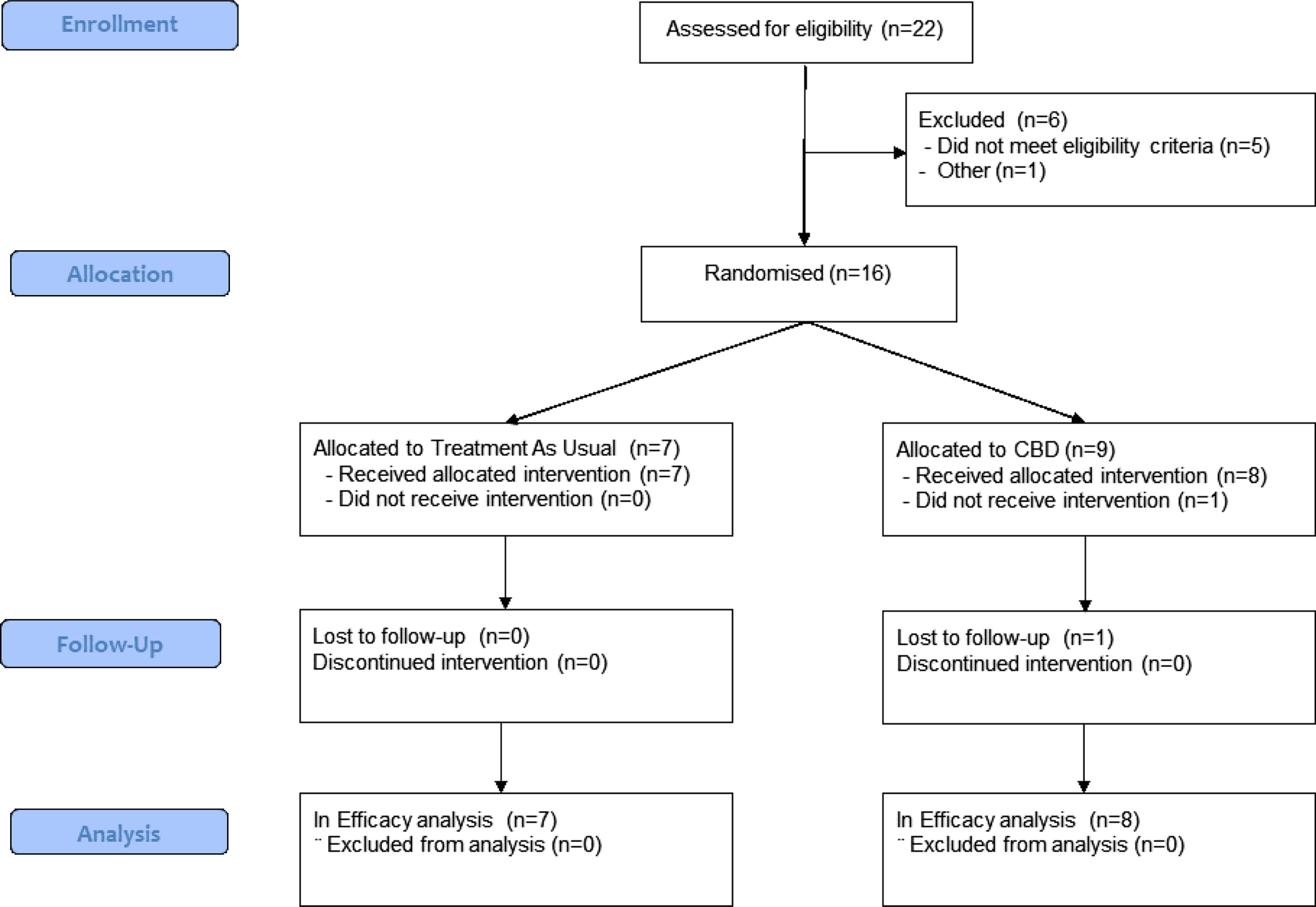
Figure 1. CONSORT diagram.
Overall, adherence to study treatment was 100% (95% confidence interval, CI: 78–100%) and retention rate was 94% (95% CI: 70–100%). A total of 34 adverse events (AEs) were observed during the entire period of the study (Supplementary Results and Table 2), most common being dizziness (CBD: 63%; placebo: 0%); and falls (CBD: 25%; placebo: 43%). There were no withdrawals or deaths in either group. There was one serious AE of a fall experienced by a participant in the placebo group after the end of treatment. Improvement on NPI-clinician rating scale (de Medeiros et al., Reference de Medeiros, Robert, Gauthier, Stella, Politis, Leoutsakos, Taragano, Kremer, Brugnolo, Porsteinsson, Geda, Brodaty, Gazdag, Cummings and Lyketsos2010) was observed for total score (mean ± SD of change from baseline; CBD: −29.86 ± 51.50; Placebo: −10.14 ± 38.15) and for hallucinations, anxiety, agitation, apathy/indifference, and irritability/lability domains along with caregiver distress in CBD-treated compared to placebo-treated participants (Supplementary Table 3). Such a change was not seen for delusions, perhaps because severity of delusions was lower in CBD-treated patients to start with.
Our study showed good acceptability, compliance, and retention. The tolerability and safety profile of CBD were consistent with previous reports (Velayudhan et al., Reference Velayudhan, McGoohan and Bhattacharyya2021a) and naturalistic evidence (Tumati et al., Reference Tumati, Lanctôt, Wang, Li, Davis and Herrmann2022) with mild and transient treatment-related dizziness, somnolence, and increased liver enzymes being the most common. Increased levels of liver enzymes have been known with CBD, though evidence in older adults has been limited (Velayudhan et al., Reference Velayudhan, McGoohan and Bhattacharyya2021a). Hence, it is interesting to observe this AE in our study which needs monitoring in future trials.
Preliminary potential effect that CBD may be useful in BPSD domains such as apathy, one of the most prevalent BPSD across the spectrum of neurocognitive disorders and associated with worse clinical outcomes (Mortby et al., Reference Mortby, Adler, Agüera-Ortiz, Bateman, Brodaty, Cantillon, Geda, Ismail, Lanctôt, Marshall, Padala, Politis, Rosenberg, Siarkos, Sultzer and Theleritis2022; Velayudhan, Reference Velayudhan2023), or agitation, an area of considerable unmet treatment need in AD, suggest promising intervention targets.
However, it is worth noting that the study was not powered to demonstrate clinical efficacy through hypothesis testing. The sample size was much smaller than originally intended due to the challenges posed by the COVID-19 pandemic. Nevertheless, the preliminary demonstration of safety and tolerability; acceptability; adherence to treatment; and signals of potential effect across a range of unmet treatment targets such as apathy, anxiety/agitation, and hallucinations is promising. Recruitment and retention during the COVID-19 pandemic of a frail population with moderate-to-severe AD are particularly encouraging.
Collectively, they support the case for pivotal studies to evaluate the efficacy of CBD for behavior symptoms in people with AD.
Conflicts of interest
LV, SB, and DA are in receipt of funding from Parkinson’s UK and Alzheimer’s Research UK. The funding source had no involvement in this research. LV and SB have collaborated with Beckley Canopy Therapeutics/Canopy Growth (investigator-initiated research) wherein they supplied study drug for free for charity-funded research. SB is supported by grants from the National Institute of Health Research (NIHR) Efficacy and Mechanism Evaluation scheme. SB has participated in advisory boards for or received honoraria as a speaker from Reckitt Benckiser, EmpowerPharm/SanteCannabis and Britannia Pharmaceuticals. DA has received research support and/or honoraria from Astra-Zeneca, H. Lundbeck, Novartis Pharmaceuticals, Evonik, Roche Diagnostics, and GE Health, Sanofi, and served as paid consultant for H. Lundbeck, Eisai, Heptares, Eli Lilly, Enterin, Acadia, EIP Pharma, Biogen, and Takeda. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR, or the Department of Health.
Source of funding
Funding to conduct the trial was provided by King’s Health Partners Research & Development Challenge Funds (Project 659553/ RE14738), Psychiatry Research Trust (Project 586662/ RE15411), and Rosetrees Trust (Project 593627/ RE16047). Funders had no role in the design or conduct of the study. The views expressed are those of the authors and not necessarily those of the funders.
Description of author(s)’ roles
LV conceived and designed the study, obtained funding, supervised the study, and wrote the manuscript. SB participated in study design, obtaining funding, review, and revision of the manuscript. MD, SP, LV, SB, and LH contributed to patient recruitment and evaluation, and have verified the underlying data. MD, SP, and LH participated in review and revision of the final report. DA participated in obtaining funding, review, and revision of the final report. PB assisted with statistical analysis and review and revision of the report.
Acknowledgments
We would like to thank Glynis Ivin and Michael Welds at South London and Maudsley NHS trust Pharmacy for their invaluable support. We would also like to thank Dr Suresh Kallur, Dr Abimbole Fadipe, and Prof Ruth Pickering for their role as members of the Independent Data Monitoring Committee.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S1041610224000516.



